Management of Osteoarthritis Knee by Graduated Open Wedge High Tibial Osteotomy in 40-60 Years Age Group Using Limb Reconstruction System: A Clinical Study
Rajesh Kapila1, Pawan Kumar Sharma2, Ankush Chugh3, Randhir Singh4
1 Associate Professor, Department of Orthopaedics, Government Medical College and Hospital, Amritsar, Punjab, India.
2 Resident, Department of Orthopaedics, Government Medical College and Hospital, Amritsar, Punjab, India.
3 Junior Resident, Department of Orthopaedics, Government Medical College and Hospital, Amritsar, Punjab, India.
4 Professor, Department of Orthopaedics, Government Medical College and Hospital, Amritsar, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajesh Kapila, Address: 2-B, Circular Road, Amritsar, Punjab- 143001, India.
E-mail: kapila.rajesh@yahoo.com
Background
With i ncrease in elderly population, osteoarthritis has become major concern nowadays. Knee joint is most commonly affected joint. A number of methods have been developed in the last few years which help in treating the osteoarthritis knee, which includes non pharmacological, pharmacological and surgical methods. Among the most promising techniques with renewed interest for osteoarthritis knee with deformity is the use of high tibial osteotomy. Uni-compartmental osteoarthritis knee with deformity especially in relatively younger age group (less than 60 years) constitutes the main indication.
Aim
The aim of present study was to evaluate management of osteoarthritis knee by graduated open wedge high tibial osteotomy in 40-60 years age group using limb reconstruction system.
Materials and Methods
Medial Opening Wedge High Tibial Osteotomy leaving the lateral cortex intact which acts as a hinge, was done in 30 patients and stabilized by Limb Reconstruction System. Distraction was started at 7th day at the rate of 1 mm/day and continued till proper alignment was achieved.
Results
Medial Opening Wedge High Tibial Osteotomy stabilized by unilateral external fixator is a good method for unicompartmental osteoarthritis knee with deformity as it gives precise control over final limb alignment and its ability to perform a residual correction. Deformity correction can be quantified at the time of correction as it is not acute correction. Gradual deformity correction can be done over time by distraction histogenesis with the help of unilateral external fixator. It is also a good method in young patients requiring large correction.
Conclusion
Medial Opening Wedge High Tibial Osteotomy is having many benefits over closed wedge osteotomy and stabilization by unilateral external fixator also has its added benefits. It is less invasive, no internal hardware present and safer in terms of neurovascular complications.
Distraction histogenesis, High tibial osteotomy, Limb reconstruction system, Unicompartmental
Introduction
With the increase in life expectancy due to improved health care system the incidence of human degenerative joint disorder is on the rise. Knee is the most commonly affected joint. Osteoarthritis (OA), the most common joint disease, is age related, affecting more than 80% of people over the age of 55. Osteoarthritis pathogenesis involves an imbalance between normal cartilage degradative and repair mechanisms, which results in net loss of cartilage, hypertrophy of bone, and generation of osseous outgrowths called osteophytes. The heterogeneity of OA arises from the many factors that can contribute to cartilage damage [1].
Patients typically report pain that is increased with activity and relieved by rest, though rest pain occurs in advanced disease. Morning stiffness, when present, rarely lasts more than 30 minutes. Symptom severity ranges from asymptomatic disease diagnosed radiographically to significant pain with functional limitation. Physical examination findings of the affected joints include tenderness on palpation, crepitus (palpable friction) with movement, bony enlargement, abnormal alignment, decreased range of motion and sometimes joint effusion. Diagnosis can be made with reasonable certainty based on history and clinical examination. X-rays may confirm the diagnosis. The characteristic radiographic features of OA are osteophytes, asymmetric joint space narrowing, subchondral bone sclerosis and subchondral cysts [1].
Management of osteoarthritis of knee may be non-surgical and surgical. Non-surgical management may be-
Non Pharmacological such as weight reduction, change in lifestyle, heat and cold therapy, moderate exercise along with use of braces and orthosis which make the patient comfortable [2,3].
Pharmacological methods such as: NSAIDs especially Acetaminophen provides substantial relief of pain with much less toxicity [2,4], Viscosupplements such as Glucosamine and Chondroitin [2,3,5,6], Diacerein and lately collagen peptides and Rose hip may be somewhat useful by variable mechanisms of action [7]. Of late quite a bit of interest has been generated by the use of Rotational Field Quantum Magnetic Resonance (RFQMR) as a non surgical method of ostoeathritis management.
Surgical management: Among the various surgical options joint replacement is quite popular as it gives long lasting pain relief besides good function. However, due to increase in life expectancy, reoperation may be required as no joint can last lifelong. Secondly in young high demand patients some activity restrictions may be required after arthroplasty. So herein lies the importance of High Tibial Osteotomy (HTO) which provides a well aligned, pain free and excellent functional knee for a pretty long time which may either delay a replacement for many years or may eliminate its need.
Materials and Methods
The study was conducted in Orthopedics Department of a Tertiary care centre on patients admitted here for treatment of uni-compartmental osteoarthritis knee. Thirty patients of osteoarthritis knee were selected for this study in the age group of 40 years and above. The informed consent of each patient was taken on the prescribed proforma. This study was undertaken after due approval by the Ethics Committee.
The indications for proximal tibial osteotomy are: (1) pain and disability resulting from osteoarthritis that significantly interfere with high-demand employment or recreation; and (2) weight-bearing radiographs showing degenerative arthritis that is confined to one compartment with a corresponding varus or valgus deformity. The patient must be able to use crutches or a walker and have sufficient muscle strength and motivation to carry out a rehabilitation program [8].
Contraindications to a proximal tibial osteotomy are: (1) narrowing of lateral compartment cartilage space; (2) lateral tibial subluxation of more than 1 cm; (3) medial compartment tibial bone loss of more than 2 or 3 mm; (4) flexion contracture of more than 15 degrees; (5) knee flexion of less than 90 degrees; (6) more than 20 degrees of correction needed; (7) inflammatory arthritis; and (8) significant peripheral vascular disease [8].
Patients X-rays were taken to know the grade of osteoarthritis knee according to Kellgren-Lawrence Grading System for OA [Table/Fig-1] [9]. The extent of deformity was determined from weight bearing full limb roentgenograms and recorded as the mechanical axis deviation. A straight line was drawn between centre of head of femur to centre of dome of talus before operation, and after the correction of deformity [Table/Fig-2]. Postoperatively mechanical axis should pass from the Fujisawa point with the limb in 5-7 degree valgus [10]. Uniplanar external fixator (Limb reconstruction system by Pitkar) was used for deformity correction in this study.

Scannogram of the patient showing Mechanical Axis of the limb

In surgical procedure two pins were passed proximal to the osteotomy site and two distal to the osteotomy site which was distal to tibial tuberosity. The first pin in the proximal part was passed as posterior as possible. This place was determined by passing a wire and cannulated bit was passed over it. The second pin was passed in anterior part keeping maximum distance between two pins. Similarly two pins were passed distal to the osteotomy site with a distance of 3 to 4 cm between the pins. Through a small incision bone was exposed subperiosteally and an oblique osteotomy was done towards the proximal tibiofibular joint leaving the lateral cortex intact. The hinge was provided with this lateral cortex [Table/Fig-3]. Two clamps were fixed to the pins and these were mounted over a rail. Compression distraction unit (CD unit) was mounted over the two clamps and distraction was done to check the opening of the osteotomy [Table/Fig-4]. After closing the osteotomy, wound was stitched. Distraction was started at 7th day at the rate of 1 mm/day and continued till proper alignment was achieved. Average duration of distraction was 22 days. Regular follow up was carried till a solid union was achieved. Patients were advised weight bearing as early as possible depending upon the patient’s comfort. Radiological evidence of bony union was seen at 12 weeks in most of the patients [Table/Fig-5]. Fixator was removed after confirming the union.
Intraoperative osteotomy site
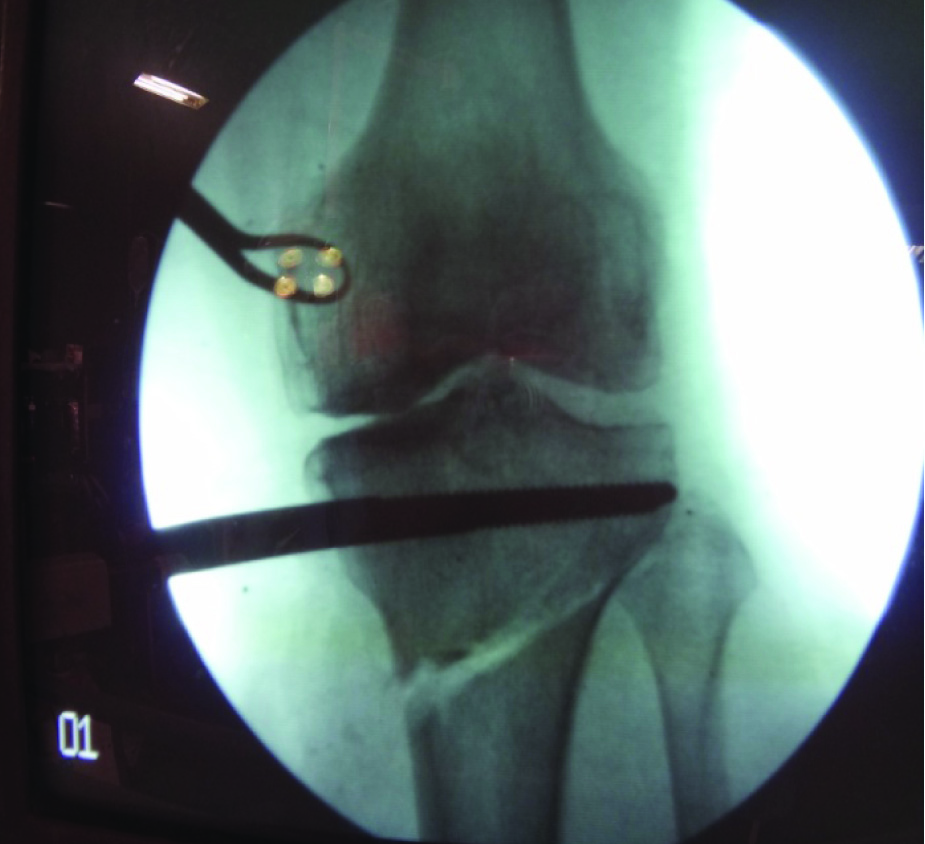
Clinical picture of LRS application

At 12 weeks follow up showing Radiological Union

Observations and Results
In this study, 30 osteoarthritic knees were treated. In this series none of the knees had undergone another surgical procedure except osteotomy. All the patients received a fair trial of conservative treatment including rest, anti-inflammatory analgesics, quadriceps exercises, hot fomentation, wax bath and walking aids. It was only in those patients in whom such a trial provided minimal or no relief and the patients had disabling pain with radiographic evidence of unicompartmental osteoarthritis knee, that HTO was performed to improve the symptomatology by mechanical as well as biological reasons. Mean age in our study was 49.2 years ranging from 41-60 years. Females were predominant sex (76.6%). Obesity (BMI more than 30) was the main risk factor in 18 cases (60%) and the average duration of symptoms were 3-5 years.
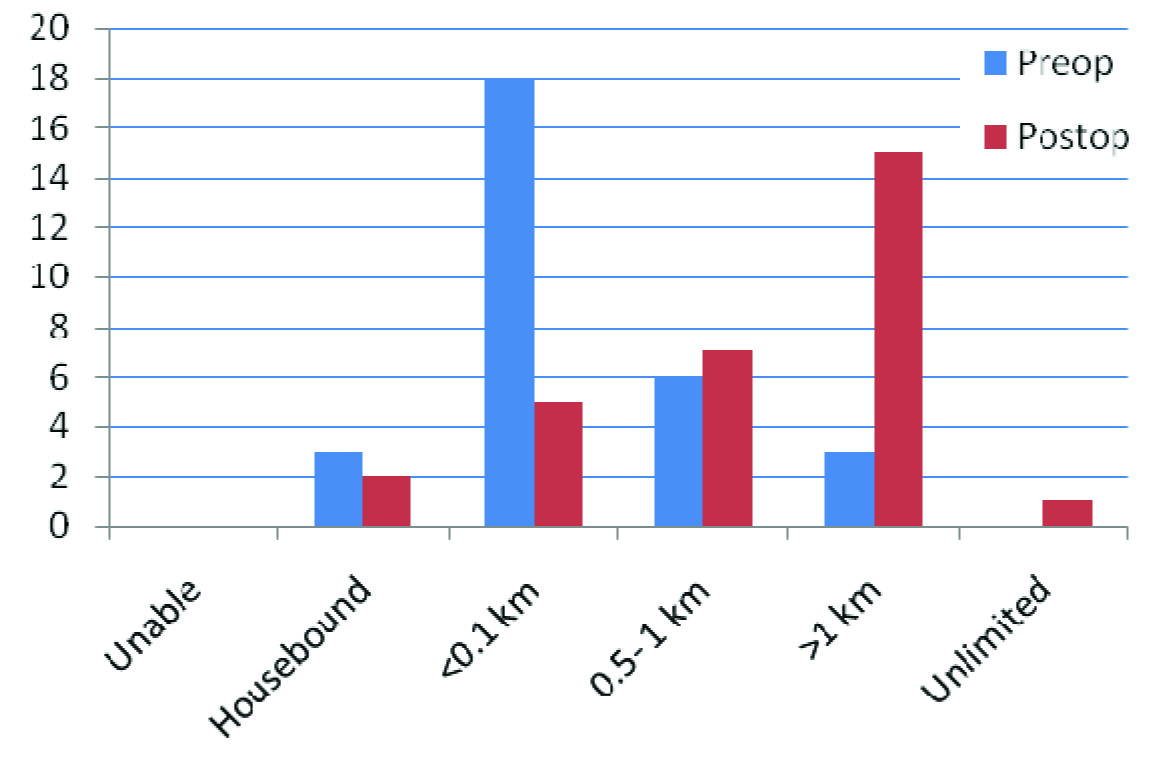
From the [Table/Fig-6] it was quite clear that the various pre operative parameters showed a marked improvement postoperatively. Pain which was the main criteria for surgery showed a significant improvement. Preoperative walking distance also showed marked improvement [Table/Fig-7].
Observations of the study
| Parameter | Preoperative (Average) | Postoperative (average) |
|---|
| Preoperative deformity | 8-10 degree Varus (0%) | 5-7 degree Valgus (60%) |
| Preoperative pain (VAS) | Moderate to severe (100%) | None to mild on strenuous activity (70%) |
| Range of motion | Greater than 125 degree | No significant difference |
| Walking distance | 100 Meters or less (60%) | More than 1 Kilometer (50%) |
| Thrust | 100% | 30% |
| Radiological union | – | 12 weeks (70%) |
| Clinical Knee Score | Less than 60 (100%) | 70-100 (80%) |
Pre and postoperative walking distance
There was not much significant change in the range of motion postoperatively with only 4 patients showing some decrease (loss of 15-20 degree). Thrust which indicates ligamentous laxity was present in 100% of patients preoperatively showed marked improvement with 70% showing no thrust postoperatively. Radiological union was seen by 12 weeks in majority of cases. Clinical knee score which was poor in all 100% of the cases improved markedly postoperatively with 80% patients having good to excellent score [Table/Fig-8,9].
Showing excellent end result

Showing postoperative deformity correction

Discussion
The present study was conducted on 30 cases of OA Knee with the main aim to assess the efficacy of HTO in improving the knee function. Medial opening wedge osteotomy stabilized by Limb Reconstruction system (LRS) was the technique used and a follow up of 24 weeks was done.
HTO may be closed wedge or open wedge. It may be done proximal or distal to the tibial tubercle and may be stabilized by internal or external fixation [11–14]. The first HTO was done by Jackson which was distal to the tibial tubercle while Coventry did his HTO proximal to the tibial tubercle which had the advantage of high union rates due to quality of bone proximal to tibial tubercle [15,16]. Goran Bauer et al., described a lateral closing wedge osteotomy which had disadvantages of requiring extensive soft tissue dissection on lateral aspect, more chances of neurological involvement, requires disruption of superior tibiofibular joint with partial excision of fibular head [17].
Open wedge osteotomy can be done either as an acute correction using some internal hardware or it can be done in a graduated manner using distraction histogenesis principle. Opening wedge haemicallotasis described by Turi et al., using an external fixator to distract the osteotomy site gradually [18]. This technique has got various advantages such as being minimally invasive, no need of fibular osteotomy, minimal risk of nerve damage and subtle corrections by continuous opening of osteotomy. In addition the stability of Medial collateral ligament is also improved.
The mean age at the time of osteotomy was 49.2 years which is comparable to a study by Robinson PM et al., [11]. Females were the predominant sex as seen in a study by Nakamura et al., [19]. Obesity was the major risk factor in OA and strong association has been well established [20–22].
Preop varus deformity was 8-10 degrees (50%). Our aim was to achieve postop mechanical axis of 6-8 degree valgus with Fujisawa point as reference. We could achieve 5-7 degree valgus in 60% of the cases. Pain was the main criteria for performing this procedure and 100% of patients had moderate to severe pain preoperatively. However postoperative pain relief was pretty good with 70% patients having none or mild pain that too on strenuous exercise. This is in accordance with a study by Insall et al., where 75% patients had partial to complete relief of pain [23].
In this study, majority of the patients maintained or rather improved their preoperative range of motion. Only 4 patients had some decrease in range of motion postoperative (15-20degree). Similar results have been described by Insall et al., [23]. So it is imperative to start knee mobilization as soon as possible.
In our study, walking distance was also a major determinant in the final outcome and there was a dramatic increase in walking distance (more than 1 Km in 40%). In this study, majority of patients had radiological union at a mean of 12 weeks (10-16) after surgery. This observation coincides pretty well with study of Nakamura et al., [19]. In this study, thrust, defined as sideways movement of the knee in the coronal plane thus indicating ligamentous laxity was present in all cases preoperative. After correction 70% showed no instability which is in accordance with Insall et al., [23].
The overall outcome with this procedure was quite encouraging. With pain relief, range of motion and walking distance as the major determining factors, the overall clinical knee score was excellent to good in 80% of cases.
Conclusion
From the above study, it is quite clear that Open wedge Osteotomy using Limb Reconstruction System is an effective method of managing OA knee especially in younger patients with Unicompartmental Knee involvement. It is minimally invasive, requires no fibular osteotomy, minimal chances of nerve injury, easy to perform and no internal hardware used requiring subsequent removal. Besides correction is graduated and not one time as is seen with use of fixed angle plates where we may get under/over correction. We strongly recommend this procedure in relatively younger patients as it may delay the need of joint replacement and in some cases it may actually avoid it.
[1]. Ashman RF, Ferguson PJ, IJdo JW, Lawry GV II, Rheumatic Diseases: Diagnosis and Management; Weinstein, Stuart L; Buckwalter, Joseph A; Turek’s Orthopaedics: Principles and Their Application 2005 6th EditionLippincott Williams & Wilkins:154-55. [Google Scholar]
[2]. Keene JS, Dyreby JR, High tibial osteotomy in the treatment of osteoarthritis of the knee. The role of preoperative arthroscopyAm J Bone Joint Surg 1983 65:36-42. [Google Scholar]
[3]. Maquet P, Advancement of the tibial tuberosityClin Orthop Relat Res 1976 115:225 [Google Scholar]
[4]. Jackson JP, Waugh W, Tibial osteotomy for osteoarthritis of the kneeJ Bone Jt Surg Br 1961 43-B:746-51. [Google Scholar]
[5]. Maquet P, Simonet J, Demarchin P, Biomacanique du gensouet gonarthrose. In Symposium, les Gonarthrosesd’origine StatiqtneRev Chir Orthop 1967 53:111-38. [Google Scholar]
[6]. Markolf KL, Bargar WL, Shoemaker SC, Amstutz HC, The role of joint load in knee stabilityJ Bone Joint Surg 1981 63(4):570-85. [Google Scholar]
[7]. Meding JB, Keating EM, Ritter MA, Faris PM, Total knee arthroplasty after high tibial osteotomy. A comparison study in patients who had bilateral total knee replacementJ Bone Joint Surg Am 2000 82(9):1252-59. [Google Scholar]
[8]. Andrew H, Crenshaw Jr, Soft tissue procedures and corrective osteotomies about the knee: S Terry Canale, James H Beaty; Campbell’s Operative Orthopaedics 2013 Volume 112th editionPhiladelphiaMosby Elsevier:471 [Google Scholar]
[9]. Kellgren JH, Lawrence JS, Radiological assessment of osteoarthrosisAnnals of the Rheumatic diseases 1957 16:494-501. [Google Scholar]
[10]. Fujisawa Y, Masuhara K, Shiomio S, The effect of high tibial osteotomy on osteoarthritis of knee. An arthroscopic study of 54 knee jointsOrthop Clin North Am 1979 10:585-608. [Google Scholar]
[11]. Robinson PM, Papanna MC, Somanchi VB, Khan SA, High tibial osteotomy in medial compartment osteoarthritis and varus deformity using the Taylor spatial frame: early resultsStrategies Trauma Limb Reconstr 2011 6(3):137-45. [Google Scholar]
[12]. Koschino T, Morii T, Wada J, High Tibial osteotomy with fixation by a blade plate for medial compartment osteoarthritisof the kneeAm Orthop Clinic North 1989 20:227-43. [Google Scholar]
[13]. Catagni MA, Guerreschi F, Ahmad TS, Cattaneo R, Treatment of genu varum in medial compartment osteoarthritis of knee using the ilizarov methodOrthop Clinic North Am 1994 25:509-14. [Google Scholar]
[14]. Hoell S, Suttmoeller J, Stoll V, The high tibial osteotomy, open versus closed wedge: a comparison of methods in 108 patientsArch Orthop Trauma Surg 2005 125:638-43. [Google Scholar]
[15]. Jackson JP, Osteotomy for osteoarthritis of the kneeJ Bone Jt Surg Br 1958 40:826 [Google Scholar]
[16]. Coventry MB, Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary reportJ Bone Jt Surg Am 1965 47:984-90. [Google Scholar]
[17]. Bauer GC, Insall J, Koshino T, Tibial osteotomy in gonarthrosis (osteo-arthritis of the knee)J Bone Jt Surg Am 1969 51:1545-63. [Google Scholar]
[18]. Turi G, Cassini M, Tomasi PS, Armotti P, Lavini F, Directional osteotomy of the knee using haemicallotasisChir Organi Mov 1987 72(3):205-09. [Google Scholar]
[19]. Nakamura E, Mizuta H, Takagi SK, Sakamato K, Open wedge osteotomy of the proximal tibia with haemicallotasisJ Bone Joint Surg Br 2001 83(8):1111-15. [Google Scholar]
[20]. Coggon D, Reading I, Croft P, Mclaren M, Barrett D, Cooper C, Knee Osteoarthritis and obesityInt J Obes Rel Met Dis 2001 25(5):622-27. [Google Scholar]
[21]. Felson D, Zhang Y, Anthony J, Naimark A, Anderson J, Weight loss reduces the risk for symptomatic knee osteoarthritis in women: the Framingham studyAnn Intern Med 1992 116(7):535-39. [Google Scholar]
[22]. Felson D, Anderson J, Naimark A, Walker AM, Meenan RF, Obesity and knee osteoarthritis: the Framingham studyAnn Intern Med 1988 109(1):18-24. [Google Scholar]
[23]. Insall JN, Shoji H, Mayer V, High tibial osteotomy. A Five Year evaluationJ Bone Joint Surg 1974 56:1397-405. [Google Scholar]