Delay in diagnosis is a collective term for patient delay and health system delay. The patient delay refers to the time interval between onset of disease till patients approach the formal health facilities [2,8–12]. Health system delay is the time for complete diagnosis of the disease after patient approaches for formal health care provider [2,8,9,12].
The prompt identification of cases depends on patients recognizing TB symptoms and seeking appropriate health care as well as the capacity of the health care system to diagnose the disease. Delays in diagnosis and treatment of TB have important implications towards the individual and community [12]. At individual level, patients experiencing long delays in initiation of treatment may have an increased risk of developing severe disease and death [8,12,13].
Therefore, understanding the magnitude of the delay can prove to be fruitful for the management of TB and taking an appropriate action for its control in future. The objectives of the study was to investigate all types of delay in diagnosis of a new pulmonary tuberculosis patient in the central development region of Nepal.
Materials and Methods
Ethical consideration: The present study was approved by office of the Khon Kaen University ethics committee in human research (Reference No. HE 582071) and institutional review committee, Kathmandu University School of Medical Sciences, Dhulikhel, Nepal (Protocol approved number 08/15). In addition, the informed consent was taken from each of the respondents to protect their autonomy.
Study design
A cross-sectional study was conducted by administering structured questionnaire interview amongst the new smear positive pulmonary tuberculosis cases in the center development region of Nepal. The study was conducted between January-May 2015. The study required two additional interviewers apart from the researcher to collect the data. The interviewers were the paramedics (Health Assistants) who had basic training on medicine and surgery for three years after finishing ten years of schooling. They received a formal training before the start of the survey. We randomly selected at least one district from each geographical region, totally 5 districts were drawn out of the 19 districts from the study region followed by listing the treatment centers in the selected districts. Finally, we selected and interviewed a total of 374 respondents by applying systematic random sampling at each treatment center of the selected districts. New smear positive pulmonary tuberculosis cases above 15 years of age were included in this study. Smear negative, relapse, retreatment, return after defaulter, and the patient those who had history of prior TB were excluded.
The sample size was calculated by using the formula required for determination of sample size for estimating single proportion [14]. By taking a previous study done on delay in diagnosis and treatment in Uganda [6], which showed 58% proportion of patient delay of more than one month, 95% confidence interval and a margin error of 5%, the sample size for this study was calculated to be 373.84 and our sample size was fixed to be 374. The structured questionnaire was translated to the Nepali language and assessed. The questionnaire included various questions relating to socio-demographics, major symptoms of PTB, duration of first symptom presented the date of first health care visit for diagnosis, the basic knowledge on tuberculosis, attitude and stigmatization. Patient’s treatment cards, TB registration books and laboratory register were cross checked to assure the quality of data. The questionnaire was tested by 5 experts for content validity. The attitude and stigmatization parts had high reliability of eight and seven questions respectively. In addition, the questionnaire was pretested before presenting to the study population to make it more clear and valid.
Statistical Analysis
Based on the previous studies, we took ≥30 days for patients, ≥7 days for health system and ≥ 28 days for total delay as cut off points to dichotomize the sample for identifying the unacceptable delays in diagnosis of TB [6,9]. The categorical data were reported as number and percentage mean, standard deviation, median and range (minimum-maximum) described for the continuous variable. Proportion and their 95% CI had been reported. Responses to questions that assessed TB knowledge, attitude and stigma related to TB were analysed by calculating their percentile score and finally, the responses were categorized into yes/no, good/bad and presence/absence. STATA (Version 13, Stata Corporation, College Station TX) was used for data analysis.
Results
A total of 374 new smear positive pulmonary TB patients were randomly enrolled from 5 districts representing at least one from each 3 ecological region of Central Development Region (CDR), Nepal. The median patient, health system and total delay were 32 (IQR 11-70), 3 (IQR 0-7) and 39.5 (IQR 17-84) days respectively [Table/Fig-1].
Characteristics of delay in diagnosis
| Characteristics | Number of days | Delay (%) | 95% CI |
|---|
| Patient delay | 199 | 53.21 | 48.12-58.29 |
| Mean(SD) | 78.64 (233.94) | | |
| Median (IQR) | 32 (11-70) | | |
| Health system delay | 100 | 26.74 | 22.23-31.24 |
| Mean(SD) | 14.13 (44.32) | | |
| Median (IQR) | 3 (0-7) | | |
| Total delay | 235 | 62.83 | 57.91-67.75 |
| Mean(SD) | 92.77 (240.17) | | |
| Median (IQR) | 39.5 (17-84) | | |
The following [Table/Fig-2] described that the proportion of males slightly exceeds the females with a ratio of 1.7:1. The mean age of the patients were 39.68±18.6 SD years with a median age of 35.03 years, minimum 15.07 and maximum of 100.56 years. The highest proportion of the respondents (39.84%) was in their reproductive age (15-29 years). Nearly two third (66.58%) of the respondents were from the urban areas of Nepal, whereas the rest 33.42% were residing in the rural areas. Majority (59.36%) of respondents were non-smokers while 40.64% were current smokers or had just quit. Among smokers, 75.66% smoke ≥5 cigarettes per day.
Characteristics of study population
| Characteristics | Number (%) |
|---|
| Gender |
| Male | 234 (62.57) |
| Female | 140 (37.43) |
| Age (years) |
| 15–29 | 149 (39.84) |
| 30–44 | 85 (22.73) |
| ≥ 45 | 140 (37.43) |
| Mean (SD) | 39.68 (18.6) |
| Median (Min: Max) | 35.03 (15.07: 100.56) |
| Residence |
| Urban | 249 (66.58) |
| Rural | 125 (33.42) |
| Income (per month in NRs) |
| < 5000 | 35 (11.08) |
| 5000-7500 | 24 (7.59) |
| ≥ 7500 | 257 (81.33) |
| Mean (SD) | 27087.91 (46731.45) |
| Median (Min: Max) | 17000 (1000: 380000) |
| Smoking |
| Never | 222 (59.36) |
| Currently /used to smoke but stop currently | 152 (40.64) |
| Number of cigarettes in a day |
| < 5 | 37 (24.34) |
| ≥ 5 | 115 (75.66) |
| Basic knowledge on TB |
| No | 278 (74.33) |
| Yes | 96 (25.67) |
| Attitude |
| Bad | 223 (59.63) |
| Good | 151 (40.37) |
| Stigma |
| Absent | 195 (52.14) |
| Present | 179 (47.86) |
| Distance to reach the TB center |
| < 5 KM | 291 (78.44) |
| ≥ 5 KM | 80 (21.56) |
| Mean (SD) | 4.25 (11.82) |
| Median (Min: Max) | 2 (1:200) |
| Means of transport |
| Traveling | 167 (44.65) |
| Walking | 207 (55.35) |
| Centre of first contact |
| Traditional healer/ self-treated | 18 (4.81) |
| Private practitioners | 159 (42.51) |
| Government health facilities | 197 (52.67) |
Most of the respondents (78.44%) answered that the TB services were available in <5km of distance from their homes and more than half (55.35%) of them had to walk to reach DOTS center. However, government health facilities were considered by 52.67% of the participants to seek their first advice, private practitioners/pharmacists/vendors by 42.51% and 4.81% of them visited traditional healer. Majority of the participants (55.88%) were examined by medical officer, but fewer than half were diagnosed on the basis of sputum examinations (43.05%) and paramedics and chest specialist treated the rest.
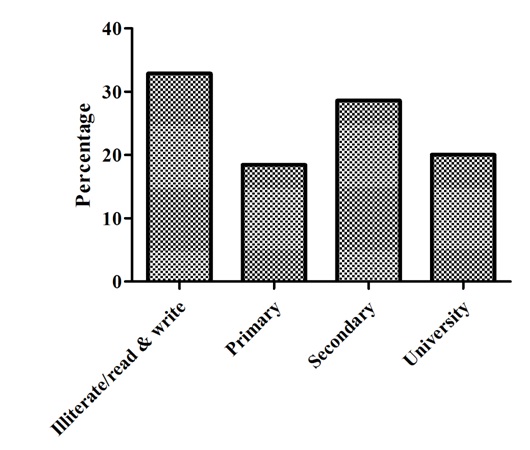
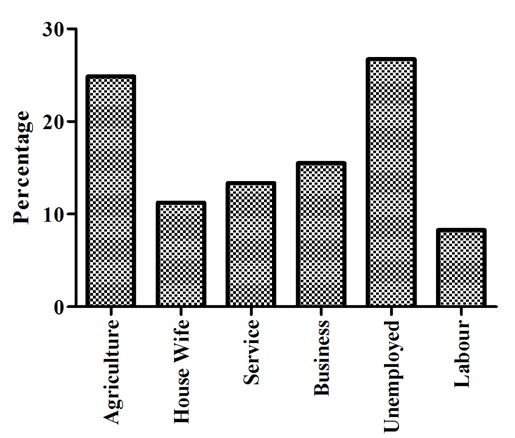
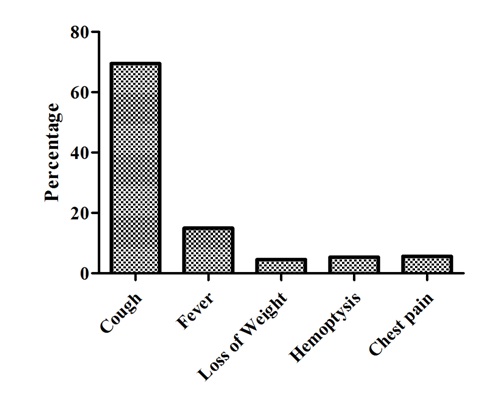
In addition, the marital status of the majority of the respondents was married followed by single and widowed [Table/Fig-3]. The highest proportion of the respondents (32.89%) never attended formal education, 18.45% finished primary school, 28.61% completed secondary school, and remaining 20.05% attended higher than the college level [Table/Fig-4]. Nearly one fourth of the tuberculosis patients (24.87%) were farmers and 26.74% were jobless [Table/Fig-5]. Cough was the most frequently reported symptom (69.52%) followed by fever (14.97) and 4.55% weight loss [Table/Fig-6].
Marital status of the respondents

Educational attainment of the respondents
Occupational status of the patients
First symptom present before diagnosis of TB
Prevalence of delays
The prevalence of patient delay was 53.21% (95% CI: 48.12-58.29) [Table/Fig-1]. The given [Table/Fig-7] illustrated that there was high prevalence of patient delay observed among those who lived in rural areas (65.6%, 95% CI: 57.16-74.04). The patients who were unable to achieve the primary education have 62.60 % (95% CI: 53.93-71.27) of patient delay. The farmers seemed to have more prevalence of 65.59% (95% CI: 55.75-75.43) patient delay in comparison with other occupations.
Prevalence of patient delay (PD) and health system delay by different independent variables and their 95% CI
| Patient delay | Health system delay |
|---|
| Characteristics | n | (%) | 95%CI | n | (%) | 95%CI |
|---|
| Gender |
| Male | 126 | 53.85 | 47.41-60.28 | 61 | 26.07 | 20.40-31.73 |
| Female | 73 | 52.14 | 43.76-60.52 | 39 | 27.85 | 20.34-35.38 |
| Age (years) |
| 15–29 | 76 | 51.01 | 42.89-59.13 | 50 | 33.56 | 25.89-41.22 |
| 30–44 | 44 | 51.76 | 40.92-62.61 | 21 | 24.71 | 15.35-34.06 |
| ≥ 45 | 79 | 56.43 | 48.11-64.74 | 29 | 20.71 | 13.92-27.51 |
| Residence |
| Urban | 117 | 46.99 | 41.59-53.23 | 72 | 28.92 | 23.24-34.59 |
| Rural | 82 | 65.6 | 57.16-74.04 | 28 | 22.4 | 14.99-29.81 |
| Education |
| Illiterate/read & write | 77 | 62.60 | 53.93-71.27 | 27 | 21.95 | 14.53-29.37 |
| Primary | 40 | 57.97 | 46.03-69.92 | 13 | 18.84 | 09.38-28.30 |
| Secondary | 45 | 42.06 | 32.56-51.56 | 35 | 32.71 | 23.68-41.74 |
| University | 37 | 49.33 | 37.75-60.91 | 25 | 33.33 | 22.41-44.25 |
| Occupation |
| Agriculture | 61 | 65.59 | 55.75-75.43 | 17 | 18.28 | 10.28-26.28 |
| Housewife | 20 | 47.62 | 31.87-63.37 | 07 | 16.67 | 04.91-28.42 |
| Service | 22 | 44.00 | 29.75-58.25 | 10 | 20.00 | 08.51-31.48 |
| Business | 28 | 48.28 | 35.02-61.53 | 17 | 29.31 | 17.24-41.38 |
| Unemployed | 52 | 52.00 | 42.04-61.96 | 45 | 45.00 | 35.08-54.92 |
| Labour | 16 | 51.61 | 32.98-70.25 | 04 | 12.90 | 0.04-25.40 |
| Income (per month in NRs)(n=316) |
| < 5000 | 24 | 68.57 | 52.39-84.75 | 7 | 20.0 | 06.06-33.94 |
| 5000-7500 | 14 | 58.33 | 37.07-79.59 | 05 | 20.83 | 03.32-38.35 |
| ≥ 7500 | 130 | 50.58 | 44.43-56.74 | 70 | 27.24 | 21.76-32.72 |
| Smoking |
| Never | 111 | 50.0 | 43.37-56.63 | 62 | 27.92 | 21.98-33.88 |
| Currently /used to smoke but stop currently | 88 | 57.89 | 49.96-65.83 | 38 | 25.0 | 18.04-31.96 |
| Number of cigarettes in a day (n=152) |
| < 5 | 26 | 70.27 | 54.82-85.72 | 8 | 21.62 | 07.71-35.54 |
| ≥ 5 | 62 | 53.91 | 44.66-63.16 | 30 | 26.09 | 17.94-34.23 |
| Symptoms present before diagnosis |
| Cough | 135 | 51.92 | 45.81-58.04 | 72 | 27.69 | 22.22-33.17 |
| Fever | 32 | 57.14 | 43.77-70.52 | 12 | 21.43 | 10.34-32.52 |
| Loss of weight | 09 | 52.94 | 26.49-79.39 | 5 | 29.41 | 05.26-53.56 |
| Haemoptysis | 10 | 50.00 | 25.99-74.01 | 4 | 20.00 | 0.08-39.21 |
| Chest pain | 13 | 61.90 | 39.25-84.56 | 7 | 33.33 | 11.35-55.21 |
| Basic knowledge on TB |
| No | 148 | 53.24 | 47.34-59.14 | 64 | 23.02 | 18.04-28.00 |
| Yes | 51 | 53.13 | 42.96-63.29 | 36 | 37.50 | 27.64-47.36 |
| Attitude |
| Bad | 114 | 51.12 | 44.51-57.73 | 63 | 28.25 | 22.29-34.21 |
| Good | 85 | 56.29 | 48.29-64.29 | 37 | 24.50 | 17.56-31.44 |
| Stigma |
| Absent | 98 | 50.26 | 43.18-57.34 | 55 | 28.21 | 21.83-34.58 |
| Present | 101 | 56.42 | 49.09-63.76 | 45 | 25.14 | 18.72-31.56 |
| Distance to reach the TB center (n=371) |
| < 5 KM | 141 | 48.45 | 42.68-54.23 | 80 | 27.49 | 22.33-32.65 |
| ≥ 5 KM | 57 | 71.25 | 61.11-81.39 | 20 | 25.00 | 15.30-34.69 |
| Means of transport |
| Traveling | 105 | 62.87 | 55.47-70.28 | 44 | 26.35 | 19.59-33.09 |
| Walking | 94 | 45.41 | 38.57-52.25 | 56 | 27.05 | 20.95-33.16 |
| Centre of first contact |
| Traditional healer/ self-treated | 13 | 72.22 | 49.30-95.14 | 9 | 50.00 | 24.41-75.59 |
| Private practitioners | 79 | 49.69 | 41.83-57.54 | 38 | 23.90 | 17.19-30.60 |
| Government health facilities | 107 | 54.31 | 47.29-61.33 | 53 | 26.90 | 20.66-33.15 |
| Categories of HCP for TB diagnosis |
| Paramedics | 35 | 40.23 | 29.72-50.74 | 24 | 27.59 | 18.01-37.17 |
| Medical officer | 112 | 53.59 | 46.77-60.40 | 55 | 26.32 | 20.29-32.34 |
| Specialist | 52 | 66.67 | 55.97-77.36 | 21 | 26.92 | 16.86-36.99 |
| Method of TB diagnosis |
| Sputum examination | 80 | 49.69 | 41.88-57.49 | 48 | 29.81 | 22.67-36.96 |
| X-ray | 55 | 52.38 | 42.67-62.09 | 29 | 27.62 | 18.92-36.31 |
| Advanced technique | 64 | 59.26 | 49.84-68.68 | 23 | 21.29 | 13.45-29.14 |
In addition, 70.27% (95% CI: 54.82-85.72) of the patient delay has been observed among the respondents, who smoked < 5 cigarettes per day. The patients, who lived more than 5 km far from the DOTS centers had the high prevalence of patient delay (71.25%, 95% CI: 61.11-81.39). Furthermore, the respondents, who used any mode of transportations and seek care from chest specialist have observed to be increasing the prevalence of patient delay with 62.87% (95% CI: 55.47-70.28) and 66.67% (95% CI: 55.97-77.36) respectively.
However, the patient who had completed their secondary education were found to have less patient delay (42.06%, 95% CI: 32.56-51.56) in comparison with those who were illiterate. Similarly, those who have an access of DOTS center within walking distance were observed to have less prevalence of patient delay (45.41%, 95% CI: 38.57-52.25).
This study revealed that the proportion of health system delay was 26.74% (95% CI: 22.23-31.24) [Table/Fig-1]. The increased prevalence was observed among the patient who were unemployed (45.0%, 95% CI: 35.08-54.92) and those who don’t have basic knowledge on tuberculosis (37.50%, 95% CI: 27.64-47.36). However, farmers (18.28%, 95% CI: 10.28-26.28) and labour workers (12.90%, 95% CI: 0.04-25.40) had less prevalence of health system delay [Table/Fig-7].
Discussion
The study aimed to understand the major delays in diagnosis of tuberculosis in central development region of Nepal. This study was conducted in 5 districts of that region and it highlights the unacceptable delay from onset of cough to inition TB diagnosis. We found that the median patient’s delay is 32 (IQR 11-70) days. The findings are similar with the several other studies that were conducted in Angola [15], Malaysia [16], and Uganda [6] showing median patient’s delay of 3-4 weeks. On the other hand, previous study conducted in Nepal [9] found 50 days for median patient delay. This might be because the study was conducted six years ago in 2009 and it was conducted in only one district of far western development region of Nepal. The changes in trend signify that the knowledge and socio-economic status of the people has been improved simultaneously with increasing literacy rate as well as expansion of DOTS facilities within these years. However, the studies revealed that the patient delay in low and middle income countries varies from 4.9 days in Gambia to 162 days in Tanzania [2,15].
The median health system delay was very short, i.e. only 3 (IQR 0-7) days, suggesting that referrals and diagnosis were swift whenever a person with TB interacted with the health system. Our result is correlated as found in other studies [8,15,17]. However, some other studies in Malawi [12] and Mozambique [13] revealed 59 (IQR 26-108) days and 150 (IQR 91-240) days as health system delays respectively. Even though the length of median health system delayed is shorter in this study, the magnitude of unacceptable (≥ 7 days) health system delay was 26.74%. Our result is quite near to the study conducted in Croatia which had 30% of health system delay [7]. Because of the inappropriate management of the DOTS facilities, studies have shown that the health system delay varies from 47.8% in Malawi [12] to 88% in the study conducted in Uganda [6].
In this study, gender wise the proportion of males exceeded the females with the ratio of 1.7:1. This is quite similar with the national (2.2:1) and regional figures of the gender wise distribution of TB [3,4]. Similar higher prevalence of TB in males has been reported in other studies as well [6,18]. The higher risk of TB in males may be due to higher exposure of risk factors to males. The distribution of population by age also showed that the majority was in the reproductive age group (15-29 years) [15]. More than 60% of them were between age group of 15-44. The mean age of the study population was 39.68 years, which is also similar with the trend in general in developing countries like Ethiopia and Uganda [6,19]. According to the South Asian regional report, all new cases detected in the region in 2012 were among the young adults, particularly in the reproductive age group [3].
As per this study, two third of the respondents were married. Nepal demographic health survey, 2014 revealed that the 76% women and 64% male were currently married [20]. One third of the respondents participated in this study were form the rural areas of Nepal as the central development region has more urban area than that of other region i.e. 36% [20]. Therefore, the prevalence of patient delay was high among them and those who were illiterate. In addition, the proportion of patient delay was more likely to increase among farmers. This clearly indicates very poor socio economic condition among the study population. It is evident that tuberculosis is most common in low socio-economic class, immigrants, homeless and refugees [21].
Furthermore, the distance of the DOTS center of 5 km from where they lived is contributing in an unacceptable patient delay. Even though, the DOTS centers are continuously expanding since 2005, it has not reached proximately to the TB patient in significant manner with assured quality. Study of the Ibadan, Nigeria, shows that the far distance of health services had 22.2% chances of prolonging delay [10,22]. Moreover, the means of transportation was also equally responsible for the rising patient delay. This might be due to the less availability of transportation services in mountain and hilly region and the travel cost is significantly higher. However, those patients who had completed their secondary education and got the facilities of DOTS center in the walking distance were found to have less proportion of patient delay.
On other hand, the prevalence of health system delay significantly raised among those who were unemployed and having poor knowledge on TB. This is again recommended that the socio-economic status of the country needs to be improved. The awareness on TB will reduce the burden in significant manner. However, surprisingly the proportion of health system delay was seen low among the farmers (18.28%, 95% CI: 10.28-26.28). This might be due to the improving the economy of farmer in terai region. Therefore, this study indicate that the proportion of delay in diagnosis of TB varies according to the regions more in mountain, followed by hilly and less in terai region.
Limitation
As, the information of the study depended on self-reports based on recall history and individual variations in perception of disease. The study, however, planned to include only the cases which had been recently diagnosed to minimize the recall bias. To overcome such limitations, questionnaire was pre-tested to make sure that all questions were understandable. In addition to that, the interviewer recruited for the study received training before the start of the study. The technical and field trainings were given as per requirement of the study to the recruited interviewer. However, this study only described the prevalence of delays, so we can generalised it to the population to make them aware on the prevalence of major delays and take appropriate action to reduce such delays.
Conclusion
This study revealed a long patient delay among the patient with pulmonary TB. Though the health system delay was short, it shows that Nepal still has a significant problem of TB diagnosis and treatment. Most of the Patient delay was caused due to the inaccessible health facilities, poor knowledge on TB. Identifying major delays and developing evidence-based approaches to address those delays will help in advancing tuberculosis prevention and management in low-income settings like Nepal. This will also be the key to success for reducing TB burden. Further study should be conducted to see the relation between longer pre-treatment delays and its effect on treatment outcome on the already studied patients. The magnitude of individuals having suspected symptoms of TB but did not seek treatment should be explored to better understand the impact of diagnostic delay in the case finding activity in the region.