Acne vulgaris is a chronic inflammatory disease of Pilosebaceous glands. It is believed to be the most common disease of skin affecting more than 80% of adolescents [1] and is the leading reason for visits to dermatologists. Adolescence is a line of physical, emotional and social development. They are the representative of the general population of individuals with acne, the prevalence of which peaks between 12 –18 years [2]. The most severe forms of acne vulgaris occur more frequently in males, but the disease tends to be more persistent in females [3]. A report in the BMJ in 1989 opined that in a life time a person is more likely to have acne than any other disease [4]. The levels of social, psychological and emotional impairments in acne is comparable with chronic diseases such as asthma, epilepsy, diabetes and arthritis. Besides anxiety and depression acne patients are prone to low self esteem, low self confidence, low self assertiveness, embarrassment, social inhibition, affection, shame, altered body image, psychosomatic symptoms, obsessive compulsiveness and suicidal tendencies [3,5]. It can be negatively associated with intention to participate in sports and exercise. Patients with acne have higher unemployment rates compared to patients without acne [6]. Assessing the impact of acne on quality of life requires well-validated and reliable measures of acne specific quality of life that are brief and easy to administer and interpret [7]. Several acne-specific health related quality of life (HRQOL) instruments now exist, including the Assessment of the psychological and social effects of acne (APSEA), the acne disability index (ADI), the Cardiff acne disability index (CADI) and the dermatology-specific quality of life (DSQL) questionnaire [8]. There are very few studies on, impact of acne on QOL in Indian populations [9–12]. Keeping this thing in mind a study was under taken with the aim: (a) to measure the physical, psychological and social impact of Acne, in turn determine the Quality of Life; (b) Compare impact of acne in male and female patients; and (c) Perceptions of acne among non-sufferers.
Materials and Methods
The prospective, cross-sectional, prestructured, questionnaire-based study was conducted from March 2012 to February 2013 at rural based tertiary care centre. The Human Research Ethical Committee of the Institute had approved the study protocol. The study population comprised of candidates of both sexes of ages between 14–25 years attending skin OPD, with or without acne. Patients having any chronic cutaneous disorders or systemic disorders like asthma, DM, epilepsy, HIV patients and patients on any systemic therapy were excluded from study. The subjects were well informed about the project and informed consent was obtained from all participants and they were assured that their participation is voluntary and their responses would be kept confidential. Patients with grade1 and grade 2 acne vulgaris were included and were subjected to a self-administered, 15 point questionnaire for acne sufferers. DLQI is a general questionnaire for evaluation of quality of life in dermatology patients and consists of 10 questions about disease symptoms, feelings, daily activities, type of clothing, social or physical activities, exercise, job or education, interpersonal relationships, marriage relationships and treatment [13]. CADI is a questionnaire which is specific for acne and contains 5 questions related to the last month about feelings, interference with social life and interaction with the opposite gender, avoidance of public places, appearance of the skin and perceived severity of disease state [14].
Perception of acne among non acne sufferers were evaluated on the basis of three questions i.e., whether they consider acne as a problem, disturbed by the idea of having acne, and whether acne is an obstacle in making friends.
The intensity and frequency of symptoms is evaluated on a 4- point Likert scale (range 0-3) [15]. Other individual of same age and sex not having acne were subjected to 3 point questionnaire as for non-acne sufferers and were scored on a 3 point scale of -1, 0, and 1. Other variables included for patients with acne were skin type (dry/oily) as given history by patient, undergoing treatment for acne or not, If undergoing treatment what kind of treatment and if not why.
Statistical Analysis
The data was entered into Excel 2010 and coded into numerical score. Statistical Calculation were done in Excel 2010 and using Statgraphics Centurion XVI.I. The descriptive statistics were done for each variable. Categorical data were expressed as frequencies and percentages. Continuous data were expressed as means and standard deviations. Cross-tabulation was used with Chi square test, p-value determination. The level of significance was set at p < 0.05.
Scoring of 15 Point Questionnaire in Acne Sufferers
If more than 2 questions were not answered, it was not included in the study, the data considered as missing.
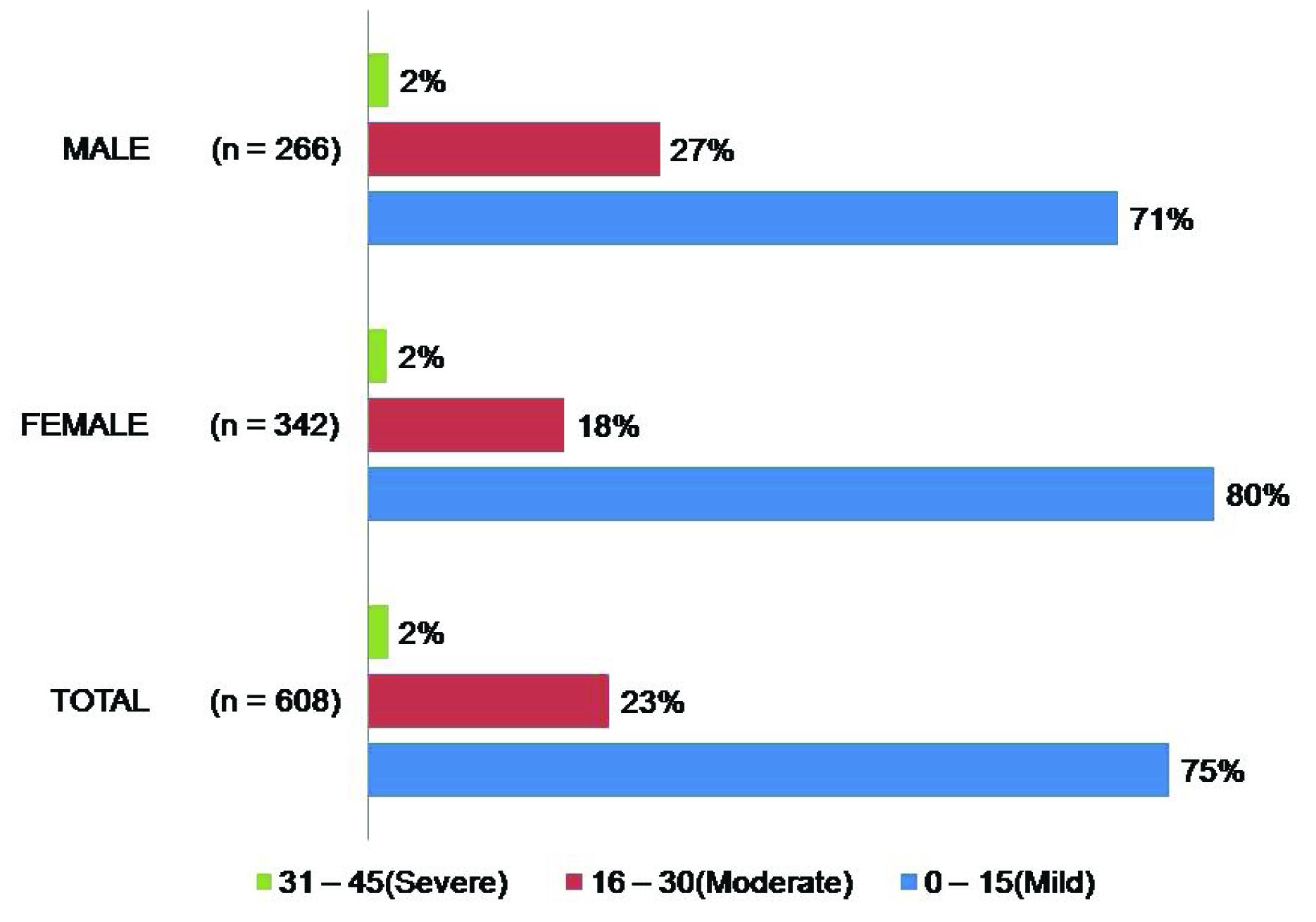
1. Total Acne Quality of Life (TAQOL): Total score is calculated by summing the score of each 15 question resulting in a possible maximum of 45 and minimum of 0. The higher the score, the more the quality of life is impaired. A score of 0-15 translates to mild quality of life impairment, 16-30 indicates moderate impairment, and 31-45 demonstrates severe impairment [Table/Fig-1].
| QOL Impairment | Total Score(TAQOL) | VocationalScore(VQOL) | Severity Score |
|---|
| Mild | 0 – 15 | 0 – 2 | 0 - 3 |
| Moderate | 16 – 30 | 3 – 4 | 4 - 6 |
| Severe | 31 – 45 | 5 – 6 | 7 - 9 |
Scoring of 3 Point Questionnaire for Perception of Acne among Non-acne Sufferers
The three questions is scored on a three point scale -1 (No), 0 (May Be), +1 (Yes), with a minimum score of -3 and maximum score +3. A score of – 3 for Acne is not a problem, and +3 for Acne is a problem and can affect one’s life.
Results
Total 888 participants had volunteered for the self-administered questionnaire, of which 19 were considered as missing, for not answering more than two questions. The age group of the participants was 14-25 years, mean ± standard deviation (SD) age was 19.82± 2.20 years. Of the total of 869 data included in the study, 523 (60.18%) were females and 346 males (39.82%), 624 (71.80%) were in the age group 18-21 [Table/Fig-2]. Of the 869 individuals 608(69.97%) had acne while 261(30.03%) had no acne. 48 (5.52%) were employed and the rest 94.48% were students. All the 48 employed individuals were acne sufferers.
Demographic details of the participants
| ACNE (n) 608 (69.97%) | NO ACNE (n) 261 (30.03%) | TOTAL (n) 869 | p-value | Odds ratio | 95% CI |
|---|
| Male | Female | | Male | Female |
|---|
| Gender | | 266 (43.75%) | 342 (56.25) | | 80 (30.65%) | 181 (69.35%) | | 0.0003 | 0.5682 | 0.4175 –0.7233 |
| 14 – 17 YRS | 65 (10.69%) | 31 | 34 | 11 (4.21%) | 3 | 8 | 76 (8.75%) | 0.0018 | | |
| 18 – 21 | 413 (67.93%) | 171 | 242 | 211 (80.84%) | 66 | 145 | 624 (71.81%) |
| 22 – 25 | 130 (21.38%) | 64 | 66 | 39 (14.94%) | 11 | 28 | 169 (19.45%) |
| OILY | 529 (87.01%) | 233 | 46 | 110 (42.15%) | 35 | 75 | 639 (73.53%) | 0.000 | 0.1087 | 0.0773– 0.1529 |
| DRY | 79 (12.99%) | 33 | 296 | 151 (57.85%) | 45 | 106 | 230 (26.47%) |
Internal consistency reliability of the multi-item scales was assessed by Cronbach’s coefficient alpha and was found to be 0.794, which can be considered to be adequate for group comparisons. Response to each questions were recorded [Table/Fig-3]. Perception of severity was grouped in mild, moderate and severe according to gender, age and skin type [Table/Fig-4].
Response for each question
| Scale | Not affected | Mildly | Moderately | Very Markedly | |
|---|
| Parameter of life Affected | Score (0) | Score (1) | Score (2) | Score (3) | Mean (n = 608) |
|---|
| Q1 | Self – Consciousness | 32% | 34% | 22% | 12% | 1.137 |
| Q2 | Socialisation | 50% | 25% | 16% | 9% | 0.844 |
| Q3 | Relationship with immediate family | 78% | 11% | 7% | 4% | 0.365 |
| Q4 | Relationship with spouse / partner | 64% | 17% | 13% | 6% | 0.607 |
| Q5 | Relationship with close friends | 67% | 17% | 10% | 6% | 0.541 |
| Q6 | Feeling like an “outcast” | 65% | 20% | 10% | 5% | 0.554 |
| Q7 | Made fun of due to appearance | 68% | 20% | 9% | 4% | 0.479 |
| Q8 | Romantic relationship | 64% | 19% | 9% | 8% | 0.600 |
| Q9 | Rejection by friends | 73% | 15% | 8% | 4% | 0.429 |
| Q10 | Feeling aggressive / frustrated / embarrassed | 40% | 33% | 16% | 10% | 0.959 |
| Q11 | Performance at work / school | 62% | 21% | 11% | 6% | 0.604 |
| Q12 | Finding suitable job | 71% | 13% | 9% | 7% | 0.528 |
| Q13 | Concern of appearance of skin over last month | 27% | 43% | 24% | 6% | 1.099 |
| Q14 | Feeling how bad the acne is | 20% | 58% | 17% | 4% | 1.051 |
| Q15 | Self-perception of severity of acne: | 8 % | 52% | 34% | 6% | 1.156 |
Perception of severity by gender, age and skin type
| Scale | Mild n(%) | Moderate n (%) | Severe n (%) | P-value |
|---|
| Gender | Males | 133 (50.0%) | 102 (38.3%) | 14(5.3%) | 0.1991 |
| Females | 182 (53.2%) | 107(31.3%) | 24(7.0%) |
| Age Group | 14 – 17 | 30 (4.9%) | 26(4.3%) | 4(0.7%) | 0.1991 |
| 18 – 21 | 226 (37.2%) | 131(21.5%) | 19(3.1%) |
| 22 – 25 | 59 (9.7%) | 52(8.6%) | 15(2.5%) |
| Skin Type | DRY | 37 (46.8%) | 28(35.4%) | 4(5.1%) | 0.1991 |
| OILY | 278 (52.6%) | 181(34.2%) | 34(6.4%) |
Among acne sufferers 398 (65.56%) patients were taking some form of treatment while 210 patients (34.43%) were not taking any kind of treatment. Among non-acne participants 54.02% were disturbed by the idea of having acne while 57.09% considered acne is a problem [Table/Fig-5]. Perception score regarding acne in non-acne sufferers is tabulated in [Table/Fig-6]. For Quality of life impairment score [Table/Fig-7], similar response was noted for TAQOL among both the genders.
Non – Acne participants response to questionnaire
| Question | Yes | May Be | No |
|---|
| Qi | Disturbed by the ideaof having acne | 141 (54.02%) | 59 (22.61%) | 61(23.37%) |
| Qii. | Acne is problem | 149 (57.09 %) | 72 (27.59%) | 40 (15.33 %) |
| Qiii. | Obstacle in makingfriends | 55 (20.69%) | 37 (14.18%) | 169 (65.13%) |
Perception score of Acne in Non-acne participant
| Perceiving Acne | Score | Total | Female | Male |
|---|
| | N=261 | N=181 | N = 80 |
|---|
| Acne does not affectour life | -3 | 32.18% | 32.60% | 31.25% |
| 0 | 16.48% | 15.47% | 18.75% |
| Acne can affect our life | 3 | 51.34% | 51.93% | 50.00% |
Quality of life impairment score, TAQOL
Discussion
WHO defines QOL as the individual perception of their position in the context of culture and value systems in which they live and in relation to their goals, expectations, standard and Concerns. Measurement of QOL is done through validated questions [16].
Although acne is sometimes considered to be unimportant in comparison with other medical conditions, the associated morbidity is significant. Acne ruins beauty and in some it scars for life, hence is often considered a cosmetic condition. Acne has a significant impact on the quality of life, wellbeing of sufferer’s in particular adolescent and young adult group. The importance of QOL research in relation to health care evaluation is now well established. It is known fact that Health related Quality of Life (HRQL) is more strongly associated with mental than with physical health status. A general HRQL scales potentially will underestimate physical functional loss in chronically ill people. Disease specific HRQL-questionnaires are more sensitive instruments for specific condition, but outcomes cannot be compared across conditions. This study from India is done on the adolescent and young adult with the age group of 14 – 25. No other similar study has been reported for such large sample size, which looks at the quality of life scale, treatment modalities and perception of acne among non-acne sufferers particularly from our country. Though there is a correlation with severity of quality of life scale, individual perception varies.
Of total 869 participants 69.97% were suffering from acne. Female predominance with 56.25% has been reported in other studies [17,18] too, probably they might be more concern about acne and are aware of the disease. In female patients psychological impact is more than male patients [19,20]. Most common age group affected was 18-21 years in our study with 67.93% from 14 to 25 years of age, which we cannot compare as different study has taken different variables. i.e, a study from India included 18-30year [12]. In this study the self reported acne severity was mild in 52%, moderate in 34% and severe in 6 % as compared to 71.2 % with mild, 28.8% for moderate-severe acne in other study [21]. Self-perceived acne subjective severity rating is reported 12.2% by Do JE et al., [22].
It was observed that there was a large impact on QOL in 68.94% based on the C ADI score. And as per the DLQI score there was a moderate to extremely large impact on the Quality of Life in 75.1% of patients [23].
Studies have found that females have more severe quality of life impairment due to their acne [18]. However, this study showed no significant difference in quality of life issues based on gender as in the mild scale females were more affected with 53.2% than males with 50% while in moderate scale it was vice-versa, 38.3% were males and 31.3% females. In the severity scale of quality of life females were more affected by 7% than males with 5.3% there was no difference between the genders. The 18-21 age group and oily skin type reported higher impairment in severity scale, with 3.1% and 6.4% respectively probably because the population in this groups were higher. Pruthi et al., had studied physical and psychological impact of acne in adult females only in age group 18-25 years [10].
Present study shows 87.01% with acne had oily skin while only 42.15% patients without acne had oily skin higher than reported by Arbuckle et al., [24] where 74% patients with oily skin had mild to moderate acne. Oily skin has both emotional and social impact on patients life. Statistical Correlation of TAQOL, found by Pearson product moment shows P-values below 0.05 was found, indicating statistically significant non-zero correlations at the 95.0% confidence level, Statistical correlation was established between Sex and TQOL (P < 0.417) There was no correlation found between age group and skin type with any of the QOL scores. Of those undergoing treatment of Acne, 65.56% patients were taking treatment compared to 47.9% in one Indian study [12] 82.91% were seeking doctor advice, which is higher than that reported 77% [25]. Significantly higher number, 54.52% were also using Home remedies as it is prevalent in the culture. Over the counter drugs at the pharmacy were obtained by 17.08%. Many were undertaking multiple modalities of remedies. One third of the population i.e. 210(34.43%) with acne in this study was not undergoing treatment, which is a significant number [Table/Fig-8]. Those not undertaking treatment 45.93% didn’t feel the need of undergoing treatment and 15.31% felt they can’t be bothered, which is significantly less than other study [24], this might be as the study group included mostly students pursuing some career, where the priority is usually goal oriented. In 20.57% didn’t know whom to consult, 8.61% found the treatment expensive is also higher than reported by Pawin [25].
Comparative study of acne sufferers not taking treatment
| Taking No Treatment for Acne | N =210 (34.43%) | Pawin et al., [25]N = 489 |
|---|
| No need | 96 (45.93%) | 73 % |
| Cannot be bothered | 33 (15.31%) | 8% |
| Didn’t want to ask parents | 1 (0.47 %) | 7% |
| Fear to consult | 3 (1%) | 4% |
| Too Expensive | 18(8.61%) | 4% |
| Not knowing whom to consult | 43 (20.57 %) | 4% |
Compared to France where adolescent worry even about getting acne, Indians appear to accept acne more readily and its impact on QOL is our populations is of lower magnitude [25]. Another study report, 17.8 % felt that there was no need of treatment [26].
This highlights that the Indian rural population considers dermatological medication costly, not knowing most of the time whom to consult and also less bothered about their look. In majority of Non-acne participants 57.09% considered Acne as a problem which is less than reported 62 %, 54.02% were also disturbed by the idea of having acne, which slightly more than that reported [26]. The difference between the two studies can be due to the cultural and regional difference.
Limitation
The study is a self-administered questionnaire based; hence there is a possibility of individual bias, prejudice to the questions.
Conclusion
Acne has a significant impact on the quality of life and though there is a correlation between various quality of life scale, individual perception varies. Measuring the impact of acne on quality of life allows us to understand the disease from the patient’s point of view. The quality of life scale of acne can vary according to individual perception and differ from population to population, it is an important tool to physicians for better understanding of patients view point and psychological state. Questionnaire evaluation and assessment of quality of life to evaluate the psychological impact cannot replace the proper psychological assessment by a psychologist.