Innominate Artery Aneurysm: Simulating a Thyroid Nodule
K. Felix Jebasingh1, Dukhabandhu Naik2, Anuradha Chandramohan3, Rahul Thampi4, Nihal Thomas5
1 Senior Registrar, Department of Endocrinology, Diabetes & Metabolism, Christian Medical College, Vellore, India.
2 Associate Professor, Department of Endocrinology, Diabetes & Metabolism, Christian Medical College, Vellore, India.
3 Associate Professor, Department of Radiology, Christian Medical College, Vellore, India.
4 Senior Registrar, Department of Endocrinology, Diabetes & Metabolism, Christian Medical College, Vellore, India.
5 Professor, Department of Endocrinology, Diabetes & Metabolism, Christian Medical College, Vellore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nihal Thomas, Professor, Vice Principal (Research), Department of Endocrinology, Diabetes and Metabolism, Christian Medical College Hospital, Vellore-632004, India.
E-mail: nihal_thomas@yahoo.com
Atherosclerosis, Dysphagia, FNAC thyroid, Fusiform dilatation
We report a 69-year-old lady who was referred for the evaluation of a suspected solitary thyroid nodule. The patient noticed a gradually increasing neck swelling of over a year duration along with a history of intermittent dysphagia to solid food without other compressive symptoms. There were no signs and symptoms of hypothyroidism or hyperthyroidism. She had other co-morbidities including Type 2 Diabetes mellitus, Systemic Hypertension and Coronary Artery Disease with no prior history of local trauma. Examination revealed a non-tender soft and non-pulsatile, fluctuant swelling of size 2X 2cm on the right side of the neck just above the sternoclavicular joint [Table/Fig-1]. The swelling moved with deglutition. There was no cervical lymphadenopathy or tracheal deviation. Laboratory investigations revealed a normal Thyroid Stimulating Hormone (TSH) -4.24uIU/ml (Normal-0.8-4.5), Total Thyroxine (T4) of 9.7ug/dl (Normal-4.5-12.5), Free Thyroxine (FT4) – 0.95ng/dl (Normal-0.8-2), with negative anti-thyroid antibodies. The fasting blood glucose was 123mg% (Normal-70-100), Post prandial blood glucose was 185mg% (Normal<140) and Glycated Haemogloin, (HbA1c) of 5.3% (Normal<7%). The lipid profile showed total cholesterol 206 mg% (Normal-<160), LDL–C- 136 mg% (Low Density Lipoproteins) (Normal <100), TG -189 mg% (Trigly cerides) (Normal<150). Ultrasonography of the thyroid did not reveal any thyroid nodule; however the Colour Doppler revealed a focal fusiform dilatation of the right innominate artery measuring 2x2cm in diameter [Table/Fig-2] and no obvious thrombus was detected. Barium swallow showed left ward displacement of the cervical oesophagus [Table/Fig-3] which could be the cause for her dysphagia. Thus, although she was clinically diagnosed to have a thyroid nodule, the Colour Doppler showed a right innominate artery aneurysm. Thus FNAC and thyroid scintigraphy was avoided.
Clinical image of the patient showing nodule in the right side of the neck (shown in arrow)

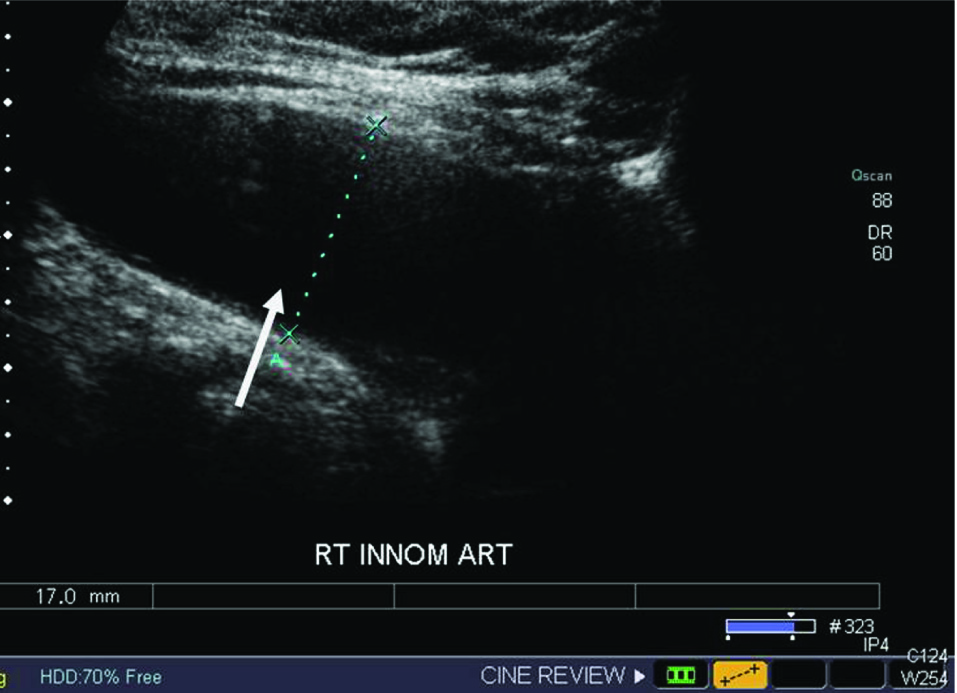
Colour Doppler showed a focal fusiform dilatation of the right innominate artery measuring 2x2 cm in diameter
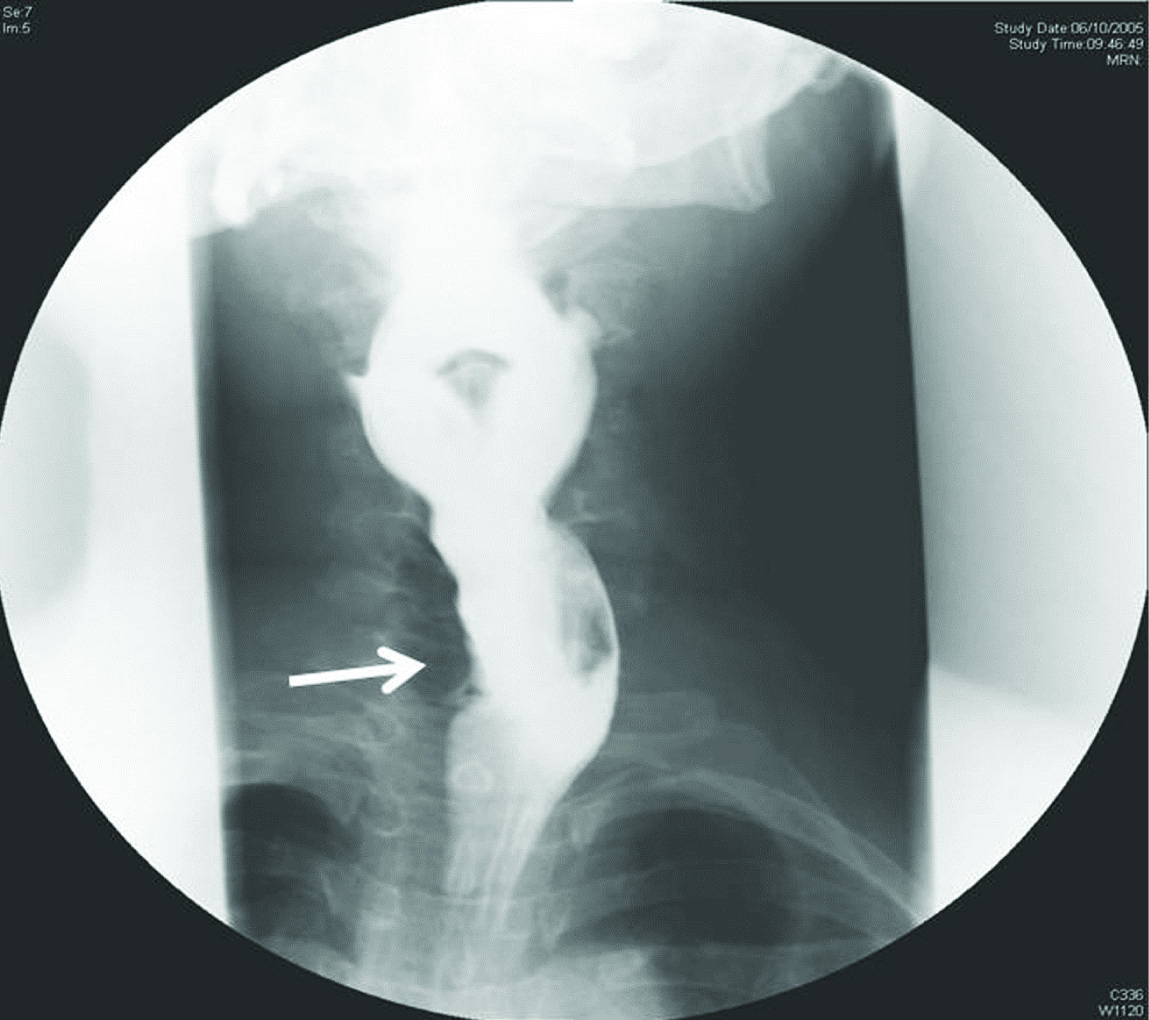
Barium swallow showed left ward displacement of the cervical oesophagus (shown in arrow)
The vascular lesions in front of the neck such as aneurysm or tortuous artery can sometimes resemble a thyroid nodule [1]. The indexed case was of right innominate artery aneurysm, which was initially suspected to be a solitary thyroid nodule. An innominate artery aneurysm is an uncommon entity which occurs exclusively in middle aged women who are at high risk for atherosclerotic disorders [2]. It may be sometimes difficult to appreciate the pulsatility of the aneurysm because of the overlying connective tissues [3]. When ultrasound shows no obvious thyroid nodules, a Colour Doppler study of the neck is helpful in determining the nature of neck swelling as in our patient [4]. Fine needle aspiration in such a circumstance can be catastrophic with potential lethal complications. There is a previous report of a similar case where scintigraphy was done initially that revealed a cold area in the lower lobe. They subsequently performed an ultrasound that led to the diagnosis and stressed the importance of Colour Doppler Sonography as a compliment to nuclear medicine procedures in that scenario [1,5]. The patients’ clinical picture is suggestive of atherosclerotic disease, which probably played a causal role in the development of aneurysmal disease. The other causes of innominate artery aneurysm are trauma, infection, connective tissue disease, Kawasaki’s disease, and Takayasu’s arteritis [6], Small size innominate artery aneurysm is usually asymptomatic, present either as an incidentally detected neck mass or as a superior mediastinal mass on chest x-ray [7]. Patients with innominate artery aneurysm may presents with symptoms like hoarseness of voice or dysphagia due to compression of localized structures and neurological symptoms due to thrombo-embolism [8]. Ultrasound with Doppler is diagnostic, when lesions are located in the neck region. However, CT scan is indicated in case of mediastinal lesion. Asymptomatic innominate artery aneurysms are usually managed conservatively. Surgery is indicated if the size of aneurysm is more than 3 cm in transverse diameter or in the presence of thrombus or if complicated by thrombo-embolism [9]. In our case surgery was not offered as there was no definite indication. She is currently under regular follow-up without any worsening of symptoms.
Conclusion
This case highlights that a high index of suspicion is required to identify a vascular cause for neck swelling when they present with symptoms suggestive of thyroid nodule. Vascular cause should be especially thought off in patients with risk factors for atherosclerotic disease.
[1]. Brander A, Viikinkoski P, Voutilainen L, Kivisaari L, Clinical versus ultrasound examination of the thyroid gland in common clinical practiceJ Clin Ultrasound 1992 20(1):37-42. [Google Scholar]
[2]. Brewster DC, Moncure AC, Darling RC, Ambrosino JJ, Abbott WM, Innominate artery lesions: problems encountered and lessons learnedJ Vasc Surg 1985 2(1):99-112. [Google Scholar]
[3]. Kelly R, Hayward C, Avolio A, O’Rourke M, Noninvasive determination of age-related changes in the human arterial pulseCirculation 1989 80(6):1652-59. [Google Scholar]
[4]. Lacout A, Marcy PY, Thariat J, RE: Role of duplex doppler us for thyroid nodules: looking for the “sword” signKorean J Radiol 2011 12(3):400-01. [Google Scholar]
[5]. Bowles T, Hyams G, Postel AH, Tortuous Common carotid artery simulating a thyroid adenomaJAMA 1963 186:513-14. [Google Scholar]
[6]. Bower TC, Pairolero PC, Hallett JW, Toomey BJ, Gloviczki P, Cherry KJ, Brachiocephalic aneurysm: the case for early recognition and repairAnn Vasc Surg 1991 5(2):125-32. [Google Scholar]
[7]. Schumacher PD, Wright CB, Management of arteriosclerotic aneurysm of the innominate arterySurgery 1979 85(5):489-95. [Google Scholar]
[8]. Cherry K, Treatment of extracranial, carotid, innominate, subclavian and axillary aneurysmsIn Mastery of vascular and endovascular surgery: An illustrated review. Edited by Zelenock GB, Huber TS, Messina LM, Lumsden B, Moneta GL 2006 Philadelphia, PaLippincott, Williams & Wilkins:79-84. [Google Scholar]
[9]. Kieffer E, Chiche L, Koskas F, Bahnini A, Aneurysms of the innominate artery: surgical treatment of 27 patientsJ Vasc Surg 2001 34(2):222-28. [Google Scholar]