Poisoning is an important health care problem in developing countries, resulting in hospitalization, utilization of health care resources and high mortality. According to the World Health Organization (WHO), 0.3 million people die due to various poisoning agents annually [1]. Each year, 500,000 suicidal deaths are reported to occur in rural Asia, of which 200,000 are due to organophosphates (OP) poisoning alone [2]. Acute pesticide poisoning with agents like aluminium phosphide (ALP) and organophosphate poisonings (OPP) is very common in North India as majority of people are farmers [3]. Early diagnosis, treatment and prevention are the only measure through which this problem can be solved.
Thus, the purpose of this study was to study the demographic and clinical profile of patients presenting with acute poisoning to the Intensive care unit (ICU) and to identify the factors at admission that may predict their mortality.
Materials and Methods
This was a retrospective study of all patients admitted to ICU with acute consumption of poison over a period of two years (September 1, 2010 to August 31, 2012). All ICU admissions from acute poisonings were identified from the ICU registry and the files of these patients were extracted from the hospital medical records. The following data was collected and documented in a prestructured performa: demographic details, date and time of admission and consumption of poison, Acute Physiology And Chronic Health Evaluation (APACHE II) and Sequential Organ Function Assessment (SOFA) and Glasgow coma score (GCS) at admission, type (suicidal or accidental), route and the chemical compound used for poisoning. Biochemical parameters of these patients were also noted including, arterial blood chemistry, electrolytes and serum bilirubin. The need for any intervention such as mechanical ventilation, renal replacement therapy or requirement of vasoactive agents, outcome parameters like duration of mechanical ventilation and ICU stay was documented. We also documented outcome parameters like duration of mechanical ventilation and ICU stay. All patients were studied till death or discharge from the ICU.
Statistical Analysis
Descriptive statistics are presented as percentages; mean ± SD. Chi square test was performed to test the significant categorical variables. Linear discriminant analysis was performed to test the significance of continuous variables with respect to the variable outcome. All statistical analysis was performed using SPSS, version 21.0, Armonk, NY: IBM corp, p<0.05 was considered statistically significant.
Results
During the study period, 67 patients were admitted to ICU with acute poisoning. The majority of patients were males (n=46, 69%), with a median age of 29 (range 15-76) years. Most patients had consumed the poison with a suicidal intent (94%). The oral route (95.5%) was the most common one employed.
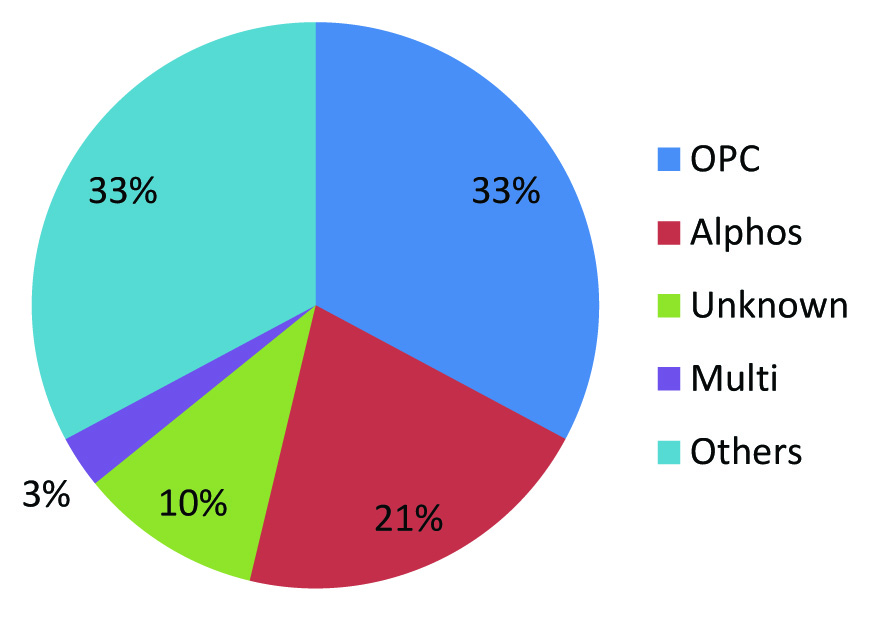
Organophosphorus compounds were the most common poison (22 patients, 32.8%) consumed, followed by aluminium phosphide (14 patients, 20.9%). In 10.4% of cases, the agent of poisoning was unknown [Table/Fig-1]. The mean delay between consumption of poison and presentation to the hospital was 4.075 ± 3.850 hours. The mean APACHE II and SOFA scores at admission to the ICU were 8.73 ± 5.2 and 3.94 ± 3.33, respectively. The mean Glasgow coma score at admission was 11.10± 4.63.
Agents of poisoning
OPC, Organophosphorus compounds; Alphos, Aluminum Phosphide; Others, drugs like benzodiazepines, calcium channel blockers
Laboratory investigations at admission revealed a mean serum sodium level of 141 ± 7.13meq/L, mean serum potassium level of 3.95 ± 0.57meq/L, Mean serum chloride level of 104.6 ± SD 6.00meq/L and a mean serum bilirubin level of 0.75 ± SD 0.64mg% [Table/Fig-2].
| Variables | Mean±SD | Range | p-value |
|---|
| APACHE II | 8.73 ± 5.27 | 0-19 | <0.001 |
| SOFA | 3.94 ± 3.33 | 0-12 | 0.006 |
| Delay (hours) | 4.07 ± 3.85 | 1-15 | .254 |
| GCS | 11.10 ± 4.63 | 3-15 | .917 |
| pH | 7.30 ± 0.13 | 6.75-7.58 | .099 |
| HCO3 | 18.58 ± 5.30 | 7.3-28.7 | .108 |
| Na | 141.84 ± 7.13 | 122-170 | .099 |
| K | 3.95 ± 0.57 | 2.1-5.7 | .504 |
| Cl | 104.64 ± 6.00 | 88-122 | 0.018 |
| Bili | 0.75 ± .64 | .02-4.70 | .930 |
*SD – Standard Deviation
APACHE – Acute physiology and chronic health evaluation score SOFA – Sequential Organ Function Assessment
GCS – Glasgow coma scale
HCO3 – Bicarbonate Na - Sodium
K – Potassium Cl – Chlorine Bili – Bilirubin
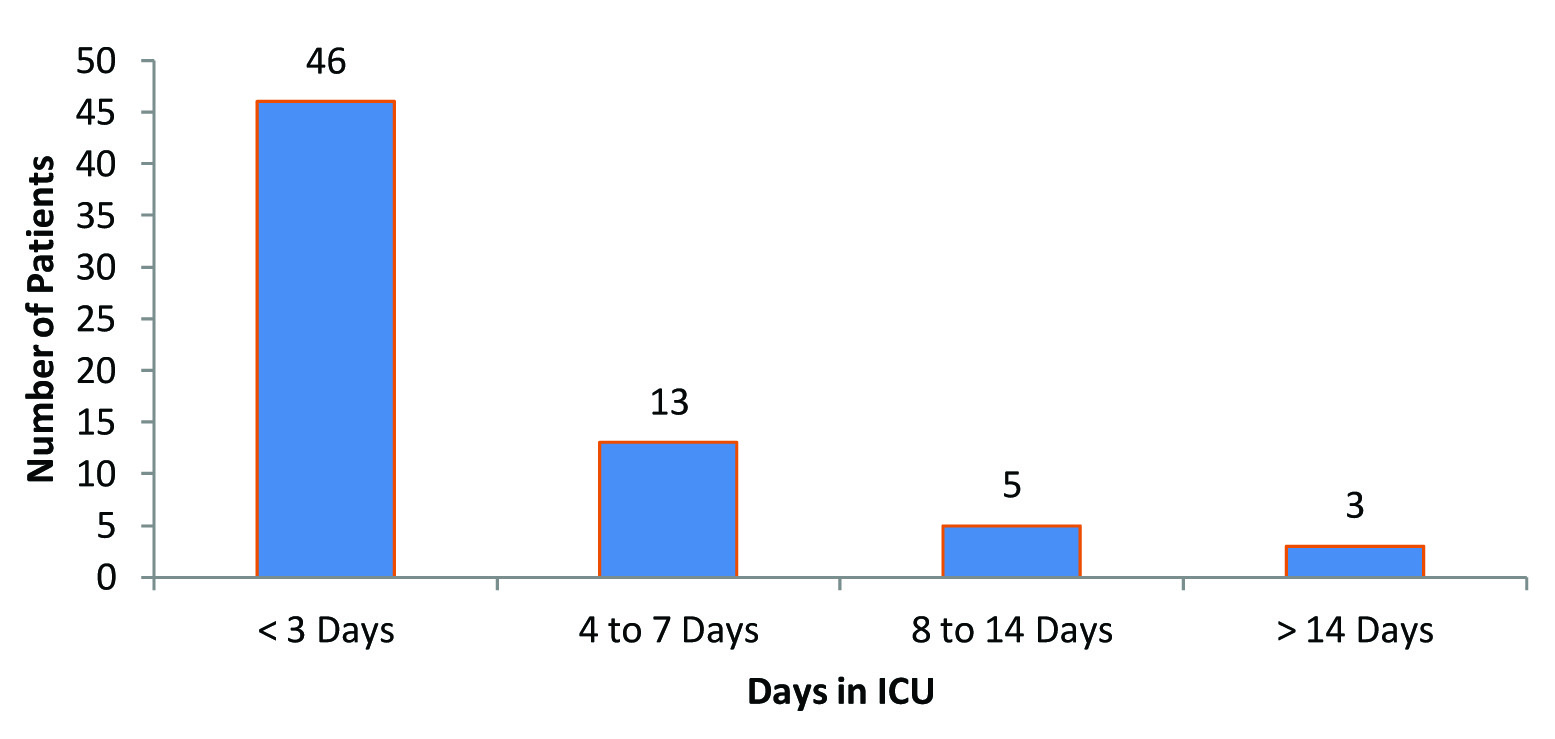
Out of 67 patients studied, 43 had required mechanical ventilation for an average of 3.81 days. More than 70% (48 patients) had three or more organ system involvement at admission to the ICU, while 30% (20 patients) had significant hypotension requiring the use of vasoactive drugs like noradrenaline, dopamine and adrenaline infusions. Only two patients had acute kidney injury severe enough to need haemodialysis. The mean duration of mechanical ventilation was 3.81± SD 4.36 days and the mean ICU stay was 3.9 ± 0.544 days [Table/Fig-3]. The overall ICU mortality from acute poisonings was 18% (12 patients). On univariate analysis, the factors which were found to correlate with mortality were the need for mechanical ventilation and vasoactive support (p=0.012 and p= 0.0001, respectively). Both, the APACHE II and the SOFA scores were found to reliably predict mortality in our patients. (p =0.0001 and p=0.006, respectively) [Table/Fig-4].
Duration of total ICU days
Factors evaluated for prediction of mortality in patients with acute poisoning (Univariate Analysis)
| Variables | Survivors(n = 51)Mean±SD | Non-Survivors(n = 12)Mean±SD | p-value |
|---|
| Age | 32 ± 13 | 33 ± 16 | .773 |
| APACHE II | 7.59 ± 4.89 | 14 ± 2.86 | <0.001 |
| SOFA | 3.31 ± 3.06 | 6.67 ± 2.64 | 0.006 |
| Delay (hours) | 4.02 ± 3.65 | 5.17 ± 4.95 | .721 |
| GCS | 11.24 ± 4.46 | 10.75 ± 5.41 | .904 |
| pH | 7.32 ±0 .11 | 7.29 ± 0.13 | .244 |
| pH<7.2 | 1.82 ± 0.39 | 1.67 ± 0.49 | .231 |
| HCO3 | 19.33 ± 4.63 | 15.88 ± 6.58 | .064 |
| Na | 141 ± 5.64 | 145 ± 11.49 | .177 |
| K | 3.91 ± 0.5 | 4.13 ± 0.88 | .426 |
| Cl | 103.84 ± 4.79 | 108.92 ± 9.27 | .013 |
| Bili | .76 ± 0.69 | .68 ± 0.37 | 1.00 |
| Days Intubated | 4.57 ± 5.03 | 2.50 ± 2.47 | 0.001 |
| Total ICU Days | 4.45 ± 4.88 | 2 ± 2 | .015 |
On subgroup analysis of the patients who had consumed organophosphorus compounds (22 patients), more patients were found to have required mechanical ventilation than the overall average (17 patients, and 77%), however, mortality rates remained approximately the same (18.2%). We found that high APACHE II and SOFA scores (p=0.024 and p=0.003 respectively) as well as the need for vasoactive drugs (p=0.001) at admission to the ICU correlated positively with deaths from organophosphorus poisoning.
Among the patients who had ingested Aluminium Phosphide (14 patients), the mean APACHE II and SOFA scores at admission were 10.6 ± SD 6.5 and 4.6 ± SD 4.0 respectively. These patients had much higher average mortality rates (35%) and the factors which were significantly associated with mortality were, a higher APACHE II score (p=0.051), lower GCS (≤ 12) (p<0.001), acidotic pH (p<0.001), need for mechanical ventilation (p=0.005) and the need for vasoactive agents (p=0.04).
Discussion
In a developing country like India poisoning is a major health problem, though the type of poison and the associated morbidity and mortality varies from one place to another [4,5]. Suicidal poisoning with house-hold agents (OPs, carbamates, pyrethrinoids, etc.) is the most common modality of poisoning in India [6]. Thus a detailed knowledge about the nature, clinical profile and severity of presentation from acute poisoning is not only important for early diagnosis and prompt treatment but is also essential for triaging patients appropriately and developing predictive scores to reliably prognosticate outcomes.
Typically males are more vulnerable to deaths from poisonings than females, with several studies reporting twice as many deaths in them [7]. This trend is reflective of the greater stress and strain, occupational hazards and the better accessibility of poisons to them [8].
The majority of our patients belonged to the age group of 20-40 years, the most active and yet the most vulnerable to stressors like examination failure, unemployment, marital problems etc [9,10].
As reported by many national and international studies on acute poisoning, we also found that most acute poisonings were suicidal [11] and commonly employed the oral route [12].
One of the major causes of death in rural and agricultural areas across the world is acute pesticide poisoning [3,13] with developing countries reporting high fatality rates from poisoning following pesticide consumption. The most commonly employed pesticides in India are organophosphorus compounds and aluminium phosphide compounds [14–16]. Our study also revealed the same findings. Other studies from urban subpopulations in India report aluminium phosphide to be the commonest poison consumed followed by organophosphorus compounds [13,17–19]. The rampant use of pesticides in our country, the ease of their availability, their low cost are probably some of the reasons why these are commonly employed for self- poisoning [17,20–23].
Following poisoning, patients may report after a significant delay to an appropriate health care facility. The speed with which a patient receives clinical attention, the efficacy of treatment provided and the degree to which the toxicity is understood are all contributory to the clinical outcomes of patients. Ramesha et al., reported that time was a significant factor in determining mortality and patients who had presented within 2 hours of poisoning had the least mortality [24]. Our patients presented after a mean delay of approximately four hours, which may account for the high mortality rates seen.
In developed countries mortality rate from poisoning is 1-2% [25], but in developing countries where critical care resources are limited and time delays are significant, mortality rates are quite high. In India, the reported mortality due to poisoning varies between 15-30% [26,27]. In our study a total of 12 patients died in the two year period and mortality rate was 18%. Prajapati, Unikrishnan, Boukatta et al., and Cengiz et al., documented mortality rates from acute poisonings as 18.6%, 15.7%, 10.9% and 5.8% respectively [5,25,28,29].
Among our patients the factors which contributed to mortality were, a high APACHE II and SOFA score, need for mechanical ventilation and vasoactive support. Some studies reported APACHE II as better than SAPS score in the prediction of mortality and morbidity associated with poisoning [30] while others [31] have found that the SOFA score was more useful and simpler to use than the APACHE II and SAPS II scores.
Organophosphate pesticides are responsible for a vast majority of deaths in most series of poisoning episodes especially from rural parts of the developing world, with reported mortality in hospital based surveys as high as 46%. In our study, the mortality of patients who consumed organophosphorus compounds was 18.2% and this was similar to the rates reported by Ali et al., [32].
We found that severity of illness scores like the APACHE II [33] and SOFA scores were significantly useful in predicting increased mortality and the need for vasoactive drugs at admission to the ICU was predictive of poor outcomes. In a retrospective cohort study of 76 consecutive cases presenting with acute organophosphorus poisoning, serum acetylcholinesterase levels of less than 1000 the time elapsed after ingestion to presentation of greater than two hours, and SpO2 (at room air) at presentation lesser than 85%, were found to predict need for mechanical ventilation. In the same study, a low level of consciousness (GCS ≤ 12) was predictive of the need for ventilation and a prolonged hospital stay [34]. Davies et al., reported that the Glasgow coma scale and the International Program on Chemical Safety Poison Severity Score (IPCS PSS) were similarly effective in predicting outcomes from OP poisonings [35]. A prospective descriptive survey to assess the utility of severity scales in 71 patients with organophosphate (OP) and carbamate poisoning over a one year period concluded that significant correlation (p < 0.05) between poisoning severity score and GCS and APACHE II and predicted mortality rate were observed with the poisoning severity score predicting mortality significantly (p < 0.001) [36].
Aluminium phosphide, a highly toxic compound used mainly for storage of wheat in granaries, is increasingly being used as a modality of poisoning, particularly in north-western parts of India. The toxicity of this compound stems from the release of phosphine gas after contact with water in the stomach. The gas is cytotoxic and mediates free radical mediated injury. The mortality rates from this compound are much higher, varying from 40 to 80% [37]. In the present study, we found that ingestion of aluminium phosphide resulted in a mortaliy of 35% and the factors which were associated with mortality were, low GCS (score ≤ 12, acidotic pH (pH ≤ 7.2), need for mechanical ventilation and the need for vasoactive agents. High APACHE II scores reliably predicted mortality in these patients. Several other studies have also found that early evidence of organ dysfunction; low APACHE II score, acidosis, and need for vasoactive drugs for haemodynamic instability have all been associated with poor prognosis [38]. Another retrospective study on aluminium phosphide poisoning done by Boukatta documented that the factors implicated in causing deaths were, delay in the initiation of treatment, presence of potassium disorders, and need for mechanical ventilation, vasoactive drugs and shock [39,40].
Thus, our study highlights the typical patterns of acute poisoning among patients presenting to a tertiary level hospital. Data such as this will help in enhancing the knowledge on profile of poisoning and aid in formulating more effective preventive and management strategies. In addition, the study of the factors affecting mortality as revealed in our study can be a useful tool in the ICU and emergency department to prognosticate outcomes in such patients. There were however two major limitations in our study. Firstly, the inherent limitations of an observational retrospective study and secondly, as ours was a tertiary care centre, most patients had been referred to us from other smaller centers. Thus, the patients who presented to our hospital were probably the ones who could not be managed at the primary care level and therefore, were sicker. Hence our data may not be truly reflective of the patterns of poisoning at the community level.
Conclusion
The present data gives additional insight to the epidemiology of acute poisoning in our country and reflects the need for stringent rules regarding the availability and sale of these substances. Early psychiatric consultation will minimize the risk of next attempt of self harm in suicidal cases. Effective clinical management of poisoning can minimize the mortality.
*SD – Standard Deviation
APACHE – Acute physiology and chronic health evaluation score SOFA – Sequential Organ Function Assessment
GCS – Glasgow coma scale
HCO3 – Bicarbonate Na - Sodium
K – Potassium Cl – Chlorine Bili – Bilirubin