Successful Retrieval of Uncoiled Coronary Guidewire Using Simple Balloon Method
Shivanand Patil1, Rangraj Ramalingam2, Jayashree Kharge3, Mohan Nayak4, Cholenahally Nanjappa Manjunath5
1 Associate Professor, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences & Research, Bangalore, India.
2 Professor, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences & Research, Bangalore, India.
3 Associate Professor, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences & Research, Bangalore, India.
4 Chief Technician, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences & Research, Bangalore, India.
5 Director, Professor and Head, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences & Research, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shivanand Patil, Associate Professor, Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences & Research, Jayanagar 9th Block, Bannerghatta Road, Bangalore-560069, Karnataka, India. E-mail : drssspatil@rediffmail.com
Breakage of angioplasty device in coronary artery can cause panic in the catheterization laboratory. These broken fragments may serve as a nidus for thrombus formation; hence, removal of these fragments becomes mandatory. Since the incidence of guidewire fracture during angioplasty are rarely reported, evidence-based approaches are not available for the management of such incidental conditions. Here, we report an interesting case of entrapment and unravelling of guidewire. We successfully retrieved unravelled guidewire using a noncompliant balloon inflated in the guiding catheter. Subsequently, the procedure was completed successfully with an implantation of a stent in the culprit lesion. We are of opinion that this novel technique is quite easy and less cumbersome than other described techniques reported earlier.
Complications, Interventional cardiology, New techniques
Case Report
A 70-year-old hypertensive male patient presented to our institute with a history of inferior-wall myocardial infarction one month prior to the presentation. Despite the initial treatment for infarction received elsewhere, he was persistently experiencing effort angina of NYHA class III. Angiography was performed through femoral access, which revealed an insignificant lesion in proximal right coronary artery along with 80–90% stenosis in the left circumflex artery at the origin of left posterior descending artery. Patient was taken for angioplasty in the same sitting.
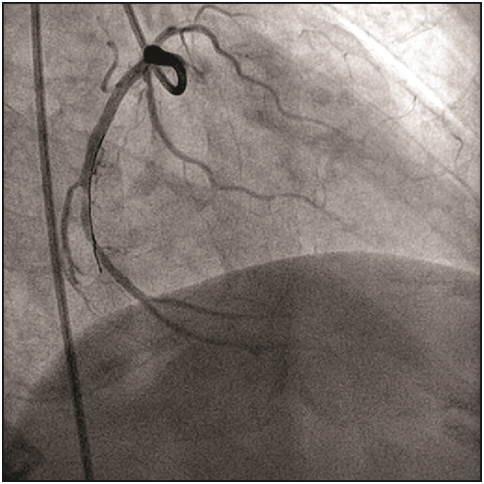
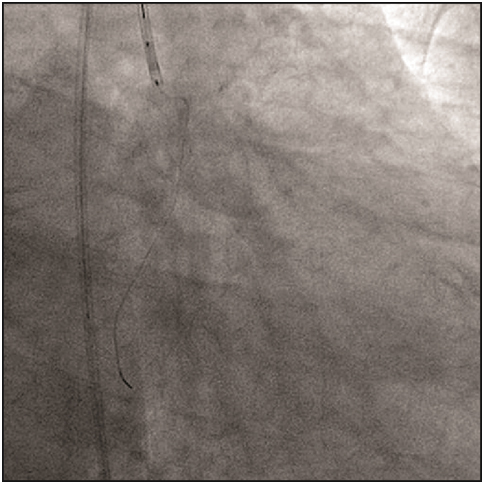
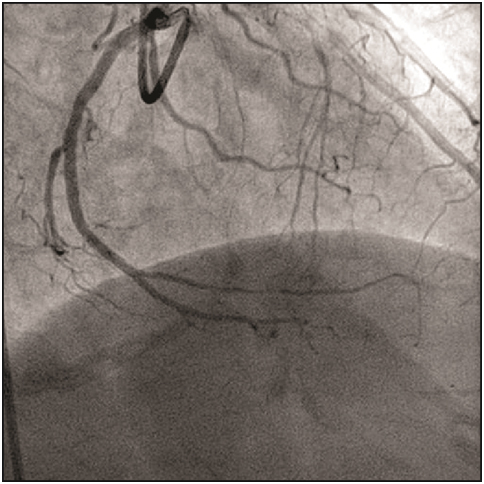
A 7F Judkins guiding catheter (Cordis Corp., Florida, USA) was used to cannulate the left coronary artery, and the lesion was crossed by using 0.014”Floppy guidewire (Abbott Vascular Inc., California, USA). We experienced that the movement of the wire tip became restricted after it crossed, the lesion. Angiograms in different views showed that the distal tip of wire was trapped in a small branch of the left circumflex coronary artery [Table/Fig-1], which had gone into spasm. Immediately, nitroglycerin, sodium nitroprusside, and nicorandil were given to relieve the spasm. Repeated attempts were made to gently pull the wire, but the guiding catheter was getting sucked in to the left circumflex coronary artery and also the guidewire did not move at all. Later, the spring over the wire got uncoiled [Table/Fig-2] and the radio-opaque tip got fragmented upon increasing the pressure over the wire. The two portions were being held together by the fine uncoiled spring coating. At that point, we passed a noncompliant Sprinter balloon (Medtronic Inc., Minnesota, USA) of 1.5 X 10 mm size to the distal tip of the wire and tried to pull the wire gently, but this caused further uncoiling of the wire and the wire could not be retrieved. To tide over the crisis, we used a simple indigenous way of retrieval using a bare noncompliant balloon of 2.5X 9 mm size, which was passed up to the tip of guiding catheter [Table/Fig-3]. The balloon was inflated at 10 atm pressure inside the tip of guiding catheter, which led to successful entrapment of the guidewire between outer surface of the balloon and inner wall of the guiding catheter. Once the wire was secured properly, whole assembly was removed en masse through the vascular system [Table/Fig-4,5 and 6].
Guidewire entrapped in a small branch of the left circumflex coronary artery
A 2.5 X 9 mm noncompliant balloon inflated inside the catheter
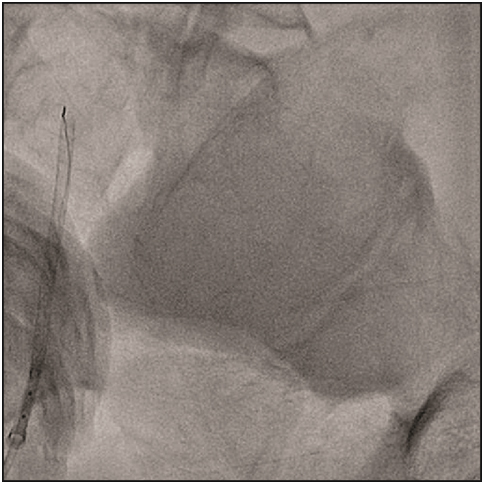
Whole assembly in the descending aorta after its removal from coronary artery
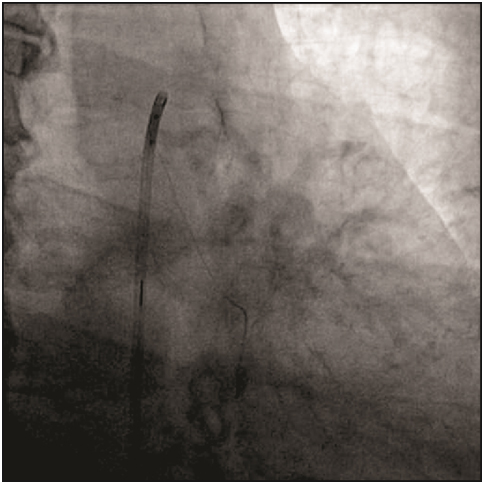
Whole assembly being removed en masse through the femoral sheath
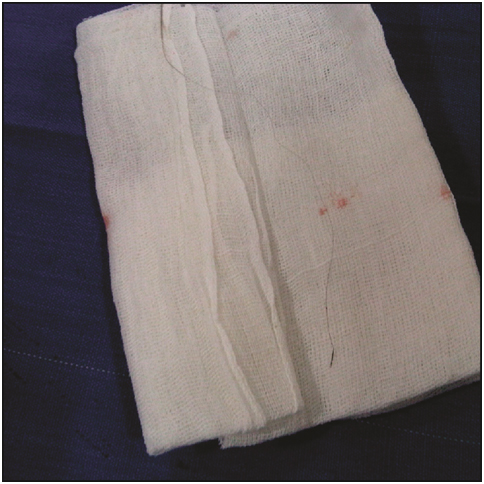
Retrieved guidewire after its removal from the vascular system
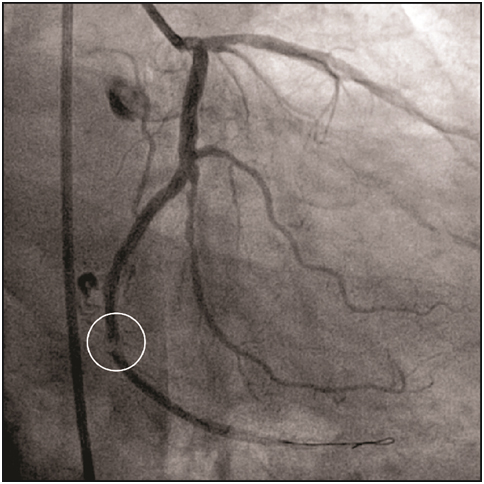
After ensuring that no fragments were left in the coronary artery [Table/Fig-7], procedure was continued. Lesion was crossed with another 0.014” Floppy wire (Abbott Vascular Inc., California, USA). Lesion was predilated with 2.5 X 10 mm sprinter balloon. Subsequently, a drug-eluting stent of 2.75 X 19 mm size was deployed at 12 atm. As the stent was not fully expanded, post-dilation was performed using a noncompliant Sprinter balloon (Medtronic Inc., Minnesota, USA) of size 3X9 mm at 16 atm. Immediately after post-dilation, the patient complained of chest discomfort. Check shoot revealed thrombus just at the distal end of the stent [Table/Fig-8]. The activated clotting time, measured at that time, was 170 seconds. Instantly, a bolus of intracoronary glycoprotein IIb/IIIa inhibitor, additional heparin, nitroglycerin, sodium nitroprusside and nicorandil was given. This led to complete dissolution of thrombus and the patient was relieved of symptoms. Post-procedural angiogram showed good coronary flow [Table/Fig-9]. The patient was discharged two days after the procedure, and the hospital stay remained uneventful. At 6-month follow-up, the patient remained asymptomatic.
Check angio ensured that no fragments were left in the vascular system; displaying 80% stenosis in the left circumflex artery
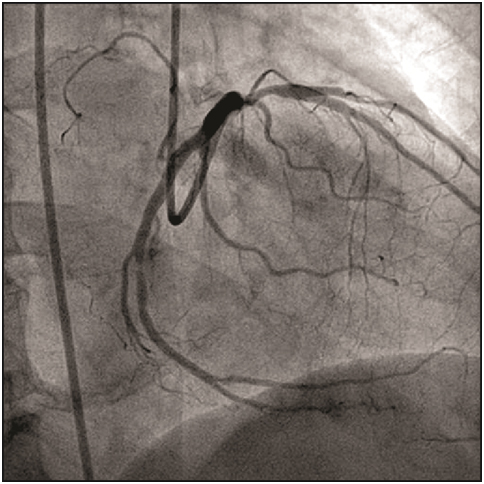
Thrombus seen at the distal end of the deployed stent
Discussion
Percutaneous coronary intervention is a commonly performed procedure these days. Although advances in percutaneous coronary intervention have dramatically improved the outcomes in patients with coronary artery disease, it is not complication-free [1]. Hardware breakage, entrapment, fracture, and dislodgement of angioplasty devices in coronary arteries are such infrequent, but serious procedure-related complications, with reported incidences of approximately 0.2–0.8% of cases [2–4]. Guidewire fractures inside the intravascular compartment are reported in 0.1–0.2% of cases undergoing coronary intervention. The reported causes of guidewire unravelling are entrapment of the wire in a small branch, vessel tortuosity, and over-rotation of the wire [4]. Here, we present a case report of unravelling coronary guidewire inside the coronary artery, which was successfully retrieved using a balloon catheter. In our case, the possible mechanism of complication would have been that the guidewire got caught in a small branch leading to spasm of vessel and subsequent attempts to release the wire led to unravelling.
It is widely established that remnants of fractured guidewire are associated with life-threatening conditions such as intracoronary thrombus formation, embolization, and perforation [2–4]. Hence, every possible attempt should be made to retrieve them from the coronary circulation [1]. Nevertheless, no evidence-based approach is available for the optimal management of fractured guidewire during coronary intervention due to rarity of such events [4]. Further, retrieval of these fragments can be challenging since there is no single technique which will succeed in all situations. Hence, it is worthwhile to be acquainted with different retrieval techniques [5].
Available literature suggests the use of cardiothoracic surgery as the last resort, while it recommends the use of various percutaneous retrieval methods such as simple snare loop, paired guidewires knotted together, or homemade wire loop snares [6,7]. Since, there are theoretical concerns over thrombotic risks with various snare devices [6], we did not opt for them. On the contrary, we used a balloon catheter to retrieve the uncoiled coronary guidewire.
Earlier, Patel et al., demonstrated a retrieval of a broken angioplasty wire fragment from the coronary system using an additional angioplasty wire and a balloon catheter [8]. In other report, Surhonne et al., used a hybrid technique with a slip catheter for the successful retrieval of a fractured wire tip [9]. Kharge et al., displayed a successful retrieval of a broken stent-delivery system using a balloon on another guidewire [7]. On the contrary to these techniques, we propelled a 2.5 X 9 mm noncompliant bare balloon in the catheter and then inflated the balloon inside the proximal most part of the catheter. In our case, the balloon held the guidewire against the inner wall of the guiding catheter with enough pressure to enable us to pull the whole system through the femoral sheath en masse. This novel technique was quite easy and less cumbersome than other described techniques.
It is suggested that the activated clotting time during angioplasty in such patients should be kept at least 50 seconds higher than the usual activated clotting time, by giving extra dose of heparin, so as to prevent thrombus formation around the foreign body. Unfortunately in our case, slightly prolonged duration of procedure and an endothelial injury by wire led to thrombosis at the distal portion of the stent, which was managed appropriately. The patient was discharged in healthy state and was asymptomatic at follow up.
Conclusion
Although percutaneous coronary interventions are relatively safe, procedure-related complications, such as hardware breakage inside the intravascular compartment, presents a unique set of problems. In the present case, we successfully retrieved unravelled guidewire using a noncompliant balloon inflated in the guiding catheter. We believe that this novel technique is quite easy and less cumbersome than other described techniques reported earlier.
[1]. Bonvini RF, Werner KD, Buettner HJ, Buergelin KH, Zeller T, Retrieval of lost coronary guidewires during challenging percutaneous coronary interventionsCardiovasc Revasc Med 2010 11(4):262.e7-10. [Google Scholar]
[2]. Chang TM, Pellegrini D, Ostrovsky A, Marrangoni AG, Surgical management of entrapped percutaneous transluminal coronary angioplasty hardwareTex Heart Inst J 2002 29(4):329-32. [Google Scholar]
[3]. Kim TJ, Kim JK, Park BM, Song PS, Kim DK, Kim KH, Fatal subacute stent thrombosis induced by guidewire fracture with retained filaments in the coronary arteryKorean Circ J 2013 43(11):761-65. [Google Scholar]
[4]. Singh D, Darbari A, Retrieval of trapped and broken guidewire with immediate rescue off-pump coronary bypass surgeryInteract Cardiovasc Thorac Surg 2014 19(3):529-31. [Google Scholar]
[5]. Mehta V, Pandit BN, Trehan V, Retrieval of broken export catheter during primary angioplastyInt J Angiol 2013 22(3):185-88. [Google Scholar]
[6]. Balbi M, Bezante GP, Brunelli C, Rollando D, Guidewire fracture during percutaneous transluminal coronary angioplasty: possible causes and managementInteract Cardiovasc Thorac Surg 2010 10(6):992-94. [Google Scholar]
[7]. Kharge J, Sreekumar P, Swamy K, Bharatha A, Ramegowda RT, Nanjappa MC, Balloon-assisted retrieval of a broken stent-delivery systemTex Heart Inst J 2012 39(5):644-46. [Google Scholar]
[8]. Patel T, Shah S, Pandya R, Sanghvi K, Fonseca K, Broken guidewire fragment: a simplified retrieval techniqueCatheter Cardiovasc Interv 2000 51(4):483-86. [Google Scholar]
[9]. Surhonne PS, Mahla H, Bhairappa S, Somanna S, Manjunath CN, Successful retrieval of fractured pressure wire tip (FFR) by hybrid techniqueJ Saudi Heart Assoc 2015 27(2):118-22. [Google Scholar]