Large Nabothian Cyst Obstructing Labour Passage
Fisun Vural1, Ilhan Sanverdi2, Ayse Deniz Ertürk Coskun3, Alim Kusgöz4, Orhan Temel5
1 Specialist, Department of Obstetrics and Gynaecology, Haydarpasa Numune Teaching Hospital, Istanbul, Turkey.
2 Specialist, Department of Obstetrics and Gynaecology, Haydarpasa Numune Teaching Hospital, Istanbul, Turkey.
3 Specialist, Department of Obstetrics and Gynaecology, Haydarpasa Numune Teaching Hospital, Istanbul, Turkey.
4 Specialist, Department of Obstetrics and Gynaecology, Haydarpasa Numune Teaching Hospital, Istanbul, Turkey.
5 Specialist, Department of Obstetrics and Gynaecology, Haydarpasa Numune Teaching Hospital, Istanbul, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Fisun Vural, Tıbbiye Cad. No:40 Üsküdar/Istanbul-34668, Turkey. E-mail : fisunvural@yahoo.com.tr
Nabothian cysts are common and silent retention cysts of the uterine cervix with no particular intervention required. It is quite rare to reach a size of more than 4 cm and it is a diagnostic dilemma to differ it from adenoma malignum. We report a case of a woman with 38 weeks of gestation presented to the maternity unit with labour pain and protruding cystic mass (60x70 mm) out of the vagina. Simple drainage was performed to allow the vaginal delivery. She delivered 4130 grams, 9-10 Apgar, male baby by spontaneous vaginal delivery. The patient’s and the newborn postpartum course was uneventful. Gynaecologic examination revealed a persisting cystic mass in the cervix (40x50 mm) two months after the delivery. We performed a total excision of the cyst to confirm the pathologic diagnosis. This paper is the first report of nabothian cysts obstructing labour passage. In the view of this case, we aimed to discuss cervical cystic masses and a review of the literature.
Cervical cystic mass, Dystocia, Retention cyst, Tumour, Uterine cervix
Case Report
A 38-year-old multiparous woman (G4 P2 A1) with 38 weeks of gestation presented to the maternity unit with labour pain and protruding mass out of the vagina. She had regular gynaecologic examinations and pap smears. There was no medical disease, medication use, history of in utero exposure to diethylstilbestrol. She was in the active phase of the labour with 4cm cervical dilatation and regular contractions. There was a mass (6x7cm) on the anterior lip of the cervix compressing the cervical canal. The mass was soft in consistency with a smooth surface protruding out of the vagina [Table/Fig-1].
Giant nabothian cyst protruding from the vagina

Firstly, we performed a simple drainage and the discharge was mucoid. Then vaginal delivery was allowed. After that, 4130 gm live male baby was born by spontaneous vaginal delivery. The postpartum course is uneventful without haemorrhagic or infectious complication.
Postpartum Follow-up
Gynaecologic examination revealed a persisting cystic mass in the cervix (40x50 mm) two months after the delivery. The mass was soft with a smooth surface penetrating deep into the cervix. This cystic mass compressed and deviated the external os.
The ultrasonographic findings of the pelvis were normal: uterus (80x65x60 mm), right ovary (35x25mm) and left ovary (33x35 mm) with a normal follicular appearance. There was a homogeneous hypoechoic cystic dilatation (40x 50 mm) in the cervix located deeply.
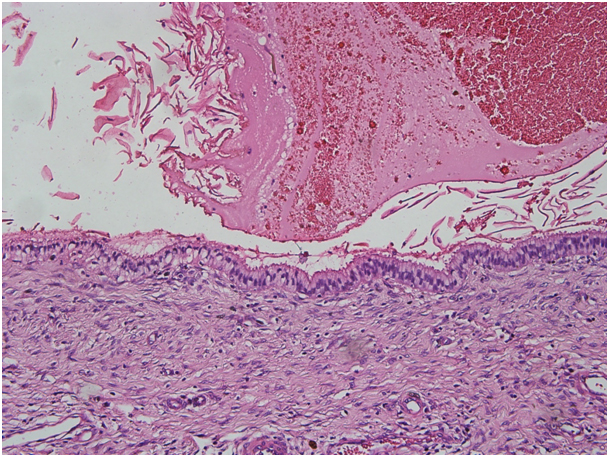
The vaginal cytologic examination was normal. We decided to excise persisting large sized cyst to exclude malignancy. We performed a total excision of the cyst under general anaesthesia. The diagnosis of nabothian cysts was done with the pathologic evaluation that showed retention cyst wall lined by ciliated columnar epithelium without atypia [Table/Fig-2] (H&E, 200X).
Nabothian cyst, the ciliated columnar epithelium without atypia (H&E, 200X)
Discussion
Nabothian cysts are a common gynaecological finding in women of reproductive age without clinical significance. They are multiple-opaque nodules (whitish to yellow) on the cervix, also called as mucinous retention cyst or epithelial cysts. It is caused by chronic inflammation of the uterine cervix. Nabothian cysts usually are small in size, it is quite rare to reach a size above 4 cm [1–3]. This paper shares a rare presentation of large nabothian cyst obstructing labour passage. Previously, few cases of large nabothian cyst have been reported in the literature [4–6]. To the best of our knowledge, this is the first report of nabothian cysts obstructing labour passage. Herein, the management of pregnant women with cystic cervical mass during labour and differential diagnosis of cervical cystic masses discussed in the view of the literature.
Cervix mainly contains fibromuscular tissue that is covered with an epithelium either squamous or columnar. The glandular or columnar epithelium covers the endocervical canal and variably extend the ectocervix. This epithelium contains the single layer of mucin-secreting cells and invaginations of this epithelium make up endocervical glands. The border between the ectocervix (stratified squamous epithelium) and the endocervical canal (columnar epithelium) is called the squamo columnar junction (SCJ) [3]. There is a continuous process of repair in the SCJ. The inflammatory process may block an endocervical gland orifice and retention cysts occur [3].
Nabothian cysts are common, non-neoplastic findings, rarely of clinical significance and are thought to occur secondarily to healing process of chronic cervicitis. There is no need for treatment intervention unless the retention cyst is symptomatic or large enough with suspicion of malignancy. Ablation is usually sufficient. However, if the diagnosis is uncertain, deep cysts or large symptomatic cysts as in this case, excision required evaluating histopathology [1–3]. Firstly, we performed simple drainage to allow a vaginal delivery. Two months after delivery, cystic mass still persisting and infiltrating deep in the cervix. Thus to exclude malignancy, we excised it completely. The differential diagnosis of a cystic mass in the cervical stroma includes adenoma malignum, deep nabothian cysts, other benign tumours of cervix and well-differentiated adenocarcinoma [3,7]. Endocervical polyps, leiomyomas, endometriosis, squamous papilloma, microglandular hyperplasia and mesonephric duct remnants are benign tumours of the uterine cervix. Cervical myomas are solitary tumours of the cervix, but may become degenerated, pedunculated through the vagina and need pathologic evaluation for diagnosis [3].
Histopathologically, nabothian cysts are lined by single layer of columnar epithelium or flattened epithelium without cellular mitosis or atypia as in our case. Huge nabothian cysts need a pathologic diagnosis to exclude other tumours of cervix and adenoma malignum that contains well-differentiated glandular cells with atypia and mitosis. Adenoma malignum (AM) is also called minimal deviation adenocarcinoma and is quite a rare phenomenon. It mimics an appearance of deep and larger sized nabothian cysts. Papanicoula smear screening and cervical punch biopsies may not detect the AM lesion. Similarly, pap smear of our case was normal. Histopathologically, the lesion shows a benign histological appearance and it contains well-differentiated mucinous glands, deeply invading the cervical stroma. Despite benign histopathologic findings, the clinical behaviour is aggressive. Thus, it is a diagnostic challenge and accurate diagnosis is important and depends on high suspicion of gynaecologist [6–8].
Conclusion
In conclusion, despite nabothian cysts are benign and common findings of gynecology practice, they may unusually present with giant mass. If the cystic mass in the cervix is large and deeply located total excision is required to exclude malignancy.
Consent and Competing Interest
This paper obeys ethical issues as informed consent and confidentiality. Written informed consent was obtained from the patient for photography and publication.
[1]. Casey PM, Long ME, Marnach ML, Abnormal cervical appearance: What to do, when to worry?Mayo Clin Proc 2011 86:147-51. [Google Scholar]
[2]. Katz VL, Lobo RA, Lentz G, Gershenson D, Comprehensive Gynecology 2007 5th EdPhiladelphia, PAMosby/Elsevier:437-438. [Google Scholar]
[3]. Malpica A, Robboy SJ, Cervical Benign and Nonneoplastic conditions in: Robboy Pathology of Female Reproductive Tract 2009 2nd EdElsevier:141-166. [Google Scholar]
[4]. Nigam A, Choudhary D, Raghunandan C, Large nabothian cyst: a rare cause of nulliparous prolapseCase Rep Obstet Gynecol 2012 2012:192526 [Google Scholar]
[5]. Temur I, Ulker K, Sulu B, Karaca M, Aydin A, Gurcu B, A giant cervical nabothian cyst compressing the rectum, differential diagnosis and literature reviewClin Exp Obstet Gynecol 2011 38(3):276-79. [Google Scholar]
[6]. Clement PB, Young RH, Deep nabothian cysts of the uterine cervix. A possible source of confusion with minimal-deviation adenocarcinoma (Adenoma malignum)Int J Gynecol Pathol 1989 8(4):340-48. [Google Scholar]
[7]. Sosnovski V, Barenboim R, Cohen HI, Bornstein J, Complex Nabothian cysts: a diagnostic dilemmaArch Gynecol Obstet 2009 279:759-61. [Google Scholar]
[8]. Ki EY, Byun SW, Park JS, Lee SJ, Hur SY, Adenoma malignum of the uterine cervix: report of four casesWorld J Surg Oncol 2013 11:168 [Google Scholar]