Plasmacytoid Myoepithelioma of the Hard Palate in a Child – A Rare Case Report
Padmaja Ramesh Kulkarni1, Anita Pandit Javalgi2, Bhaswanth Pottipati3, Fazil Shajahan4
1 Associate Professor, Department of Pathology, BLDEU Shri B M Patil Medical College, Hospital & Research Centre, Bijapur, India.
2 Assistant Professor, Department of Pathology, BLDEU Shri B M Patil Medical College, Hospital & Research Centre, Bijapur, India.
3 Post Graduate Student, Department of Pathology, BLDEU Shri B M Patil Medical College, Hospital & Research Centre, Bijapur, India.
4 Post Graduate Student, Department of Ear, Nose and Throat, BLDEU Shri B M Patil Medical College, Hospital & Research Centre, Bijapur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Padmaja Ramesh Kulkarni, Associate Professor, Department of Pathology, BLDEU Shri B M Patil Medical College, Hospital & Research Centre, Bijapur - 586103, India. E-mail : padmaja.kul21@gmail.com
Myoepithelioma is a rare tumour accounting for 1-1.5% of salivary gland tumours, 21% of which occur in soft & hard palate. Cytologic features of these tumours are not well established leading to diagnostic pitfall in many cases on FNAC. However, as radiologic findings are overlapping and inconclusive in salivary gland tumours, preoperative cytologic diagnosis may help surgeons to plan surgery especially in patients requiring facial surgery. Here, we present a rare case of plasmacytoid myoepithelioma of the hard palate in an 11-year-old boy which was conclusively diagnosed on FNAC and further confirmed by histopathological and immunohistochemical studies. We have made an attempt to describe cytologic features of myoepithelioma with differential diagnosis of these tumours through review of literature.
Cytologic diagnosis, Intra oral mass, Salivary gland tumour
Case Report
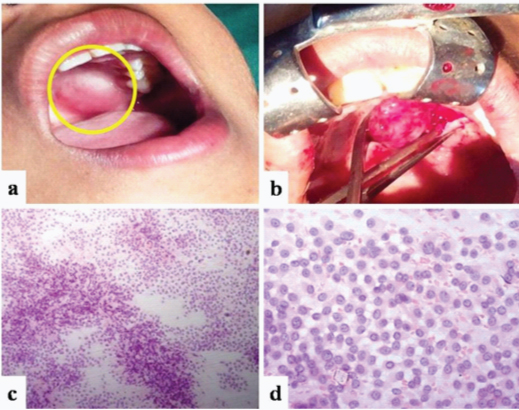
An 11-year-old boy with painless, slowly growing mass over hard palate since six months was referred to Pathology department for FNAC of the lesion. Examination revealed a well circumscribed, firm, nontender mass that measured about 1.5x1cm. Mucosa covering the mass was reddish and showed congested vessels [Table/Fig-1a&b]. FNA was performed using 23 G needle and 10 cc syringe. Multiple smears stained with H&E, PAP & Giemsa showed high cellularity consisting of plasmacytoid cells in sheets, clusters and singles. Individual tumour cells were round to polygonal with eccentrically placed round nuclei showing fine to vesicular chromatin and small nucleoli. Most of these cells had moderate to abundant eosinophilic cytoplasm. There was neither atypia nor mitosis noted in these cells. Background showed few myxoid stromal fragments with absence of necrosis [Table/Fig-1c&d]. Correlating the clinical and cytologic features, diagnosis of plasmacytoid myoepithelioma was given on FNAC and tumour was excised.
(a) Clinical photograph showing a mass on hard palate (b) Intraoperative photograph showing firm, well circumscribed mass (c) Fine Needle Aspiration smear showing high cellularity (H&E Stain, x100) (d) Microphotograph showing sheets of plasmacytoid cells with eccentric nucleus and prominent nucleoli (H&E Stain, x400)
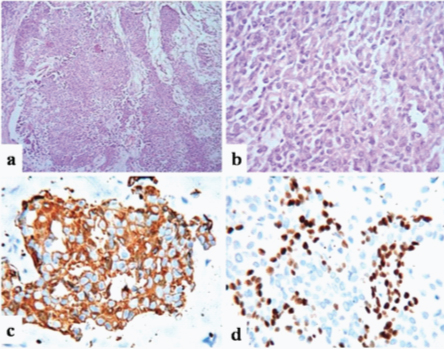
Gross examination of the mass revealed a partially encapsulated grey brown globular mass measuring about 1.5x1cm, and firm in consistency. Cut section was solid, lobular and grey white in colour. Histopathological examination revealed a solid tumour consisting of plasmacytoid cells in nests, islands and cords separated by scanty myxoid stroma. There were no ductal or glandular elements, as well as atypia or necrosis in the sections studied [Table/Fig-2a&b]. On immunohistochemical studies tumour cells were strongly positive for cytokeratin 14 and focally positive for cytokeratin 19, p63 and Smooth Muscle Actin (SMA) [Table/Fig-2c&d] confirming the diagnosis of myoepithelioma.
(a) Histological section showing tumour cells in nests, islands and cords separated by scanty myxoid stroma (H&E Stain, x100) (b) High power view showing plasmacytoid myoepithelial cells (H&E Stain, x400) (c) Microphotograph showing strong positivity for Cytokeratin 14 (IHC stain, x400) (d) Microphotograph showing focal positivity for p63 (IHC stain, x400)
Discussion
Myoepithelioma was first described by Sheldon in 1943. Most of the authors in the past had considered these tumours to represent an extreme spectrum of pleomorphic adenoma with predominance of myoepithelial differentiation. However, since 1991 WHO has classified myoepithelioma as distinct tumour as these tumours were relatively more aggressive than pleomorphic adenoma [1]. Myoepithelioma is a very rare tumour with less than 100 cases reported in the literature, of which only four cases have been reported in pediatric age group below 12 years of age [1,2]. Myoepithelioma accounts for 1-1.5% of salivary gland tumours, 21% of which occur in soft & hard palate. These tumours occur at any age group from first decade to eighth decade with peak incidence in third & fourth decade. They arise equally in men & women, though few studies have reported a slight male predominance. The most common location is parotid gland [3].
Myoepithelioma of the palate clinically presents as slow growing, painless, firm submucosal mass as it was seen in our case. The differential diagnoses of intraoral submucosal mass include inflammatory abscess, deep mucocele, and salivary gland tumours. Most of the salivary gland tumours have overlapping features on radiological investigations and hence FNAC & Biopsy are important in diagnosing these tumours preoperatively [4]. There are few studies highlighting the cytologic features of salivary gland tumours with varied specificity and sensitivity on FNAC; however the cytologic features of myoepithelial tumours are under described in the literature.
The cytological diagnosis offered for these tumours are inconclusive most of the time despite adequate cellular material. In many cases histopathological and immunohistochemical studies are required to arrive at a final diagnosis. However, preoperative cytologic diagnosis of the type of the tumour may help the surgeon to plan the best therapeutic approach [5]. These tumours are variably positive for S-100, SMA, Cytokeratin, p63, vimentin and Glial Fibrillary Acid Protien (GFAP) on immunohistochemistry [6].
Cytokeratin 14 is expressed in normal myoepithelial cells as well as terminally differentiated neoplastic myoepithelial cells. Plasmacytoid variant of myoepithelial cells are negative for SMA or may show only focal positivity [7]. In the present case tumour cells were positive for CK14, P63, and SMA.
Myoepithelioma should be differentiated from other salivary gland tumours, its malignant counterpart and other soft tissue tumours mimicking myoepithelioma. Cytologically four different types of myoepithelioma exist; spindle cell, plasmacytoid, clear and epithelioid cell types.
Spindle cell myoepithelioma should be differentiated mainly from benign and malignant spindle cell tumours like nerve sheath tumours, cellular leiomyoma, leiomyosarcoma, synovial sarcoma, haemangiopericytoma and solitary fibrous tumour. Careful observation of cellular density, arrangement and individual cell morphology may help in differentiating these tumours. Compared to other soft tissue tumours aspirate will be more cellular and shows epithelial like arrangement of cells with distinct cell margin and nondescriptive cytoplasm [8].
Plasmacytoid myoepithelioma needs to be differentiated from benign and malignant tumours like myoepithelial cell predominant pleomorphic adenoma, plasmacytoma, lymphoma, skeletal muscle and rabdoid tumours [9]. Absence or less than 5% of epithelial cells showing ductal or acinar formation and absence of chondroid stroma helps in differentiating from pleomorphic adenoma [1,9]. In our case scanty myxoid stromal fragments were noted and inconspicuous ductal or acinar pattern helped us to distinguish it from pleomorphic adenoma. Absence of cellular pleomorphism, increased mitotic count and necrosis helps to differentiate myoepitheliomas from myoepithelial carcinomas [10]. Previous studies have documented recurrence rate of 15 to18% for myoepithelioma. Treatment of choice is local excision with normal margins and long term follow up for recurrence [1,7]. In our case patient did well postoperatively and no recurrence noted till six months of follow up.
Conclusion
Myoepithelial tumours should be kept as one of the differential diagnosis when dealing with intraoral submucosal mass in pediatric age group. Myoepitheliomas are very often misinterpreted as malignant tumours due to high cellularity on aspirate. Pathologists should be aware of its cytological features as preoperative cytological diagnosis may help the surgeon to give best possible treatment to their patients.
[1]. Gore CR, Panicker NK, Chandanwale SS, Singh BK, Myoepithelioma of minor salivary glands - A diagnostic challenge: Report of three cases with varied histomorphologyJ Oral Maxillofac Pathol 2013 17:257-60. [Google Scholar]
[2]. Reddy H, Reddy SE, Reddy KE, Sudhir G, Plasmacytoid Myoepithelioma of the Palate: A Rare Case ReportJournal of Research and advancement in Dentistry 2013 2(1):52-54. [Google Scholar]
[3]. Zormpa MT, Sarigelou AS, Eleftheriou AN, Assimaki AS, Kolokotronis AE, Plasmacytoid Myoepithelioma of the Palate: Case ReportHead and Neck Pathology 2011 5(2):154-58. [Google Scholar]
[4]. Cruz Perez DE, Lopes MA, Almeida OP, Jorge J, Kowalski LP, Plasmacytoid myoepithelioma of the palate in a childInt J Paediatr Dent 2007 17:223-27. [Google Scholar]
[5]. Brennan PA, Davies B, Poller D, Mead Z, Bayne D, Puxeddu R, Fine needle aspiration cytology (FNAC) of salivary gland tumours: Repeat aspiration provides further information in cases with an unclear initial cytological diagnosisBr J Oral Maxillofac Surg 2009 10:1-4.doi:10.1016/j.bjoms.2008.12.014 [Google Scholar]
[6]. Gayathri BN, Kalyani R, Kumar HM, Azeem SM, Fine-needle aspiration findings in epithelioid myoepithelioma of the parotid gland: A diagnostic pitfallJ Oral Maxillofac Pathol 2014 18:131-13. [Google Scholar]
[7]. Rani P, Kaur R, Malhotra D, Dass PK, Sachdeva S, Kapoor R, Plasmacytoid Myoepithelioma of The Palate In An Adolescent – A Case Report And Review of LiteratureIndian Journal of Dental Sciences 2014 6(2):55-57. [Google Scholar]
[8]. Horibe Y, Murakami M, Korematsu M, Imaeda Y, Tashiro K, Tsukinoki K, Fine needle aspiration cytology of spindle cell myoepithelioma of the submandilar gland: A case reportOral Med Pathol 2000 5:65-68. [Google Scholar]
[9]. Kumar AY, Nadarajah J, Chandrashekhara SH, Tambade VD, Acharya S, Myoepithelioma of the Soft Palate: A Case ReportCase Reports in Otolaryngology. [Internet] 2013 [cited 2014 Sep 15]:1-4. Available from : http://dx.doi.org/10.1155/2013/642806 [Google Scholar]
[10]. Mukunyadzi P, Review of Fine-Needle Aspiration Cytology of Salivary Gland Neoplasms, With Emphasis on Differential DiagnosisAm J Clin Pathol 2014 118(1):S100-15. [Google Scholar]