Carpal boss is defined as an osseous formation at the dorsal portion of the quadrangular joint of the wrist, which involves the second and third metacarpal bone, the capitate and trapezoid. It is mostly asymptomatic and an incidental finding on X-ray imaging. Nevertheless, a minority of patients suffers from symptomatic carpal bossing, including pain, restricted mobility and concomitant joint instability. Possible complications comprise tendon rupture, inflammatory and degenerative joint disease. The entity was first described by Fiolle in 1931 [1], but to date there is still few scientific data available in regard of diagnosis and effective treatment of patients with symptomatic carpal boss. We therefore pooled our experiences from three institutions with orthopaedic and radiological maintenance to bring together and share our investigations.
Materials and Methods
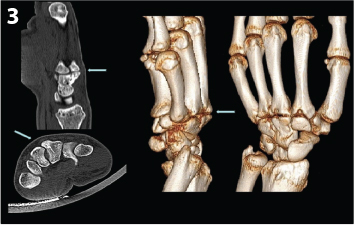
We are reporting our multicenter experience with this entity in a retrospective observation from 2010 to 2015 [Table/Fig-1]. Eight patients, mean age 35.6 years (29-42 years), were diagnosed with symptomatic carpal bossing. Three had a direct trauma to the dorsal wrist; five are competitive racket sport players, including tennis (3), golf (1) and badminton (1). Symptoms were pain at palmar flexion and limited mobility of the wrist in combination with a palpable protuberance over the quadrangular joint. All patients underwent X-ray examinations with anterio posterior and lateral projections. A bony protuberance was seen in all patients [Table/Fig-2]. In order to have thorough understanding of the anatomical line up of bones and bony changes, CT was conducted with a slice thickness of 1 mm with additional coronal, sagittal and 3D reconstructions. No accessory bones were detected and no degenerative changes of the quadrangular joint were seen, like joint space narrowing or subchondral sclerosis [Table/Fig-3].
Patient characteristics. CRPS = complex regional pain syndrome
| Patient | Sex | Cause | Treatment | Outcome (2-year follow-up) |
|---|
| 1 | female | traumatic | non-surgical | free of symptoms |
| 2 | female | traumatic | initially non-surgical, secondary surgical | CRPS |
| 3 | male | traumatic | initially non-surgical, secondary surgical | free of symptoms |
| 4 | female | non-traumatic | non-surgical | free of symptoms |
| 5 | male | non-traumatic | non-surgical | free of symptoms |
| 6 | male | non-traumatic | non-surgical | free of symptoms |
| 7 | male | non-traumatic | initially non-surgical, secondary surgical | free of symptoms |
| 8 | male | non-traumatic | non-surgical | free of symptoms |
Carpal boss on X-Ray imaging, lateral projection,

Carpal boss on CT imaging, multiplanar and 3D reconstructions
Imaging diagnostics were completed by MRI of all wrists with T1-, T2-, STIR, PDW-SPIR- and PDW-SPIR-contrast enhanced sequences. Bone edema surrounding the carpal boss was seen in four patients, including all posttraumatic patients. In addition to this, three patients had moderate signs of bursitis. The extensor tendons were not conspicuous of attrition or rupture. No fractures were seen and there were no indications of a benign or malignant tumour disease [Table/Fig-4].
Carpal boss on MRI imaging, sagittal STIR-sequence

A conservative treatment strategy was initiated for 6 weeks in all patients, including immobilisation, non-steroidal anti-inflammatory drugs on a daily basis for 3-4 weeks and extracorporal shock wave therapy on a weekly basis for 6 weeks. After this schedule, five patients were asymptomatic for the whole follow up period of 2 years. Three patients had persisting pain and were thus recommended for surgery. Wedge resection was performed to the depth of normal cartilage. In the postoperative course, two patients were asymptomatic for 2 years. One patient developed a type 1 complex regional pain syndrome (CRPS) in the first postoperative year, which was treated with pain-adapted physiotherapy, pharmacotherapy with analgesics and calcitonin, and a triple CT-guided thoracic sympathetic nerve blockade [2]. The patient showed a complete remission of symptoms after 10 weeks of therapy.
Discussion
Diagnosis
The prevalence of carpal boss is high, reported with up to 19% in cadaver studies [3]. Nevertheless most of the carpal bosses do not cause any symptoms. The entity may be seen on imaging as an auxiliary finding. Only approximately 1% of the affected people report of symptoms, mostly pain at the dorsal wrist, especially while performing repetitive or strong mechanical work. Referring to this, more than 60% of our patients are competitive racket sport players. Discomforting tendon snapping can be seen in some patients, usually from the extensor tendon of the index finger, leading to attrition, tendinitis, tenosynovitis or rupture [4]. Furthermore reactive bursitis may occur. We did not note these aspects in our patients.
The dominant hand is more likely to be affected, amplifying the assumption, that mechanical stress plays an aetiological role. There is no general gender preference. It is mostly seen in young adults from 20 to 50 years. We are in this range with our study group. It can be bilateral in 10-20% of cases [5].
Concerning the aetiology, several possibilities were published to date. It can occur posttraumatic, like in nearly 40% of our patients. A persisting os styloideum can be another underlying cause. This accessory ossicle is located dorsal between capitate, trapezium and the bases of the second and third metacarpals. Usually it fuses with the latter; however it can show a partial or missing coalition and can get symptomatic. An accessory capitate between capitate and hamate has also been reported [6]. With multimodal imaging, we did not detect any accessory bones at the quadrangular joints in our patients.
Degenerative aetiology has been assumed, but remains controversial, since reports about joint space narrowing and subchondral sclerosis are rare in the specific literature. Finally carpal boss can be a congenital partial osseous coalition. The physiological dorsal ligaments are missing in these cases [4].
Clinically it is best seen in wrist flexion and ulnar deviation. Diagnostic imaging should be conducted multimodal, if available. Useful imaging modalities consist of ultrasound, X-ray, CT and MRI, also in combination with PET or SPECT. X-ray as the initial modality is best conducted using the “carpal boss view”, a lateral projection of the wrist with flexion and supination of 30-40° and ulnar deviation of 20-30°.
The most frequent differential diagnosis is a ganglion cyst, which is often located in the tendons at the carpometacarpal joints. On clinical examination, it is softer than carpal boss and movable. Unfortunately it can also be caused by a carpal boss and mask this underlying condition. Other less frequent conditions are fibrosis, subcutaneous calcifications, intraosseous ganglion cysts, benign tumours (aneurysmal bone cysts, giant cell tumours from synovial tissue, lipoma, neuroma, neurofibroma, enchondroma, osteochondroma, osteoid osteoma) or malignant tumours (osteosarcoma, metastases) [7].
Treatment
Conservative therapy is recommended as the initial treatment, composed of immobilisation in a bandage or splint for 4-6 weeks and oral nonsteroidal anti-inflammatory drugs as and when required. If an accompanying inflammatory condition subsists (tenosynovitis, periostitis, peritendinitis calcarea), corticosteroid injections can be added, however the effect seems to be low [4]. We added extracorporal shock wave therapy to this protocol since we have good experience concerning pain relief and outcome. When the symptoms remain unchanged after this period of time or do not decrease significantly, surgery has to be discussed with the patient.
Wedge resection is the most commonly preferred option and has been performed in our three surgical patients. It is usually conducted with transversal incision at the metacarpal basis and a resection depth as far as undamaged cartilage tissue is seen at all sights of the quadrangular joint. If a persisting os styloideum is involved it must be resected completely, both if symptomatic itself or if it is the underlying cause of a carpal boss. This method’s success is disputed in the respective literature, ranging from excellent results [8], to persisting and recurring symptoms, potentially due to bony rebuilding and joint instability caused by the transection of dorsal ligaments and a change in angle between capitate and third metacarpal [9,10].
In the event of insufficient surgical outcome, repetitive wedge resection is one option, arthrodesis is another option. Unfortunately this procedure is not standardized. Loréa et al., described a technique for the second carpometacarpal joint, consisting of boss resection, wedge-shaped joint resection, followed by the insertion of a radial bone graft into the defect between the third metacarpal bone and the capitate to preserve the preexisting length [11]. Results were excellent, so the authors recommend the technique as the treatment of choice. Both wedge resection and arthrodesis require postoperative splinting for 3 weeks and physical therapy.
Limitation
The limitation of this study is the small sample size, taking into consideration that it is a rare entity and we already assembled three institutions.
Conclusion
In summary, carpal bossing is a mostly asymptomatic entity, which in our experience may become symptomatic due to direct trauma or repetitive stress, especially in competitive racket sports players. It can be diagnosed by thorough clinical examination and multimodal diagnostic imaging. Conservative treatment comprises an excellent prognosis, however surgery, either wedge resection or arthrodesis, must be considered if the response is not positive after 6 weeks.