Serous Microcystadenoma of Pancreas
Puvitha Rajeswari Duraisami1, Vinuta Malaichamy2, Lalitha Chithambaram3
1 Senior Assistant Professor, Department of Pathology, Coimbatore Medical College, Coimbatore, Tamil Nadu, India.
2 Senior Assistant Professor, Department of Pathology, Coimbatore Medical College, Coimbatore, Tamil Nadu, India.
3 Professor and Head, Department of Pathology, Coimbatore Medical College, Coimbatore, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. R.D. Puvitha, 9-Kappiniya Gounder Layout, M.K.P. Colony, Ganapathy, Coimbatore, Tamil Nadu-641006, India.
E-mail: drrdpuvitha@yahoo.com
Cystic tumours of the pancreas are less common, representing 5% to 10% of all pancreatic neoplasms. They constitute an important subset because many cystic tumour are either benign or low-grade (indolent) malignant neoplasm. Cystic lesions are also detected more commonly owing to the increased use of sensitive imaging techniques. A female patient 48-year-old, presented with upper abdominal symptoms. CT abdomen reveals a large multicystic mass with central scar shows no communication with pancreatic duct. Resected specimen, show a large lobulated mass with central scar and many small cysts. Microscopic examination confirms the diagnosis of serous adenoma. PAS positivity is used to demonstrate the glycogen content of the lining epithelium.
Cystic neoplasm, Cystadenoma, Pancreas
Case Report
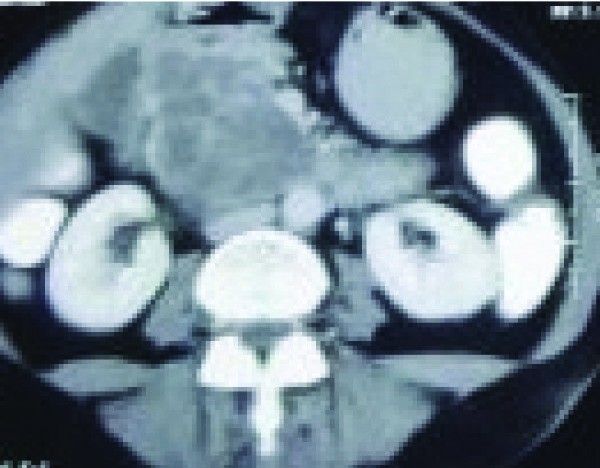
A 48-year-old female presented with upper abdominal pain, nausea and vomiting for about two weeks duration. No relevant past and family history. Clinical examination was inconclusive. So, investigations were done; ultra sonogram of abdomen showed a huge mass around the duodenum and the head of pancreas. CT abdomen was done to locate the site; it revealed a large multicystic lesion with central scar in the pancreatic head, measures app. 5.6x6.2x7 cm, show no communication with pancreatic ducts [Table/Fig-1]. Findings were suggestive of serous cystic neoplasm of pancreas. Patient underwent Whipple’s procedure. We have received resected specimen of pancreas with portion of small intestine and gall bladder measures 14x8x6 cm. Cut surface revealed an apparently encapsulated, lobulated lesion measuring 7x6x5 cm, with multiple tiny cysts with central stellate scar [Table/Fig-2]. Histopathological examination revealed, multiple cysts lined by low cuboidal epithelium, along with few glycogen- rich clear cells arranged in a single flat layer without atypia [Table/Fig-3]. These features validated the diagnosis of serous micro cystadenoma of pancreas. Histochemistry of Periodic acid Schiff stain positivity demonstrates glycogen content of cells [Table/Fig-4]. Patient was reviewed periodically for about a year, showed symptom free and healthy.
CT abdomen show a hypodense, lobulated lesion in the head and uncinate process of pancreas, measuring 10x8 cm. Multiple septae are seen within the lesion with enhancement
Gross appearance show circumscribed, lobulated lesion measuring 11x9 cm with multiple tiny cysts and central stellate scar

Histopathological examination showing multiple cystic spaces are lined by low cuboidal epithelium (H&E, 10X)

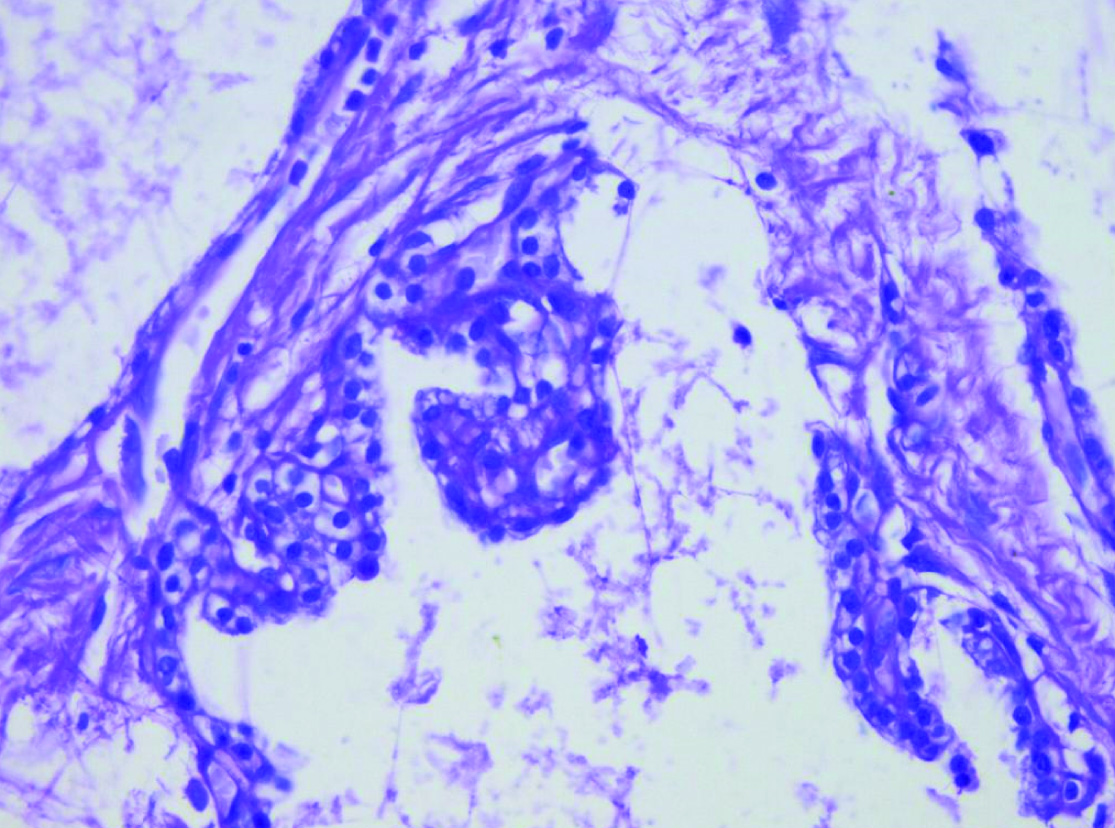
Shows histochemistry by PAS demonstrates intracytoplasmic glycogen (40X)
Discussion
Most of the cystic lesions of pancreas are developmental or inflammatory in origin and only 10 to 15% represents true neoplasm [1,2]. Serous cystic neoplasm constitutes the most common type of ‘true’ cystic neoplasm of the pancreas. Common presenting symptoms are abdominal mass along with pain, nausea, vomiting and jaundice [3]. This patient also presented with similar symptoms. Forty percent of the cases were asymptomatic and detected only incidentally. SMCA is usually solitary but can be multiple or diffuse, with wide ranges of size from 1-25 cm. Current diagnostic modalities like CT abdomen are helpful for pre operative diagnosis. In this it revealed a large circumscribed, multicystic lesion with central scar in the pancreatic head, measures app. 5.6x6.2x7 cm, show no communication with pancreatic ducts [4,5]. The tumour is encapsulated, slightly bosselated and a circumscribed lesion. On section the neoplasm shows multiple cysts with honeycomb appearance. The cysts are filled with serous fluid and ranging from 0.1 cm to 2 cm in diameter and arranged around a central scar [4]. Sometimes with micro calcifications that represent the counterpart of the “Sunburst” pattern identified on imaging studies [4].
Histopathological examination shows, microcystic areas with honeycomb appearance, these cysts are lined by low cuboidal epithelium to flattened cells. They show clear cytoplasm with centrally placed nuclei in focal areas. Intracytoplasmic glycogen content is well demonstrated by special stain like by Periodic Acid Schiff stain (PAS stain) without diastase and Alcian blue stain are negative [5,6].
Serous neoplasms should be differentiated from pancreatic pseudo cysts, lymphangiomas, solid pseudo papillary tumours, renal cell carcinoma with clear cells, and clear cell endocrine tumours [7,8]. Pancreatic pseudo cyst is common cystic tumour of pancreas in that, the wall show inflammatory cells without epithelial cell lining. Pseudo microcytic pattern sometimes present in lymphangioma, but histologically lymphoid follicles and occasional bundles of smooth muscle are present in the stroma. These cells are positive for factor VIII related antigen, CD 34 and other endothelial marker [9]. Renal cell carcinoma typically large cells with less regular nuclei are not organized into a micro cystic pattern [10]. In solid pseudo papillary tumours, the cells lack glycogen, the nuclei are usually ovoid (some with a groove) and the pseudo micro cysts are actually multiple small foci of loose connective tissue. These tumours are usually invasive at their borders. Degenerative cystic changes in solid pseudo papillary tumour of pancreas may confuse, but these cystic spaces lack epithelial lining and they occur predominantly in young women [11]. Clear cell endocrine tumour of pancreas is characterized by multisystem spongy appearance, but it lacks stellate scar and it has acinar cell differentiation [6].
Multiple sections studied should be taken to rule out the possibility of endocrine neoplasia associated with SMCA, because SMCA admixed with pancreatic endocrine neoplasm has a higher malignant potential than pure SMCA [6].
Conclusion
Cystic lesions are also detected more commonly owing to the increased use of sensitive imaging techniques. As the rule, cystic serous neoplasm was diagnosed earlier by imaging techniques and the patient was promptly treated. The tumour was confined to the organ and no metastasis made out. Literatures say that in the absence of demonstrable metastases, typical case of a serious neoplasm should be considered benign. Symptomatic recovery of the patient was promising and the follow-up counts to the viable option.
[1]. Compton CC, Serous cystic tumours of the pancreasSemin Diagn Pathol 1978 69:289-98. [Google Scholar]
[2]. Jacob S, Rawat P, Mark RP, Serous microcystic adenoma (glycogen rich cystadenoma) of the pancreasIndian J Pathol Microbiol 2010 53(1):106-08. [Google Scholar]
[3]. Mandvekar AS, Amarapurkar AD, Shenoy AS, Balsarkar DJ, Serous microcystic adenoma of pancreasIndian J Gastrentrol 2011 30(4):183-84. [Google Scholar]
[4]. Clores MJ, Thosani A, Buscaglia JM, Multidispilinary diagnostic and therapeutic approaches to pancreatic cystic lesionsJ multidiscip Health C 2014 7:81-91. [Google Scholar]
[5]. Pyke CM, Van Heerdan JA, Colby TV, Sarr MG, Weaver AL, The spectrum of serous cystadenoma of pancreas. Clinical, pathological and surgical aspectsAnn Surg 1992 215(2):132-39. [Google Scholar]
[6]. Slukvin II, Hafez GR, Niederhuber JE, Warner TF, Combined serous microcystic adenoma and well differentiated endrocrine pancreatic neoplasm: a case report and review of literatureArch Pathol Lab Med 2003 127(10):1369-72. [Google Scholar]
[7]. Koksal AS, Asil M, Turhan N, Yolcu OF, Kucukay F, Akolu M, Serous microcystic adenoma of the pancreas:case report and review of the literatureTurk J Gasterol 2004 15(3):183-86. [Google Scholar]
[8]. Agarwal N, Kumar S, Dass J, Arora VK, Rathi V, Diffuse pancreatic serous cystadenoma associated with neuro endocrine carcinoma:a case report and review of literatureJournal of Pathology 2009 10(1):55-58. [Google Scholar]
[9]. Appledaum B, Cunningham JT, Two cases of cystic lymphangioma of the pancreas: a rare finding in endoscopic ultrasonographyEndoscopy 2006 38:E24-25. [Google Scholar]
[10]. Thompson LDR, Heffess CS, Renal cell carcinoma to the pancreas in surgical Pathology materialCancer 2000 89:1076-88. [Google Scholar]
[11]. Papavramidis T, Papavramidis S, Solid peudopapillarytumours of the pancreas: review of 718 patients reported in English literatureJ Am Coll Surg 2005 200:965-72. [Google Scholar]