A Case of Intraoral Lymphangioma Circumscripta – A Diagnostic Dilemma
Dara Balaji Gandhi Babu1, B. Raj Kumar2, Niharika Harsha Boinepally3, Ashalata Gannepalli4
1 Professor and HOD, Department of Oral Medicicne and Radiology, Panineeya Mahavidyalaya Institute of Dental Sciences, Kamalanagar, Chaitanyapuri, Hyderabad, India.
2 Reader, Department of Oral Medicicne and Radiology, Panineeya Mahavidyalaya Institute of Dental Sciences, Kamalanagar, Chaitanyapuri, Hyderabad, India.
3 Student, Department of Oral Medicicne and Radiology, Panineeya Mahavidyalaya Institute of Dental Sciences, Kamalanagar, Chaitanyapuri, Hyderabad, India.
4 Professor, Department of Oral Pathology, Panineeya Mahavidyalaya Institute of Dental Sciences, Kamalanagar, Chaitanyapuri, Hyderabad, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Niharika Harsha Boinepally, Student, Department of Oral Medicicne and Radiology, Panineeya Mahavidyalaya Institute of Dental Sciences, Kamalanagar, Chaitanyapuri, Hyderabad, India. E-mail : Niharika.boinepally@gmail.com
Lymphangiomas are developmental malformations which present as benign hamartomas of lymphatic channels. They are commonly located in the head and neck region and are less frequently reported in the oral cavity. However affected sites in the oral cavity include the tongue, palate, gingiva, buccal mucosa, lips and alveolar ridge of the mandible. The most common site in the oral cavity is tongue. Lymphangioma of the buccal mucosa is rare as per the available literature and they usually occur as lobular masses or cystic lesions. Histopathologically, lymphangioma appear as proliferated lymphatic vessels lined by plump endothelial cells. Surgical excision, laser therapy and sclerotherapy are the eventual modes of treatment. This paper reports a rare case of lymphangioma of the buccal mucosa in a 60-year old male patient managed by surgical excision.
Alveolar process, Endothelial cells, Gingiva, Hamartoma, Lymphatic vessels
Case Report
A 60-year-old male patient reported to the Department of Oral Medicine and Radiology, Panineeya Mahavidyalaya Institute of Dental sciences with a chief complaint of swelling in the left cheek region which started about 6 months ago. The swelling was initially small and gradually increased to the present size. Medical and family history was not contributory. On intraoral examination, a solitary well defined swelling was present in the line of occlusion with no secondary changes on the surface and no surface colour changes. The swelling was approximately 2cm in diameter [Table/Fig-1]. On palpation, the swelling was found to be smooth, soft, fluctuant slippery and non–tender [Table/Fig-2]. On correlating the history and clinical findings, a provisional diagnosis of intraoral lipoma of the left buccal mucosa was given. Fibroma, mucocele, ectopic lymph node and benign salivary gland tumour were considered in the differential diagnosis. After taking informed consent from the patient, he was subjected to routine blood investigations and surgical excision was done under local anaesthesia [Table/Fig-3] as it was a small lesion and surgery is the mainstay of treatment. The patient was prescribed amoxicillin 500mg thrice a day and a combination of Aceclofenac 100 mg and Paracetamol 325 mg for five days. The excised specimen was sent for histopathological examination. It revealed dilated cystic spaces lined by endothelial cells containing red blood cells and eosinophilic material resembling lymph or lymphatic fluid. The spaces were of varying sizes dispersed within connective tissue stroma. A final diagnosis of Lymphangioma Circumscripta of the left buccal mucosa was given. Postoperative healing was uneventful after suture removal [Table/Fig-4] and there was no recurrence observed after 1 year follow-up [Table/Fig-5].
Intra oral photograph showing swelling in the left buccal mucosa

Photograph of the swelling during palpation with slip sign positive

Photograph showing excised lesion

Photograph showing healing after suture removal

Photograph showing after one year of follow up

Discussion
Lymphangioma is a rare benign congenital lesion of unknown aetiology. It usually originates as a hamartomatous hyperplasia of the lymphatic vessels arising from sequestration of lymphatic tissue that do not communicate with the rest of the lymphatic channels. Lymphangioma was first described by Virchow in 1854 [1]. Lymphangiomas have marked predilection for head and neck region accounting for about 75% of all cases. Approximately 50% lesions are noted at birth and 90% develop by 2 years of age of [2]. These are commonly located in the head and neck region and are rarely reported in the oral cavity. The most common affected sites in the oral cavity include the tongue, rarely on other areas like palate, gingiva, lips and alveolar ridge of the mandible [1]. Of these, the common site of occurrence of lymphangioma in the oral cavity is the tongue. Lymphangioma of the buccal mucosa is certainly infrequent [3]. Seema et al., and Dogan et al., reported cases of occurrence of lymphamgioma on buccal mucosa but with a varied clinical presentation from the present case [3,4]. Lymphangiomas usually manifest as papillary lesions having same colour as adjacent mucosa [3]. On tongue, lymphamgioma are superficial and demonstrate a pebbly surface that resembles a cluster of translucent vesicles [5] or “frog egg” or tapioca pudding appearance [6]. Vijayalaxmi et al., reported another case of lymphangiomas of palate which presented as a solitary smooth and reddish nodule [7]. But in the present case, it occurred as a solitary growth with a smooth surface on buccal mucosa. A growth of this kind can be easily misdiagnosed as a lipoma or papilloma and in most cases ignored or delayed in providing treatment. Mehmet et al., has reported a similar lesion on buccal mucosa which was bluish in colour [8]. We have not found a similar presentation so far in literature to the best of our knowledge.
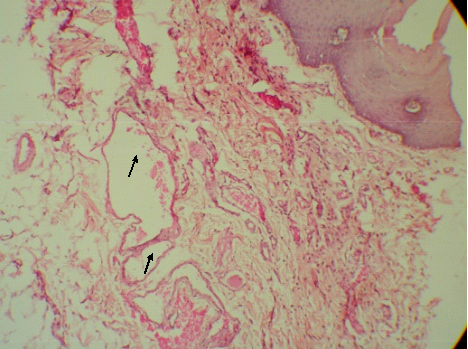
Lymphangiomas are classified clinically into macrocystic (larger than 2 cm [3]), micro cystic (smaller than 2 cm [3]) and mixed, which is a combination of the above two types [6]. Based on clinical and histological findings, lymphangiomas in the oral cavity are found to be superficial which occur as lymphangioma simplex, circumscripta and capillary type. Deep lesions are of micro cystic type [8]. In the present case, lymphangioma presented in the oral cavity at the region of buccal mucosa as a solitary swelling. On histopathological examination, lymphangioma revealed dilated cystic spaces lined by endothelial cells containing RBC and lymphatic fluid and were filled with eosinophilic material resembling lymph [Table/Fig-6,7 and 8].
Photomicrograph of H&E (10X): showing endothelial lined lymphatic channels with eosinophilic lymphatic fluid
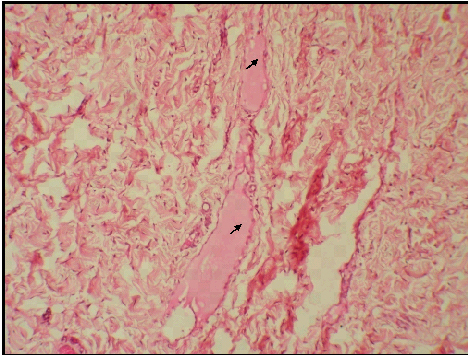
Photomicrograph of H&E (10X): showing endothelial lined lymphatic channels below the oral epithelium
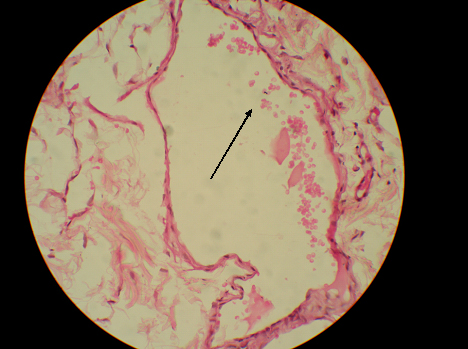
Photomicrograph of H&E (40X): showing lymphatic channel lined by spindle shaped endothelial cells
Various treatment modalities are tried such as sclerosing agents, laser therapy, cryotherapy, electrocautery, embolization and ligation. Various sclerosing agents have been tried in lymphangiomas such as hypertonic saline, 25% dextrose, sodium morrhuate, tetracycline, doxycycline, ethanol, bleomycin and OK-432. It may be pointed that OK-432, which is a lyophilized mixture of streptococcus pyogenes, is preferred as the first line of treatment for lymphangiomas than the other sclerosing agents because of the absence of perilesional fibrosis in using OK-432 [4]. Also, the use of sclerosing agents was found to cause after effects such as fever and swelling at the site of injection [4]. Because of the high fluid content in the tissues and poor blood supply, cryosurgery has also been tried for treating lymphangiomas [4]. Surgical excision is the ultimate choice of treatment for lymphangiomas as carried out in the present case as it was a small solitary growth. Surgical excision is preferred as spontaneous regression of lymphangiomas is rare [1] and most of the adult lymphangiomas are encapsulated or partially circumscribed [4]. Lymphangiomas have high rate of recurrence and in such recurrent cases intralesional injections of sclerosing agents can be given preoperatively [4].
Conclusion
The lesions involving buccal mucosa have varied presentations like papillomas, fibromas, lipomas and lesions such as a lymphangioma as reported in the present case. Sometimes rare lesions may present with a rare clinical appearance. Though rare diagnosis is rarely correct, it is the responsibility of clinician to thoroughly examine the lesions which may occur in various parts of oral and maxillofacial region and not miss the rare lesions and conditions, with the help of various diagnostic aids. The unique presentation in the histologic picture of these oral lesions always helps us in identifying such lesions which were not reported much in the literature till date.
[1]. Kheur SM, Routray S, Ingale Y, Desai R, Lymphangioma of tongue: a rare entityIndian J Dent Adv 2011 3:635-37. [Google Scholar]
[2]. Vasconcelos MG, Santos BC, Lemos LC, Ribeiro BF, Iglesias DP, Vasconcelos RG, Oral lymphangioma: Case reportRev Sul-Bras Odontol 2011 8:352-56. [Google Scholar]
[3]. Yoganna SS, Rajendra Prasad RG, Sekar B, Oral lymphangioma of the buccal mucosa a rare case reportJournal of Pharmacy & Bio allied Sciences 2014 6(Suppl 1):S188-91. [Google Scholar]
[4]. Dogan N, Durmaz CE, Sencimen M, Ucok O, Okcu KM, Gunhan O, The treatment of recurrent lymphangioma in the oral mucosa by cryosurgeryOral Health and Dent Manag Black Sea Count 2010 9(1):7 [Google Scholar]
[5]. Neville Damn, Allen Bouquot, Oral and Maxillofacial PathologSoft tissue tumours 2009 3rd editionElsevier:547-49. [Google Scholar]
[6]. Ganesh C, Sangeetha GS, Narayanan V, Umamaheswari TN, Lymphangioma Circumscriptum in an Adult: an unusual oral presentationJournal of Clinical Imaging Science 2013 3:44 [Google Scholar]
[7]. Vijayalakshmi SK, Kale AD, Satpathy Y, Lymphangioma of the Palate: A Case ReportDentistry India 2010 4(2):29-31. [Google Scholar]
[8]. Coskunses FM, Tugcu FE, Kocygit ID, Ozgul O, Karadeniz SN, Lymphangioma of buccal mucosa: an unusual caseInt J Dent Clin 2012 4(1):50-1. [Google Scholar]