To compare the safety and efficacy of expectant management of early pregnancy miscarriages with surgical uterine evacuation.
Materials and Methods
The study was conducted in a tertiary care centre for 5 years and included 212 patients with USG confirmed pregnancy miscarriages which were of less than 13 weeks duration. Ethical approval for the study was obtained from MES Medical College Ethical Committee.
The USG criteria for pregnancy miscarriage [6–8].
Anembryonic pregnancy (Gestational sac with a mean diameter of at least 20 mm, without any embryonic/extra embryonic structures).
Early fetal demise {CRL (crown-rump length) of at least 6mm with no cardiac activity or no change in size in the weekly serial scanning}.
Incomplete miscarriage (Disrupted endometrial echo of more than 15 mm measured in the antero-posterior plane, with the presence of heterogeneous and irregular tissues).
Exclusion criteria: Patients with gestational age of more than13 weeks, severe vaginal bleeding, severe abdominal pain, fever and chronic illnesses were excluded from the study.
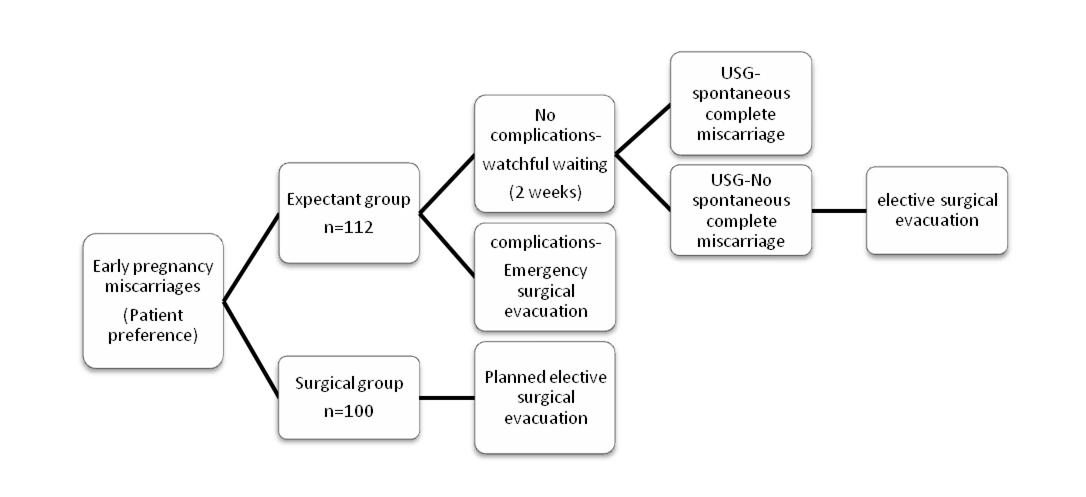
After an initial clinical examination, the patients were counseled and allowed to choose their preference between expectant management, medical management surgical management. Of the 112 patients who opted for expectant management and gave written informed consent, 7 patients changed their option to surgical management and 5 patients lost follow up. Injection Tetanus Toxoid was given to all patients and Anti- D was given to Rh negative patients.
Patients who opted for expectant management were managed as outpatients without any intervention for a period of two weeks, after which a repeat ultrasound was done to ascertain spontaneous complete miscarriage (the USG criteria for complete miscarriage being endometrial thickness of less than 15mm measured in the anteroposterior plane associated with the cessation of heavy bleeding and pain) [6–8]. Patients were counseled about the possible untoward symptoms during the waiting period, mainly severe bleeding per vaginum, severe abdominal pain, discharge per vaginum or fever and were instructed to report immediately in case they experience any of them. A pamphlet explaining the same was also handed over to the patients. Antibiotic prophylaxis was given to all patients. Emergency admission and surgical evacuation was done as indicated, if the patients became symptomatic in the waiting period. Patients with failed expectant management at the end of two weeks underwent planned surgical uterine evacuation (Dilatation and evacuation). Surgical Group: Underwent planned surgical evacuation (dilatation and evacuation), once diagnosed. Re-evacuation is considered failed surgical management [Table/Fig-1].
All the patients were followed up for 6 more weeks by clinical examination and by urine pregnancy test.
Outcomes measured were: (1) Success rate; (2) Vaginal bleeding-assessed by pictorial blood loss assessment chart; (3) Abdominal pain-assessed by visual analogue scale; (4) Need for emergency evacuation; (5) Limitation of physical activity (questionnaire); and (6) Patient satisfaction (questionnaire).
Statistical Analysis
Statistical analysis was done using Z-test. Here the hypothesis is- ‘There is no significant difference between two population proportions’ or P1 = P2. We apply Z-test by formula (P1 – P2)/S.E, where P1 and P2 are proportions of two samples. Standard Error =√P0*Q0*(1/n1*1/n2).
Results
A total of 212 patients were studied, who were allocated to expectant management (cases, n=112) and surgical management (controls n=100). Seven patients from expectant group changed their option to surgical management during the waiting period and 5 lost follow up. The patients in both the groups were comparable in relation to age, parity and gestational age [Table/Fig-2]. Of the total 212 patients studied, 16% were of middle class and 84% were of low class socio economic status.
Patient characteristics in the study
| Expectant group | Surgical group |
|---|
| Age | 25.22(+/-) 4.86 years | 25.52 (+/-) 5.46 years |
| Parity |
| Nulliparous | 61% | 56% |
| Multiparous | 39% | 44% |
| Gestational age |
| <8 weeks | 26% | 26% |
| 8-12 weeks | 49% | 51% |
| >12 weeks | 25% | 23% |
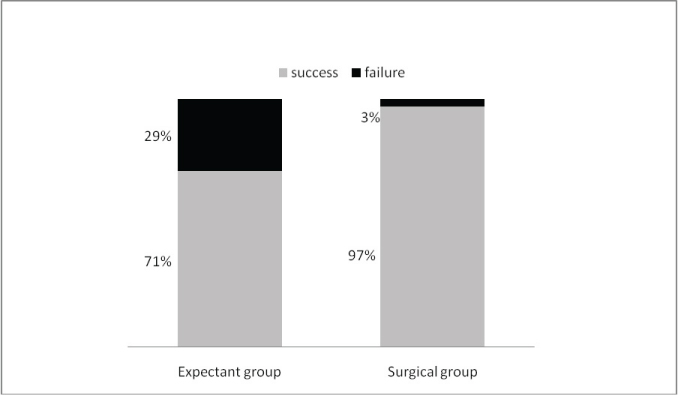
Comparison of Outcome in expectant and surgical group: In the expectant group the cumulative success rate was 71% as against 97% in surgical group. The p–value calculated was more than 0.05 [Table/Fig-3].
Comparison of success rate in two groups
Majority of patients in the study group had only mild bleeding - 80% in expectant group and 83% in surgical group. Fifteen percent of expectant and 12% of surgical group had moderate bleeding. Five percent of patients in each of expectant group and surgical group had severe bleeding. Two patients in surgical group had severe bleeding which required blood transfusion; were as none required blood transfusion in expectant group. The severe bleeding assessed was during and soon after the procedure. The severe bleeding in 2 groups was statistically significant with a p-value less than 0.05. The average time for cessation of bleeding was around 5 to 14 days in expectant group and 7 to 8 days in surgical group. Most of patients in both expectant and surgical group had only mild bearable pain. Eight percent of patients in expectant group experienced severe pain in comparison to 4% in surgical group (p<0.05).
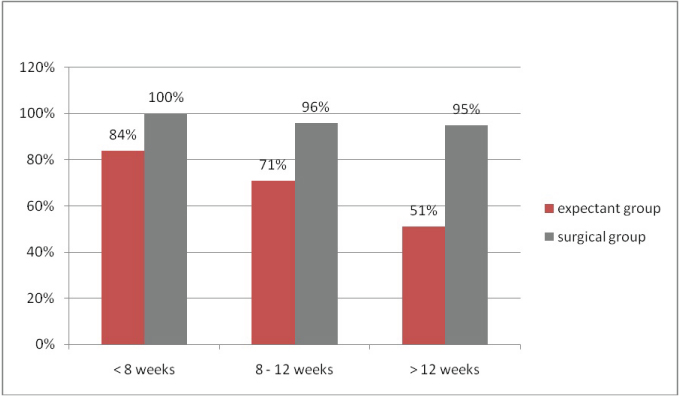
The rate of emergency evacuation in expectant group was found to be 9% as against 1% in surgical group. This finding is statistically significant with a p-value of <0.05. Twenty one percent of patients in expectant group and 17% patients in surgical group experienced limitation of physical activity (p<0.05), but this was only mild and was mainly due to pain. Patient dissatisfaction level among two groups was also statistically significant. The dissatisfaction rate was 26% in expectant group as against 20% in surgical group. The complication rates in two groups are given in [Table/Fig-4]. There was no incidence of cervical tear or uterine perforation in those who underwent surgical uterine evacuation in either group. The outcome in expectant group, according to gestational age clearly showed a decrease in success rate with increase in gestational age [Table/Fig-5].
Comparison of complications in expectant and surgical group
| Complications | Expectant group (%) | Surgical group (%) |
|---|
| Severe Bleeding | 5 | 5 |
| Severe Pain | 8 | 4 |
| Emergency evacuation | 9 | 1 |
| Limitation of physical activity | 21 | 17 |
| Patient dissatisfaction | 26 | 20 |
Comparison of success rate according to gestational age
Discussion
Early pregnancy miscarriages can be dealt with by three different methods-Surgical and medical management, the most commonly practiced options and expectant management; the most natural method. Surgical uterine evacuation is considered the gold standard management in spontaneous miscarriage; being definitive and predictive, relatively safe with a success rate of 90-100% with obvious advantage of immediate cure. There are disadvantages like the need for hospitalization and anaesthesia, risk of perforation, excessive bleeding, need for re-evacuation, sepsis, intrauterine adhesions, oligo/amenorhoea and subfertility, which encouraged clinicians to investigate the use of non-surgical options [9–12].
Medical agents with (oral/vaginal misoprostol/mifepristone) for the management of women with spontaneous miscarriage demonstrated efficacy with a success rate of 76-82%, with advantage of being non-invasive. The acceptability of medical methods is still questioned by the need for re-admission, excessive bleeding, crampy pain, gastrointestinal manifestation like nausea, vomiting and diarrhoea and other problems encountered like pyrexia, postural hypotension and sepsis [13–15].
Recently reports on expectant management of women with spontaneous miscarriage demonstrated efficacy and safety for selected case of first trimester spontaneous miscarriages, compared to the surgical uterine evacuation and has generated new interest as an alternative management options in terms of women’s acceptability, safety in the short and long term, and the health economic implications [1–12,16–19].
In our study the cumulative success rate of the expectant group was 71% as against 97% in surgical group (p-value> 0.05). From this study we cannot conclude that, the higher success rate of surgical group is statistically significant when compared to expectant group. This outcome is comparable to the study conducted by Luise et al., and H Sagili; where the success rate of expectant management was 70% when compared to 96.7% of surgical management [9,10].
The success rate reported in randomized trials for women with miscarriage managed expectantly varied between 79 and 100%. The success rate for women with incomplete miscarriage varied between 79 and 100% and for women with early fetal demise and anembryonic pregnancy ranged between 25% and 84% [1,4,5,8,11,12,16]. The success rate was 77% at 2 weeks, which rose to 93% after 7 weeks of expectant management [6]. In our study, expectant group clearly showed a decrease in success rate with increase in gestational age indicating that, selection of patients for expectant management needs to be adjusted according to gestational age. Success rate of expectant management increased with lesser gestational age, incomplete miscarriages and with longer waiting period [6–9].
The incidence of different complications like haemorrhage, emergency curettage for haemostatic uterine evacuation, suspected genital tract infection, unplanned admissions in expectant management varied from 1% to 8%, compared to 2% to 13% reported for women managed by surgical uterine evacuation [1–11,15,16].
The rate of severe bleeding in our series, in both expectant and surgical group was 5% which was statistically significant with a p-value of <.05 and was comparable to the study reported by Wieringa–de Waard et al., of 4% and 3.9% in expectant and surgical group [16].
The rate of emergency evacuation of 9% in expectant group (p-value <.05) was comparable to emergency evacuation rate of 6% and 16% reported by Hurd et al., and Jurkovic et al., respectively [17,20]. Twenty one percent of patients in expectant group and 17% patients in surgical group experienced limitation of physical activity (p<0.05), but this was only mild and was mainly due to pain. Patient dissatisfaction level among two groups was also statistically significant the dissatisfaction rate was 26% in expectant group as against 20% in surgical group.
A study on HQRL (Health related quality of life) in expectantly managed group by Weiringa De Waard showed that, women with a miscarriage who chose their own treatment had the best HRQL over time, supporting the role of free choice from a clinical point of view. Women without a treatment preference should be encouraged to start with expectant management for psychological reasons [18,19]. In our study, patients who were dissatisfied were; those patients in whom conservative management ended in failure, or emergency evacuation, or who had severe pain or bleeding. Issues of waiting period and psychological trauma were dealt with by detailed reassuring counseling sessions.
There was no incidence of cervical tear or uterine perforation in either group. The occurrence of infection rate in both groups could not be assessed, as the patients were under antibiotic coverage during this duration. In the recent MIST trial (2005), the incidence of gynaecological infection after surgical, expectant, medical management of first trimester miscarriage is low (2-3%), and no evidence exists of a difference by the method of management. However, significantly more unplanned admissions and unplanned surgical curettage occurred after expectant management and medical management than after surgical management. The cumulative success rate for women managed expectantly was 87.6%, 68% for those managed medically and 90.4% for those who underwent uterine evacuation [4,5].
Preliminary reports on future fertility rates among women following expectant management of miscarriage were reassuring in relation to future pregnancy rate, miscarriage rate and the incidence of ectopic pregnancy. The cumulative conception rates in women managed expectantly but who later required surgical evacuation were 93%, those managed expectantly 91% and those managed primarily by evacuation 88% [21].
Availability of Transvaginal sonography and services for emergency evacuation and blood transfusion should be ensured before expectant management [4,5]. Further, expectant method is proved to be more cost effective than surgical method especially in a developing country like India was resources are less [22]. The cost and complications of surgical uterine evacuation can be avoided by proper selection of patients for expectant management after proper counseling.
Different studies were conducted to increase the Success rate with lesser complications in expectant management of miscarriages. The use of Colour Doppler imaging of the intervillous space and the uterine artery blood flow has been used to predict the outcome of expectant management of early pregnancy miscarriages. Newer studies on patient selection for expectant management based on serum beta HCG, serum progesterone, serum inhibin A and cervical nitric oxide is under evaluation [7,12,23]. Proper selection and counseling of patients fit for expectant management and increasing the duration of expectant period under observation; can improve the outcome of expectant management. Further studies about biochemical and sonological markers may ensure a higher Success rate with much lesser complications in expectant management of pregnancy miscarriages.
Limitations
There were few limitations to our study like: Patient preference causing difficulty to assign patients. Matching could not be done with the type of miscarriage in each method. Follow up, unplanned admission and availability of blood products at times was difficult. USG was mandatory. Cost effectiveness and pelvic infection could not be assessed.
Conclusion
The expectant management miscarriage has an acceptable success rate with complications comparable with surgical group except for the unplanned admissions and emergency evacuation. Even though the evidence is insufficient to demonstrate the superiority of either expectant or surgical management. Success rate of expectant management can be improved with much lesser complication by proper patient selection and counseling. Routine surgical evacuation may not be a justifiable option in all early pregnancy miscarriages due to lack of scientific support and patient preferences has a large role in management of pregnancy miscarriages. With accumulating positive evidence and newer advance in patient selection; expectant management could be offered as a better, natural, noninvasive management. More studies of expectant management of early pregnancy miscarriages are required in our setup overcoming the limitations mentioned, as it could be a cost effective choice especially in developing country like India.