Renal Myxoma- A Rare Variety of Benign Genitourinary Tumour
Kamlesh S. Suthar1, Aruna V. Vanikar2, Rashmi D. Patel3, Kamal V. Kanodia4
1 Assistant Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences (IKDRC-ITS), Ahmedabad, India.
2 Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences (IKDRC-ITS), Ahmedabad, India.
3 Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences (IKDRC-ITS), Ahmedabad, India.
4 Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences (IKDRC-ITS), Ahmedabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kamlesh S. Suthar, Assistant Professor, Department of Pathology, Laboratory Medicine, Transfusion Services and Immunohematology, G.R. Doshi and K.M. Mehta Institute of Kidney Diseases and Research Centre and Dr. H.L. Trivedi Institute of Transplantation Sciences (IKDRC-ITS), Ahmedabad- 380016, Gujarat, India. E-mail : drksuthar@gmail.com
Renal myxomas are rare neoplasms and very few cases have been reported in literature. Here we report a renal myxoma in a 48-year-old lady with hypothyroidism who presented with abdominal pain. She was found to have a mass lesion of 67 x 61 x 74 mm with exophytic component in the right kidney on ultrasonography and computed tomography. Right radical nephrectomy was performed due to suspicion of malignancy. Grossly the resected kidney showed a gelatinous, semi-translucent mass involving the mid and lower poles. Microscopy revealed marked hypocellular appearance of loose myxoid tissue with foamy histiocytes. Tumour cells were reactive for vimentin. At eight months of follow-up, patient is doing well.
Benign neoplasm, Kidney, Myxoid tissue
Case Report
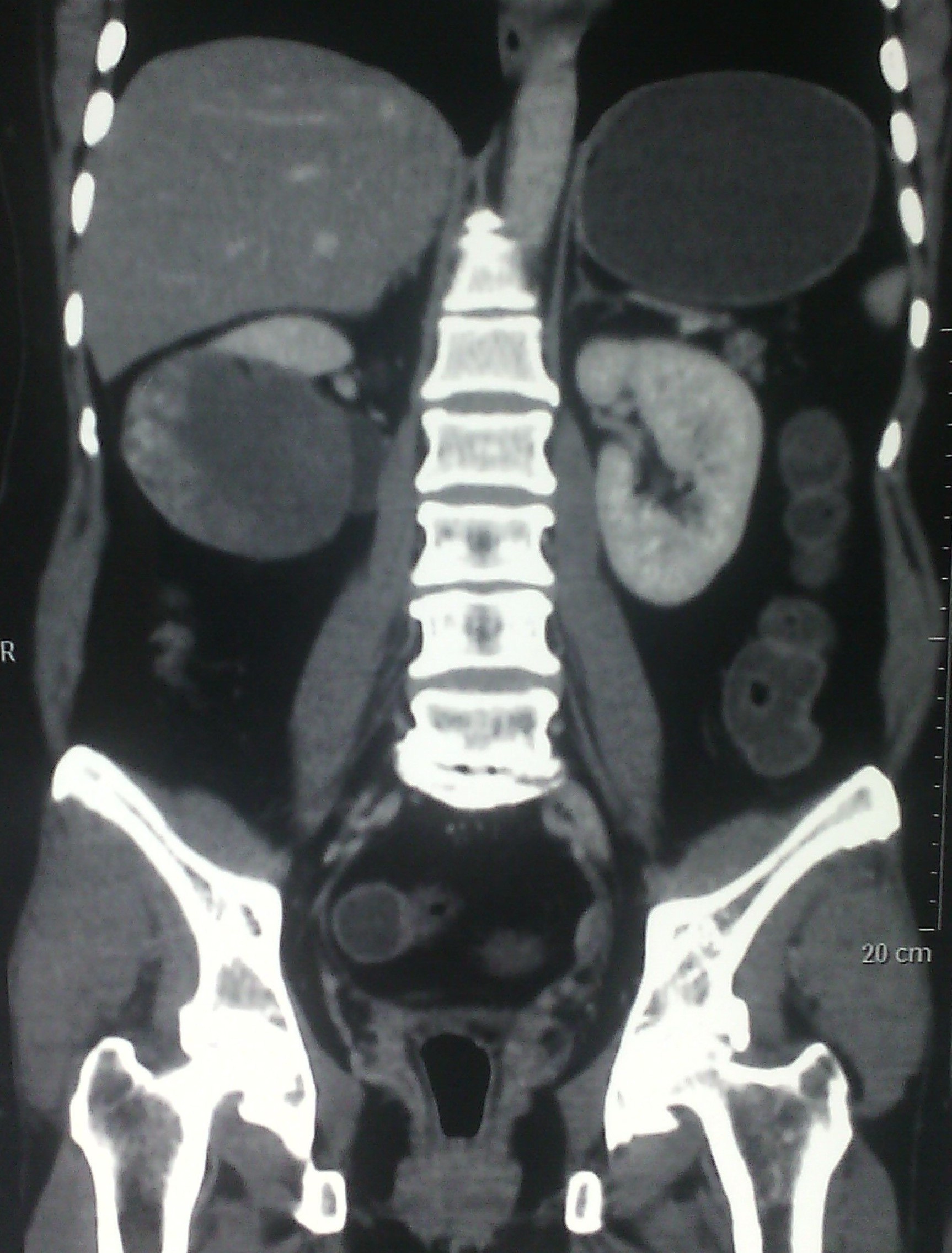
A 48-year-old female presented with right side dull-aching abdominal pain of 15 days duration. She had undergone hemithyroidectomy 7 years back for colloidal goiter and was on supplement thyroid hormone. No other significant past, present or family history was noted. Her general and systemic examination was unremarkable. Haematological and biochemical investigations were within normal limits. Ultrasonography (USG) showed an ill-defined hypoechoic mass in right kidney (RK). Computed Tomography (CT) was suggestive of hypo-dense well-defined mass involving mid and lower pole of RK, measuring 67 x 61 x 74 mm in size, with exophytic component [Table/Fig-1]. She was subjected to right radical nephrectomy and specimen was received for histopathological examination.
CT showing hypo-dense well defined mass involving mid and lower pole of kidney
Grossly RK weighed 600 grams and measured 13 x 9 x 7 centimeters in size. Outer surface was grey brown colored with congested blood vessels. Cut section showed a well-demarcated, homogenously solid, gelatinous, semi-translucent mass in the mid and lower pole. Tumour was exophytic. Normal renal parenchyma measured 6 x 2.5 cm at upper pole and 2.5 x 1 cm at lower pole. Attached ureter measured 7 cm in length with an outer diameter of 0.4 cm. Adrenal gland measured 5 x 2.5 x 1 centimeters. Outer and cut surfaces were unremarkable [Table/Fig-2]. Multiple sections from the mass, renal parenchyma, ureter and adrenal gland were submitted for histopathological examination. Paraffin sections were stained with Haematoxylin and Eosin stain. Immunohistochemistry was carried out with vimentin, S-100, desmin, epithelial membrane antigen (EMA) and cytokeratin (Novacastra, Leica Biosystems, UK).
Well demarcated, homogenously solid, gelatinous, semitranslucent mass in mid and lower poles and the surrounding renal parenchyma

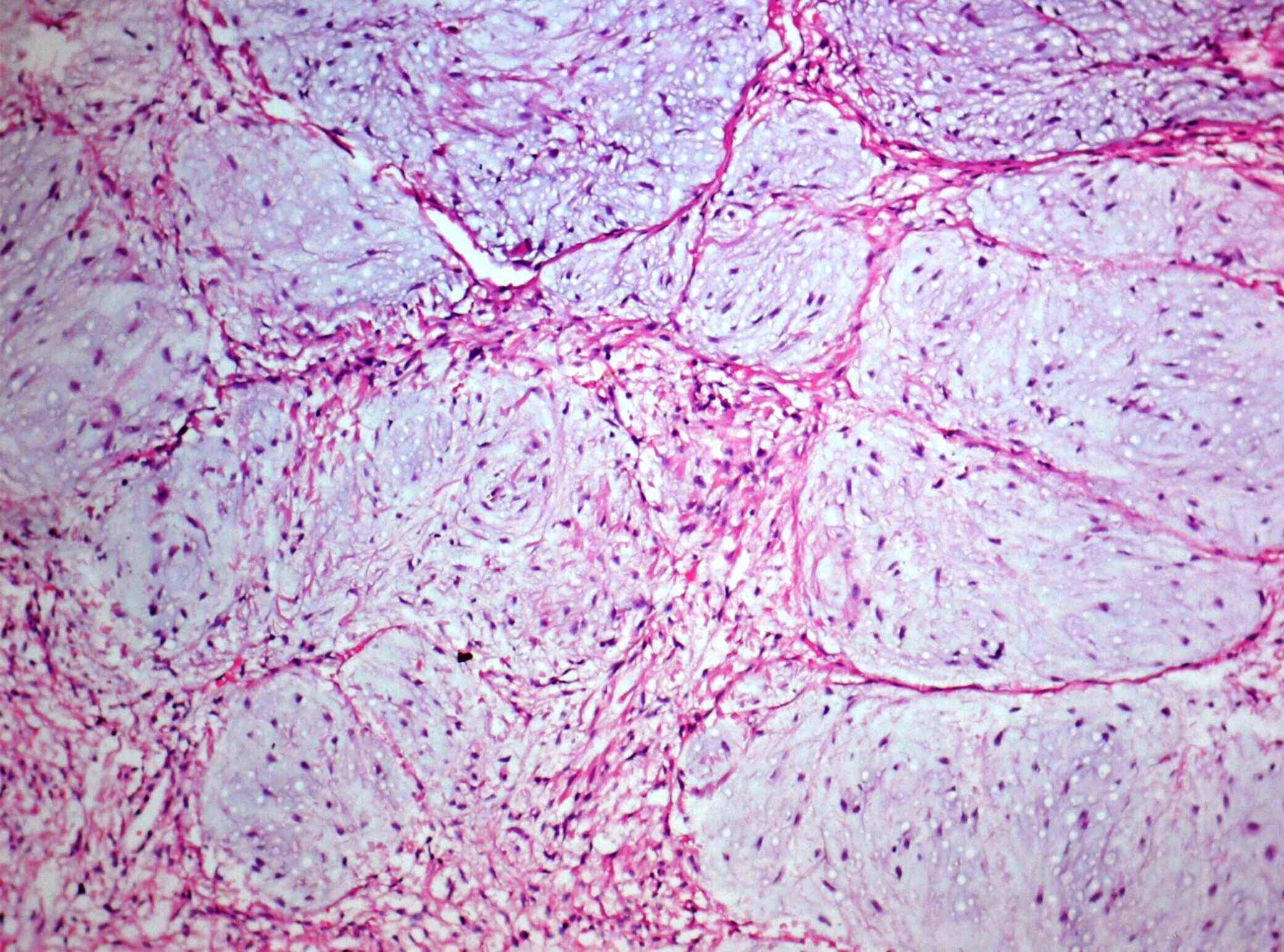
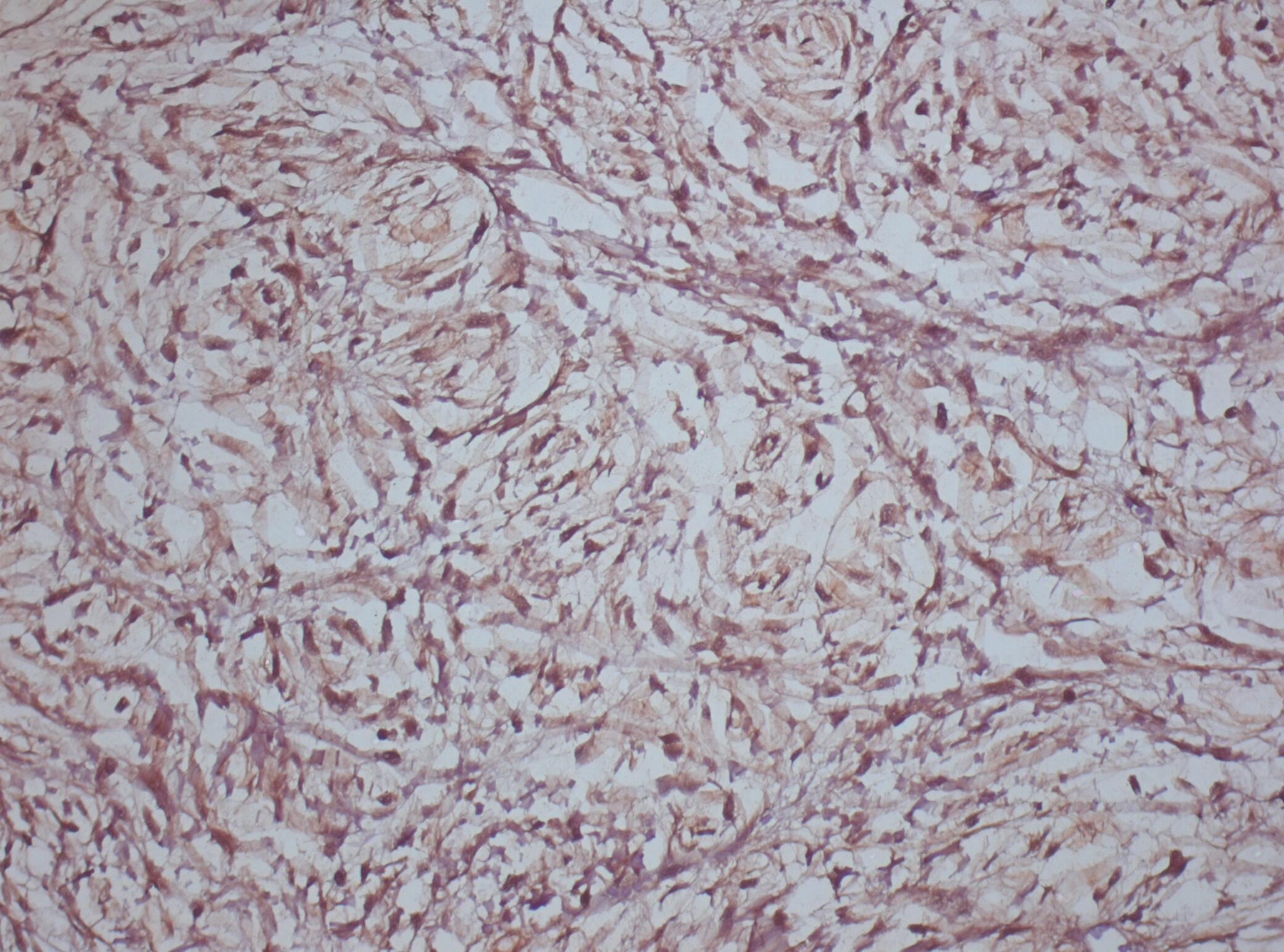
Microscopic examination revealed markedly hypocellular tumour of loose myxoid tissue with foamy histiocytes. Scattered spindle cells are seen in myxoid areas [Table/Fig-3]. Capsular invasion was absent. No atypia was evident. The adjacent renal parenchyma showed acute tubular necrosis. Ureter and adrenal gland were unremarkable. Tumor cells showed immunoreactivity for vimentin but S-100 protein, EMA, cytokeratin and desmin [Table/Fig-4]. Final diagnosis of Myxoma with acute tubular necrosis of non-tumor parenchyma was made. At eight months of follow-up, patient is well and asymptomatic.
Hypocellular appearance of loose myxoid tissue (H&E, X100)
Immunohistochemistry showing vimentin positive cells (X200)
Discussion
In 1863, Virchow gave the term ‘myxoma’ to a tumour with mucous tissue of the umbilical cord [1]. Myxomas are reported mainly in heart, soft tissues, skin, bone and other body organs. The commonest sites for myxoma are skeletal muscles of thigh and buttocks. Myxoma of kidney has been rarely reported and few cases have been documented in literature till date. In 1887, the first case of ‘a large capsular myxoma of the kidney’ was described by Hulke [2]. Data shows prevalence in male and female are nearly equal with majority of cases were asymptomatic. Few patients had pain in abdomen as a presenting symptoms as in our case. Myxoma was seen in young to elderly age [3]. Myxoma is a benign tumour of fibroblastic in origin. It has myxomatous matrix due to excessive production of mucopolysaccharides. Radiological investigations like USG, CT and Magnetic Resonance Imaging (MRI) are helpful in diagnosis and management. Due to suspicion of malignancy in these tumours, radical nephrectomy is usually carried out like in our case. However, if superior diagnostic modalities like PET CT or CT guided biopsy are available stating the benign nature of lesion, nephron sparing surgery with enucleation of the tumour would always be a preferred choice. Other tumours with features of secondary myxoma like myxolipoma, myxoid leiomyoma, perineuroma, myxoid neurofibroma, and malignant tumours like myxoid variant of malignant fibrous histiocytoma, leiomyosarcoma, rhabdomyosarcoma, and extraskeletal chondrosarcoma should be differentiated from renal myxoma [4,5]. Being benign in nature, prognosis of myxoma is good and recurrence is unheard of.
Conclusion
Renal myxoma is a rare benign genitourinary tumour with good prognosis. The present case adds up to literature with such reported cases.
[1]. Virchow R, Die Krankhaften Geschwulste 1863 Vol. 1BerlinVerlag van August Hischwald [Google Scholar]
[2]. Hulke JW, Large myxoma enclosing the left kidney, extirpated together with this organ by abdominal section, recovery, recurrence of neoplasms, and death, about 12 months after the operationLancet 1887 ii:1065 [Google Scholar]
[3]. Shah A, Sun W, Cao D, Myxoma of the kidney associated with haemorrhageIndian J Surg 2013 75(Suppl 1):480-83. [Google Scholar]
[4]. Hakverdi S, Gorur S, Yaldiz M, Renal myxoma: a case report and review of literatureTurk J Urol 2010 36(3):318-21. [Google Scholar]
[5]. Bolat F, Turunc T, Kayaselcuk F, Primary renal myxomaTurk J Pathol 2007 23:160-63. [Google Scholar]