Cerebral palsy (CP), a group of disorder of movement & posture, is considered as the leading cause of physical disability among children [1]. The resultant neurological impairments cause various activity limitations and frequently limit walking ability, which is an essential activity for daily living and social participation (International Classification of Functioning, Disability and Health (ICF) [2]. According to Gilles Caty et al., various outcome measures are available to assess locomotion ability in activity domain of ICF [2] among children with CP. E.g., Gross Motor Function Measure (GMFM), Gross Motor Functional Classification System (GMFCS), Paediatric Evaluation of Disability Inventory (PEDI), Activities Scale for Kids (ASK), Functional Independence Measure for Children (Wee FIM), Functional Mobility Scale (FMS), Gillette Functional Assessment Questionnaire (FAQ). These scales are validated and reliable scales widely used in assessment of children with CP but unfortunately have some limitations in measurement of walking ability [3].
The ABILOCO-Kids is a 10-item questionnaire described for use in children with CP to record a parent’s perceptions of their child’s usual walking performance. The scale has been calibrated in children with cerebral palsy aged 6-15 years & is available in French and English. The ABILOCO-Kids was developed from a bank of 41 questions, which were tested separately on 113 children with CP and their parents. Their responses were analysed using Rasch modeling to select items that fitted a uni-dimensional model & had an ordered rating scale. The final scale included 10 items that were invariant across age and sex & that represented a wide range of abilities. Testing by the developers of the ABILOCO-Kids with 113 children with CP and 108 parents has shown good psychometric properties with high test-retest reliability (ICC, 0.96; p<0.01) & high reproducibility of item hierarchy (ICC, 0.97). The ABILOCO-Kids also had high concurrent validity tested by correlation with the GMFCS (Spearman r = -0.88) [3].
Catty G et al., has also developed the ABILOCO questionnaire to assess locomotion ability in stroke patients & has tested the psychometric properties of the same scale [4].
A measure is valid when it fully & accurately captures the attribute that it is intended to measure. Face validity is most basic type of validity which simply examines whether an instrument appears to be measuring what it is meant to measure [5]. Content validity examines the extent to which the attribute of interest is comprehensively sampled by items or questions in instrument [5]. Concurrent validity describes how well questionnaire correlates with an existing gold standard measure [6].
Current project taken is part of a larger study to be done on various mobility issues of children with cerebral palsy which is being conducted at Ahmedabad city of Gujarat state of India. Hence, the aim of the present study was to validate Gujarati version of ABILOCO Kids questionnaire.
Materials and Methods
Present study is a cross-sectional observational (methodological) study conducted at paediatric rehabilitation unit of SBB College of Physiotherapy, Ahmedabad, Gujarat, India between 2013 – 2014.
Participants for face and content validity are (n=8) experts having mean experience of 24.62 years in field of paediatric, paediatric orthopedics, paediatric neurology and paediatric physiotherapy.
For concurrent validity children with CP of all GMFCS level & all clinical types aged 6 to 15 year were included. Children were excluded if their primary caregiver was either illiterate or do not know Gujarati. Concurrent validity was tested on 55 children with CP, mean age 8.56 year (range 6-15 year) by correlating the score of ABILOCO-Kids of their parents with GMFM 88 & GMFCS tested by therapist.
The study was approved by Institutional Ethics Committee SBB college of physiotherapy, with proposal no. PTC/IEC/93/2012-13.
ABILOCO-Kids questionnaire (41-item questionnaire) was translated into Gujarati from English using forward-backward-forward method. The translated version was approved by head of department of Gujarati Bhavan of Gujarat Vidhyapith.
Face & content validity - Nature & purpose of the study was explained to the professionals & informed written consent was obtained from all professionals along with self- filled personal and professional information. To ensure face & content validity of Gujarati version using group consensus method each item was examined by group of experts (n =8) with mean experience of 24.62 years in the field of paediatric, paediatric neurology, paediatric orthopedics and paediatric physiotherapy. Consensus is defined as agreement with a question by at least 80% of participant. Characteristic of Group Consensus method is selection of expert participants [7]. Each professional was contacted personally by primary author separately for their expert opinion in first step of validation. Each item was analysed by professionals for content, meaning, wording, format, ease of administration and scoring. Each item was scored as either accepted, rejected or accepted with modification. Coded responses were then given to secondary author for analysis. Procedure was continued until 80% of consensus for all items [Table/Fig-1].
List of items accepted with >80% consensus in phase 1
| Item no.of Englishversion | Description of activity |
|---|
| 6 | Kicking a ball with the paretic foot |
| 8 | Going up stairs putting both feet on each step |
| 10 | Running correctly even if you have to turn |
| 13 | Walking with the help of a person who guides but doesn’t support |
| 17 | Hopping on the healthy foot |
| 19 | Turning and walking in a narrow place |
| 20 | Walking less than 5 meters, indoors, holding onto pieces of furniture |
| 24 | Waling less than 5 meters alone without the help of a person |
| 25 | Going up and down stairs without holding onto the banisters |
| 27 | Kicking a ball with the healthy foot |
| 28 | Skipping rope |
| 30 | Hopping on the affected foot |
| 31 | Striding over an object with the paretic foot first |
| 33 | Walking with the help of 2 persons who support |
| 37 | Going up and down stairs with the help of a handrail |
| 41 | Walking while holding an object |
Total 22 items were modified as per suggestions given by experts with no change in meaning of original English item. None of items were rejected. No change made in sequence of item presentation. Only 3 items required rigorous discussion among group members regarding its applicability in children with cerebral palsy with reference to Indian context [Table/Fig-2].
List of items went for phase 2 of validation
| Item no.of Englishversion | Description of activity |
|---|
| 4 | Taking the train or the underground railway |
| 9 | Stepping up a kerb alone |
| 21 | Ice-skating, skate boarding, roller skating |
Concurrent validity – After explanation of nature & purpose of the study, an informed written consent was obtained from parents or legal caregiver of children with cerebral palsy & an oral consent was obtained from child who was able to understand and speak. Gujarati ABILOCO-Kids questionnaire was given to the primary caregiver of the child to be filled by themselves at home & if they have any query regarding some activity they were informed to bring it back to the primary researcher for clarity. Children were examined for GMFM 88 by other therapists who were unaware of the goal of the study. Concurrent validity of Gujarati version of ABILOCO-Kids questionnaire was assessed by comparing raw score of ABILOCO-Kids questionnaire with GMFM 88 and GMFCS.
Total 61 children with CP of all GMFCS level & all clinical types aged 6 to 15 year were screened. Two children were excluded as primary caregiver did not know Gujarati & 4 were excluded as primary caregiver was illiterate. Total N= 55 children with CP, mean age 8.56 year (range 6-15 year) were correlated for score of ABILOCO-Kids of primary caregiver with GMFM 88 & GMFCS.
Statistical Analysis
Raw scores of ABILOCO-Kids questionnaire score of GMFM 88 and GMFCS levels were analysed with use of SPSS version 16 with level of significance kept at 5%. Pearson’s & spearman’s correlation coefficients were used to assess the strength of association between the measures.
Result
[Table/Fig-3] represents the demographic details of study participants, which shows that majority of children with CP belonged to spastic diplegic and hemiplegic type. Considering the ambulation potential almost 66% was able to ambulate independently or with assistive device while rest belongs to GMFCS level IV- V & were non ambulatory.
Demographic details of study participants
| Clinical types of CP | Number (%) |
|---|
| Spastic type -Diplegic | 21 (38%) |
| Hemiplegic | 10 (18%) |
| Quadriplegic | 7 (13%) |
| Triplegic | 4 (7%) |
| Dystonic | 9 (17%) |
| Ataxic | 4 (7%) |
| GMFCS level- |
| Ambulatory –I,II,III | 36 (66%) |
| Non ambulatory – IV,V | 19 (34%) |
Face & content validity: Data were obtained from mothers of children with CP because they were mostly the primary caregiver of children in studied population except 3 children where father or grandfather was primary caregiver.
In phase 2 of validation process of Gujarati version of ABILOCO-Kids questionnaire rigorous discussion was done about translation and application of certain items in questionnaire. Item no 2 (walking between parallel bars) was translated into Gujarati with the word “parallel bar” kept as it is because the Gujarati translation of “parallel bar” was not meaningful. Item no 4 (taking the train or the underground railway) was having more global ability expectation as per CP population. It includes activities like taking a ticket, crossing a platform, climbing up in Indian rail, reaching destination etc. In item no 9 (Stepping up a kerb alone), the Gujarati translated meaning of word “kerb” was questionable among the group & hence required further clarification. For Item no 21 (Ice skating, skate boarding, roller skating), only roller skating could be possible as per location of Gujarat. The group had strong discussion on whether to keep ice skating & skate boarding in the item or not. Finally the group agreed to keep ice skating & skate boarding as the Gujarati translated version could be applicable across the globe where any kind of skating may be possible. So, the order of statement was changed within the same item without changing the actual sequence of item. It was kept as “skating – e.g., roller skating, skate boarding, ice skating).
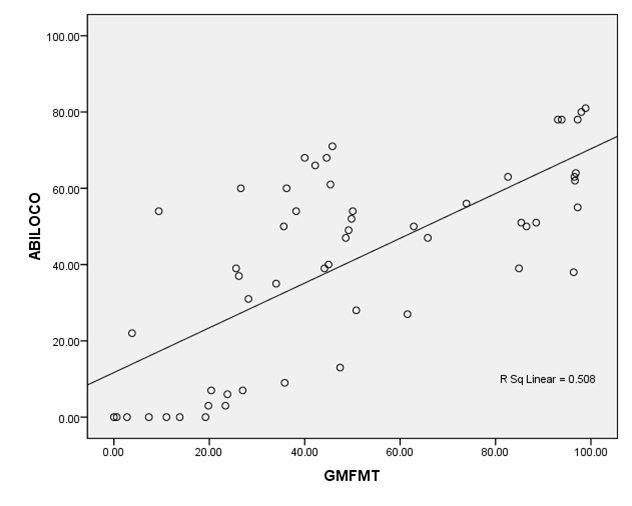
Concurrent validity: For correlation of ABILOCO-Kids raw score with total score of GMFM 88. Pearson’s correlation test was used which shows highly significant strong positive correlation with r=0.713, p<0.001 [Table/Fig-4]. For correlation of ABILOCO-Kids raw score with GMFCS, Spearman’s correlation test was used which shows highly significant strong negative correlation with r= -0.778, p<0.001 [Table/Fig-5].
Correlation of ABILOCO-Kids raw score with GMFM total
Correlation of ABILOCO-Kids raw score with GMFCS level
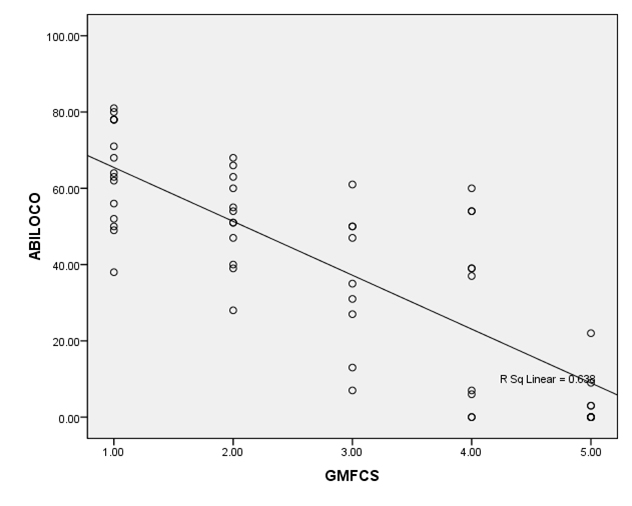
For concurrent validity raw score of 41 item ABILOCO-Kids questionnaire was correlated with GMFM 88 & GMFCS levels on 55 children with CP mean age 8.56 year (range 6-15 year), male 35 (63.63%), female 20 (36.36%). Median of GMFCS was 3.0. Mean GMFM total was 49.61±3.13 & mean ABILOCO-Kids total raw score was 40.80 ± 2.57. Pearson’s & spearman’s correlation coefficients were used to assess the strength of association between the measures. For correlation of ABILOCO-Kids raw score with total score of GMFM 88, Pearson’s correlation test was used which shows highly significant strong positive correlation with r=0.713, p<0.001 which is shown in [Table/Fig-2]. For correlation of ABILOCO-Kids raw score with GMFCS, Spearman’s correlation test was used which shows highly significant strong negative correlation with r= -0.778, p<0.001 which is shown in [Table/Fig-4].
Discussion
Caty D Gilles et al., the founder of ABILOCO-Kids questionnaire, studied both parent’s and children’s responses on their locomotion ability and concluded that locomotion ability can be discriminated with a 27 times greater resolution than when using the parents’ perception rather than the children’s [3]. Hence, direct parent’s perception was measured in current study. The reason why preliminary questionnaire was chosen for Gujarati translation was that, it specifically explores locomotion and includes a large number of locomotion activities that a healthy child realizes during his daily life activity and social participation compared to Rasch-built 10-item ABILOCO-Kids questionnaire which has very limited activities. In the same study, when children’s ABILOCO-Kids scores were used, author found that children’s perception was not correlated with GMFCS levels (p= -0.393, p= 0.142) which further supports the selection of parent’s perception [3].
Result of present study is consistent with Caty D Gilles et al., [3]. However, almost 65.45% of studied population belongs to ambulatory category of GMCS level (level I, II, III) indicating a ceiling effect. Chong J et al., studied 60 children with CPof age between 6-18 years with GMFCS levels I to III & found that ABILOCO-Kids questionnaire, 1 MWT & 6 MWT are all inversely correlated with GMFCS level [8].
[Table/Fig-3] shows that spastic diplegics and hemiplegics were 38.18% and 18.18% respectively among the total participants which is relatively less severe locomotion difficulties compared to other clinical types of CP which are less in number.
In study done by Caty Gilles et al., raw scores were converted into logit scores & they found that locomotion ability of quadriplegic children is distributed from -5.71 to ±3.04 logits (mean: -3.54 ± 2.84), of the diplegic children from -4.72 to ±4.31 logits (mean:0.48 ±3.13), and of the hemiplegic children from -5.71 to ±5.22 logits (mean:2.69 ±2.35). Thus, on average, the hemiplegic children have greater locomotion ability than the diplegic children, and diplegic children have greater locomotion ability than the quadriplegic children [3].
However, in the present study analysis was based on total raw scores of ABILOCO-Kids questionnaire & not the logit scores which is the limitation of present study. The authors of ABILOCO-Kids questionnaire recommends the raw score to be converted into linear measures which is expressed in logits using online analysis on website (www.rehab-scales.org). Substantial agreement was found by senior physiotherapists between parental report of their child’s ambulatory function & direct observation of the child’s walking around the home and school [9]. Few advantages of parental reports includes: ease of administration in clinical practice, less time consuming for therapists as it can be filled up by parents by the time therapist finishes clinical testing, cost effective. Using parent’s perception enables locomotion ability to be assessed in all patients with CP including very young children and those with mental or communicative disorders. At the same time, a written self-administered report given by the parents of caregivers is considered more appropriate for a routine clinical use than a face-to-face interview, which may be influenced by personality and the style of the interviewer & his/her relationship with the subject [10].
Conclusion
Group consensus method proves face and content validity & highly significant positive correlation with GMFM and highly significant negative correlation with GMFCS proves concurrent validity of Gujarati version of ABILOCO-Kids questionnaire. Gujarati version of ABILOCO-Kids questionnaire can be useful parent report measure of locomotor ability in a clinical set up. Future studies are required to find reliability of the same & then it can be put into clinical practice.