Materials and Methods
This prospective study was conducted from April 2010 to December 2013 at a university- affiliated teaching hospital. The procedure was performed in accordance with the ethical standards of the institutional ethics committee. Informed written consents were obtained from all the patients participating in this study.
A total of 29 patients who were diagnosed to have a benign thyroid disease that required thyroidectomy and were euthyroid were included in this study. Patients with malignant thyroid disease, very large goiter and morbid obesity were excluded from the study. All the 29 patients underwent preoperative evaluation.
All the 29 surgeries were performed by the same surgeon to maintain uniformity. Twenty patients underwent thyroid surgery under cervical plexus block (CPB) and nine patients under cervical epidural anaesthesia. (CEA)
Both sets of patients were sedated with 30 mg pentazocine (fortwin) and 2mg midazolam. Oxygen was supplied at the rate of two to four liters per minute.
The intraoperative parameters like oxygen saturation, pulse rate, blood pressure and respiratory rate were monitored and recorded every ten minutes. Postoperative pain was calculated using visual analogue scale.
Technique of deep cervical plexus block: The face of the patient was turned to the side away from the required hemi thyroidectomy. The neck was kept in slight extension. A line was drawn from the mastoid process to chaissagnacs tubercle. A second line is drawn parallel to but 1 cm behind first line as shown in [Table/Fig-1]. C4 transverse process was identified. A 22 gauge needle was used to confirm paraesthesia at the site and10 to 12 ml of local anaesthesia was introduced.
Cervical plexus block marking

Note: Only hemi thyroidectomies were conducted under cervical plexus block to avoid the risk of bilateral phrenic nerve palsy.
Technique of Cervical Epidural Anaesthesia: The patient is made to sit with forehead resting on the edge of a table with chin touching sternum. The spine of C7 vertebrae is identified. The skin and subcutaneous tissue in C7 and T1 intervertebral space is infiltrated with 2% lignocaine. An 18 gauge Tuohy needle is inserted in the C7 – T1 intervertebral space perpendicular to the skin as shown in [Table/Fig-2].
Epidural catheter in place

Abutment of needle onto ligamentum flavum is felt at approximately 3.5 to 5.5 cm. The needle placement is performed by loss of resistance technique or hanging drop method. An epidural catheter is guided through the tuohy needle and advanced. A 5 cm of the catheter is left inside the space as shown in [Table/Fig-3].

The patient is placed in supine position. Ten milliliter of two percent of lignocaine with 1:2,00,000 adrenaline is injected through the catheter.
At the end of the surgery, ten milliliter solution of two percent lignocaine and two milliliter of 100mg tramadol is given sixth hourly on the first day followed by eighth hourly on the second day. [Table/Fig- 4,5] show excised thyroid specimens under CPB and CEA respectively.
Excised thyroid specimen –CPB

An excised thyroid specimen under CEA
Results
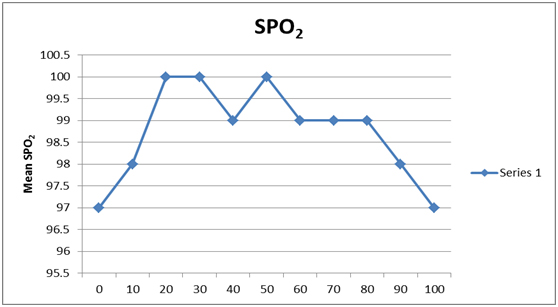
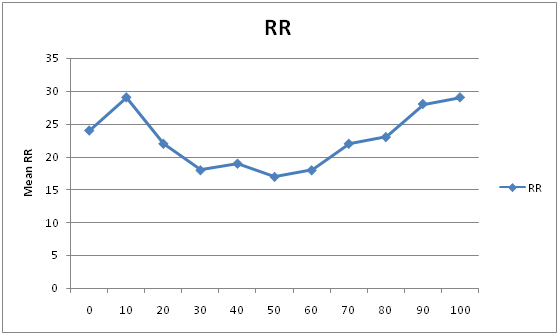
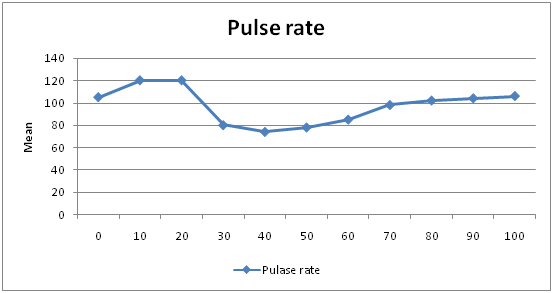
Thyroidectomy under CPB: A total of 20 patients in the age group of 22-54 years with the sex ratio of 1:3 underwent thyroidectomy (twelve right hemi thyroidectomy and eight left hemi thyroidectomy) under CPB [Table/Fig-6]. All vital parameters were within normal limits as shown in [Table/Fig-7,8,9 and 10]. No complications were encountered during the surgery.
Baseline characteristics of study group
| Cervical plexus block | Cervical epidural anaesthesia | Z-value | p-value |
|---|
| Age, mean ± SD | 31.4(mean);8.519(SD) | 33.9(mean);10.856(SD) | 0.6171 | 0.53 |
| Sex ratio (male :female) | 1:3 | 1:3 | | |
| Surgical procedure Total Thyroidectomy | 0 | 3 (33.3%) | | |
| Hemithyroidectomy | 20 (60% right, 40%left) | 6 (44.5%right, 22.2%left) | | |
Showing variation in SPO2 in CPB groups
Showing variation in RR in CPB groups
Showing variation in Pulse Rate in CPB groups
Showing variation in SBP & DBP in CPB groups
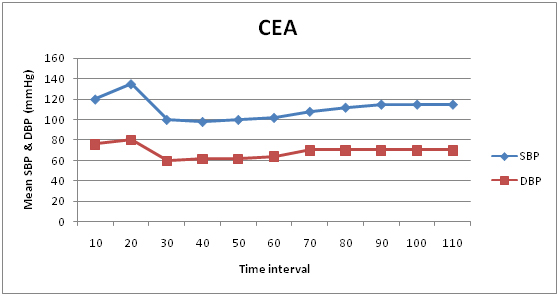
Thyroidectomy under CEA: A total of nine patients in the age group of 22-54 years with the sex ratio of 1:3 underwent thyroidectomy (four right hemi thyroidectomy, two left hemi thyroidectomy and three total thyroidectomy) under CEA [Table/Fig-6]. All vital parameters were within normal limits as graphically depicted in [Table/Fig-11,12,13 and 14]. No complications were encountered during the surgery.
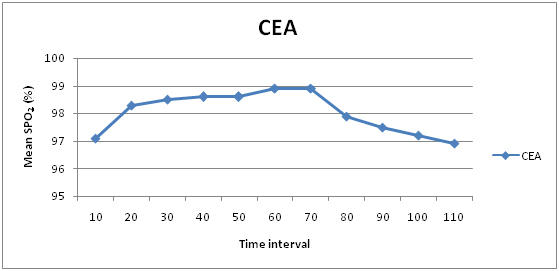
Variations in SPO2 in CEA groups
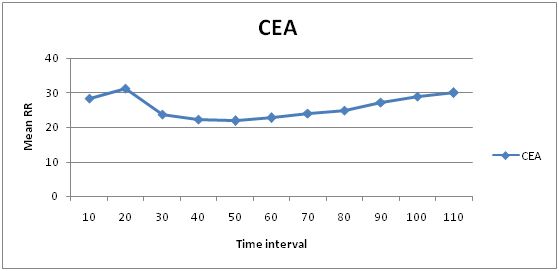
Variations in RR in CEA groups
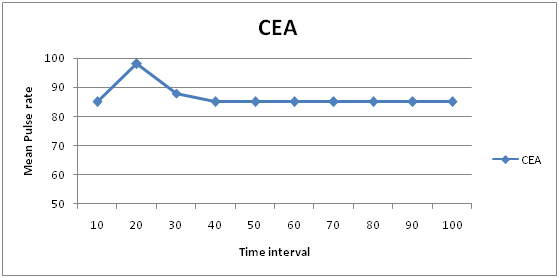
Variations in Pulse rate in CEA groups
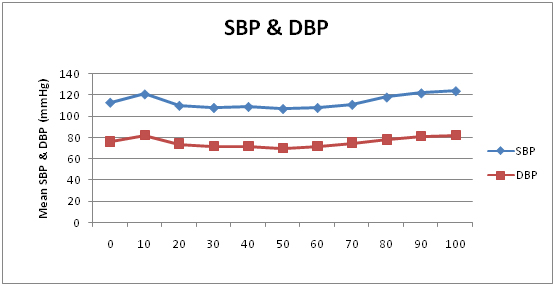
Variations in SBP & DBP in CEA groups
In our study, the surgeon was at ease as he was able to monitor the recurrent laryngeal nerve during the procedure. There was adequate muscle relaxation and the primary surgeon was able to conduct the surgery with a mean duration of 56 minutes for cervical plexus block and 55.56 minutes for cervical epidural anaesthesia [Table/Fig-15]. There did not arise any need for repeat anaesthesia. The patients were comfortable during the surgery. The patients had less pain with no nausea or vomiting during the postoperative period and were able to ambulate early. The duration of their hospital stay was also considerably less. There was no considerable statistical difference between the two regional anaesthetic techniques in terms of time taken to perform the surgery (p-value – 0.9365), hospital stay (p-value - 0.5684) and patient satisfaction (p-value – 0.9011) as illustrated in [Table/Fig-15].
Main outcomes of the study
| Outcome | Cervical plexus block | Cervical epidural anaesthesia | Z-value | p-value |
|---|
| Operative time | 56 minutes | 55.56 minutes | 0.0796 | 0.9365 |
| Hospital stay | 33.6 hours | 37.90 hours | -0.5704 | 0.5684 |
| Patient satisfaction(1/2/3/4/5)* | 3.6 | 3.556 | 0.1243 | 0.9011 |
*A verbal scale of 1 to 5 – 1 being unsatisfactory to 5 being most satisfied
Discussion
The results of our study are in concordance with studies conducted in the past [7–10]. Ahsan et al., had used CEA for a 65-year-old lady with a huge thyroid with aortic stenosis and at risk cardiac status [9]. Navaid Akhtar et al., performed thyroidectomy under regional anaesthesia on a 72-year-old male who was diagnosed to have follicular cell carcinoma of the thyroid with a severely compromised cardiac function [10].
Regional anaesthesia reduces the risk associated with general anaesthesia such as the risks associated with endotracheal intubation and the untoward effects of anaesthetic agents. This is particularly beneficial in singers and public speakers, because endotracheal intubation has shown to cause vocal cord changes in up to 5% of patients [6]. In addition to this it also allows the surgeon to monitor the patients vocal cord status and provides excellent postoperative analgesia. It also speeds up the post anaesthesia recovery when compared to general anaesthesia. Lo Gerfo et al., described their experience with outpatient thyroidectomy in 76 of 134 patients, discharged the same day after postoperative evaluation period of 4 to 8 hours. They included 21 patients undergoing total thyroidectomy in the outpatient group [11].
Regional anaesthesia is a good option in war torn countries, risk of fire on using general anaesthesia, unavailability of anaesthetic drugs [12]. Regional anaesthesia can also be used in patients with altered thyroid hormone status, where GA is contraindicated. In a study conducted by Lee JH et al., regional anaesthesia has also been shown to be useful in patients with compromised cardiac status and those with obstructive symptoms secondary to a large goiter to avoid the risks of a difficult intubation [13].
However, regional anaesthesia does present a few disadvantages including the risks of spinal or epidural injections, neuropraxia, haematoma formation etc [14]. Fortunately, we did not encounter any of these complications in our present study. Nonetheless, the risk of complications with regional anaesthesia cannot be overruled as the size of the population included in our study is relatively small. David J Terris et al., in their article have enumerated the advantages and disadvantages of thyroid surgery. They have also listed the selection criteria for performing thyroidectomies under regional anaesthesia [15].
The routine use of CEA in thyroid surgeries is avoided because of the fear of its potential complications. These include its effect on the respiratory function, heart rate and haemodynamic stability. CEA has also been found to attenuate the pancuronium induced tachycardia as a result of cardiac sympathetic denervation [16]. The cardiovascular stimulatory effect of Ketamine is also suppressed partially by CEA [17]. None of these adverse effects were seen in our study and is consistent with the study conducted by Khanna R et al., [18].
CPB is a relatively low risk procedure. The risk of the more serious complications is relatively less and the side effects that do occur more frequently are almost always of little significance [19]. There were no complications encountered in our study. Bilateral CPB was avoided in our studies to avoid the chance of bilateral phrenic nerve palsy. CPB has been used by lindt et al., for high risk for GA patients. They also used CPB for thyroidectomy patients who wished to return home in a day after the surgery. The considerations which have to be kept in mind while taking up a thyroid patient for CPB are the type of personality of the patient, extent of the disease and infrastructure available to the operating surgeon [12].
Patient cooperation is of utmost importance while performing surgeries under regional anaesthesia. Hence careful patient selection, preoperative psychotherapy and reassurance play a crucial role. Likewise patients with chronic cough cannot be taken up for thyroid surgery under regional anaesthesia. Other contraindications for thyroid surgery under regional anaesthesia include thyroids with retrosternal extension, malignancies of thyroid and the need for neck dissection [19,20].
Studies have shown that regional anaesthesia markedly reduces the operative time and the period of hospitalization. Data provided by various authors give an operative time ranging from 80 to 112 minutes depending on the extent of surgical resection needed [9,21,22]. In our study, the mean operative time for CPB and CEA was 56 minutes and 55.56 minutes respectively. Short hospital stay is one of the major advantages of this procedure. Many authors have reported the average hospital stay of 8-10 hours [12,23]. In our study the mean period of hospitalization was 33.6 hours for CPB and 37.9 hours for CEA respectively. The relative longer period of hospitalization can be attributed to the fact that most of the patients involved in our study were hailing from far off villages where the access to medical care was limited.
It is the patient’s satisfaction with the anaesthetic technique and the surgical procedure, which is our ultimate objective. In our study, the patient satisfaction as interpreted by the verbal scale of 1/2/3/4/5 was fairly good. In a study conducted by Samuel K Synder et al.,, the patient satisfaction was 93% when compared to 89% with general anaesthesia and surgical experience was 89% and 86% respectively [7].
Through the limited available data, it appears thyroidectomy under regional anaesthesia is cost effective [24–26]. Spanknebel et al., demonstrated anotable average cost difference for local anaesthesia ($2,974) versus general anaesthesia ($4,412) [26]. In our study the operating time and hospital stay was reduced. Both these parameters indicate a reduced operative cost. In a developing country like India where resources are limited and most of our patients belong to the lower socioeconomic group, lowering the cost of a surgery will be beneficial to the community.
Limitation
The major limitation of our study is the relatively small study size. The outcome of our study in terms of patient’s comfort and surgeons ease in performing the surgery was considerably good. This study was performed to emphasize on the efficacy of regional anaesthesia techniques in thyroid surgeries. However, further studies with a larger study size and a longer followup are entailed.
Conclusion
In our study, Regional anaesthesia (Cervical epidural anaesthesia and cervical plexus block) has been shown to be safe and effective in routine thyroidectomies, at the hand of our surgeon. With careful patient selection and adequate reassurance, regional anaesthesia can be offered as an alternative tool to patients undergoing routine thyroid surgeries.
*A verbal scale of 1 to 5 – 1 being unsatisfactory to 5 being most satisfied