The main objectives of any therapeutic intervention aimed at root coverage is to restore the tissue margin to the Cemento-enamel junction and to gain an attachment of the tissue to the root surface such that the gingival sulcus shows no bleeding on probing and a minimal probing depth [1]. A variety of surgical techniques have been developed throughout the years and many studies have been carried out to evaluate these techniques with regard to their predictability and amount of root coverage achieved. Different surgical techniques which are commonly used for this approach are coronally or laterally positioned pedicle grafts, rotational flaps, autogenous free gingival grafts, subepithelial connective tissue grafts and combination of these techniques by applying principles of guided tissue regeneration (GTR). Despite the introduction of all the above mentioned procedures, autografts remains the ‘gold standard’ of periodontal plastic surgery as it provides excellent predictability, improved long-term root coverage and superior esthetics over other treatment options [2,3]. But the procurement of autogenous graft significantly increases patient morbidity as there is additional donor site while also lengthening the duration of surgery. Considering these pitfalls, many patients have an aversion to periodontal plastic procedures.
According to the concept of the GTR, a critical factor for the outcome of the treatment procedure is that a space for tissue formation is established between the facial root surface and the membrane which prevented the formation of a long junctional epithelium, thus facilitating periodontal regeneration by allowing the cells from the periodontal ligament to colonize the root surface. The potential advantage of GTR to a gingival flap procedure is the possibility of having a different healing pattern and ideally achieving periodontal regeneration rather than connective tissue repair of the exposed root surfaces with no additional donor site [4]. Recently, an allograft of alternative origin derived from human amnion tissue, which is the innermost lining portion of the placental membrane has been advocated in the treatment of gingival recession [4]. Amniotic membrane is a composite membrane consisting of pluripotent cellular element embedded in a semipermeable, membranous and is an immunotolerant structure [5–7]. Also, there is existence of pluripotent stem cells possessing the ability of trans differentiation to other cellular elements of periodontium making it a suitable candidate for GTR. Excellent revascularization of the amniotic membrane is another favourable property of this natural structure [8,9]. It also contains growth factors that may aid in the formation of granulation tissue by stimulating fibroblast growth and neovascularization. Amnion has shown an ability to form an early physiologic “seal” with the host tissue precluding bacterial contamination and multiple studies support amnion’s ability to decrease the host immunologic response via mechanisms such as localized suppression of polymorphonuclear cell migration [4,9,10].
Materials and Methods
Twelve patients of mean age 33.75±6.89 having at least 2 bilateral Miller’s Class I or Class II gingival recession were recruited from the Department of Periodontology, Rajarajeswari Dental College and Hospital. All the participants were informed about the study and its potential benefits. Informed consent was obtained from the patient. The selected patients were randomly allocated to
Group I- 12 recession defects treated with amnion allografts along with coronally advanced flap.
Group II- 12 recession defects treated with chorion allografts along with coronally advanced flap.
Ethical approval was obtained from the institutional review board. Systemically healthy patients who presented with at least 2 bilateral buccal recession defects ≥3 mm, with adequate vestibular depth and width of keratinized gingiva were included in the study. Patients with history of medications, poor oral hygiene, smokers, alcoholics, orthodontic patients were excluded from the study. Tooth with recent history of surgery at the study site within 6 months, showing pulpal symptoms, severe abrasion or decay on the exposed root surfaces and buccal or interproximal restorations were also excluded from the study.
Clinical Measurements: All clinical parameters were recorded with a standard UNC-15 manual probe at baseline, 3 and 6 months postoperatively.
Gingival Recession (GR) - was measured from the cement-enamel junction (CEJ) to the free gingival margin at the middle of the buccal surface.
Relative attachment level (RAL) - was measured mid-buccally with the reference point located at the buccal cusp/incisal edge.
Width of the recession defect (WRD) - was measured across the buccal surface at the CEJ level.
Width of keratinized gingival (WKG) - was measured from the gingival margin to the mucogingival junction.
The percentage (%) of root coverage for Group I (amnion site) and Group II (chorion site) was calculated according to the following formula [8]:

Surgical Procedure
The involved site was randomly assigned either to the coronally advanced flap with Amnion membrane (AM) [Table/Fig-1a] or to the coronally advanced flap with Chorion membrane (CM) [Table/Fig-2a]. After achieving profound anaesthesia, on the facial aspect two oblique vertical releasing incisions (i.e. one mesial and one distal to the involved tooth) was made extending beyond the mucogingival junction and into the mucobuccal fold to a point where the flap could be positioned over the original defect without tension. Sulcular incisions were given on the involved tooth and a trapezoidal mucoperiosteal flap was elevated by blunt dissection up to the recession defect. In the area apical to the recession defect, partial thickness dissection was done.
(a) Preoperative recession defect (b) Amnion membrane (c) Amnion membrane placed (d) Flap coronally sutured (e)10 days postop (f) Immediate after suture removal (g) 10 days post op months post surgery (g-i) 1, 3 and 6 months

(a) Preoperative recession defect (b) Chorion membrane (c) Chorion membrane placed (d) Flap coronally sutured (e)10 days post op (f) Immediate after suture removal (g)10 days post op months post surgery (g-i) 1, 3 and 6 months

In the adjoining interdental papillae, de-epithelialization was done to provide a bleeding connective tissue bed for the future coronally advanced flap. The exposed root surface was thoroughly planed and 17% EDTA was used on the root surface for root conditioning with the help of cotton swab for 30 seconds and washed away with water spray. A template was made with sterilized tin foil outlining the recession defect and was used to measure the width of the membrane (AM or CM) required for the surgical procedure. The commercially available membrane (human amnion & chorion membrane tata memorial hospital tissue bank) was then trimmed to cover the entire recession defect area [Table/Fig-1b,c & 2b,c], the flap was then coronally positioned to completely cover the membrane and secured by interdental sutures using No. 4-0 bioabsorbable suture (VICRYLTM, Johnson and Johnson). The vertical incisions were then sutured with two direct interrupted sutures on either side [Table/Fig-1d%2d]. A tin foil of suitable size was placed on the buccal aspect and a non-eugenol periodontal dressing was placed for proper wound stabilization and patient comfort. Similar surgical protocol was adopted on opposite quadrant of the involved site and also for all the patients.
All the patients were prescribed Amoxicillin 500mg TID and Acelofenac 100 mg BID for 7 days and were also instructed to abstain from brushing at treated site. They were also prescribed chlorhexidine gluconate oral rinse to rinse twice daily for 2 weeks. Patients were recalled after 10 days for suture removal [Table/Fig-1e,f&2e,f] and measurements were recorded at 1 [Table/Fig-1g&2g], 3 [Table/Fig-1h&2h] and 6 [Table/Fig-1i&2i] months intervals.
Statistical Analysis
Descriptive and inferential statistical analysis has been carried out in the present study. Mann Whitney U-test has been used to find the significance between two groups for parameters on non-interval scale and Wilcoxon signed rank test has been used to find the significance within each group.
Results
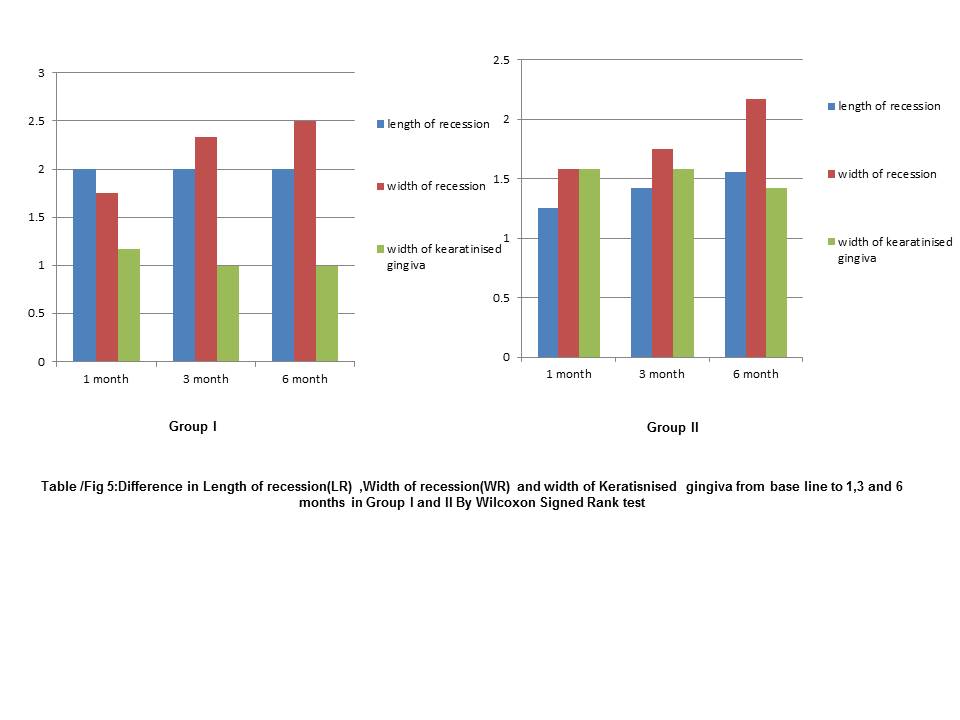
Twenty patients with gingival recession were assessed of which 12 patients with bilateral recession were recruited for the study. Twenty four recession defects of which 12 recession defects were treated with amnion allografts along with coronally advanced flap and 12 recession defects treated with amnion allografts along with coronally advanced flap. Comparison of two groups with respect to gingival index (GI) score at baseline, 1 month, 3 months and 6 months, the mean and standard deviations (SD) of GI in the group I were 2.75±0.66, 1.38±0.57, 1.04±0.50 and 1.13±0.48 respectively. In the group II these measurements were 2.88±0.80, 1.33±0.62, 0.88±0.38 and 0.79±0.33 respectively. There was reduction in GI in both the groups and statistically significant difference was seen between the amnion and chorion site seen at 1 month (p = 0.022). But no statistically significant difference was seen between both the groups at 3 months and 6 months. No adverse effects were observed after treatment. In group I from baseline to 1 month, 3 months and 6 months with respect to length of recession (p = 0.001,0002,0.002) width of recession(p=0.003,0.002,0.002) statistically significant reduction was observed and significant gain was seen with width of keratinized gingival (p=0.002,0.002,0.002). Similarly intra group analysis for group II from baseline to 1month, 3 months and 6 months with respect to length of recession (p = 0.001,0001,0.002) width of recession (p=0.002,0.002,0.002) statistically significant reduction was observed and significant gain was seen with width of keratinized gingival (p=0.001,0.001,0.001) [Table/Fig-3,4 and 5].
Clinical parameters from baseline to 1 month, 3 months,6 months for Group I* Significant difference; p<0.05 wilcoxon signed rank test
| Group I (Amnion membrane) |
|---|
| Length of recession | Width of recession | Width of keratinized gingiva |
|---|
| Difference | p-value | Difference | p-value | Difference | p-value |
|---|
| 1.25±0.45 | 0.001* | 1.58±0.90 | 0.003* | 1.58±0.67 | 0.002* |
| 1.42±0.67 | 0.002* | 1.75±0.75 | 0.002* | 1.58±0.51 | 0.002* |
| 1.56±0.68 | 0.002* | 2.17±0.58 | 0.002* | 1.42±0.51 | 0.002* |
Clinical parameters from baseline to 1 month, 3 months,6 months for Group II* Significant difference; p<0.05 wilcoxon signed rank test
| Group II (Chorion membrane) |
|---|
| Length of recession | Width of recession | Width of keratinized gingiva |
|---|
| Difference | p-value | Difference | p-value | Difference | p-value |
|---|
| 2.00±0.43 | 0.001* | 1.75±0.75 | 0.002* | 1.17±0.38 | 0.001* |
| 2.00±0.43 | 0.001* | 2.33±1.15 | 0.002* | 1.00±1.15 | 0.001* |
| 2.00±0.85 | 0.002* | 2.50±1.17 | 0.002* | 1.00±0.51 | 0.001* |
Difference in Length of recession(LR), Width of recession(WR) and width of Keratisnised gingiva from base line to 1,3 and 6 months in Group I and II By Wilcoxon Signed Rank test
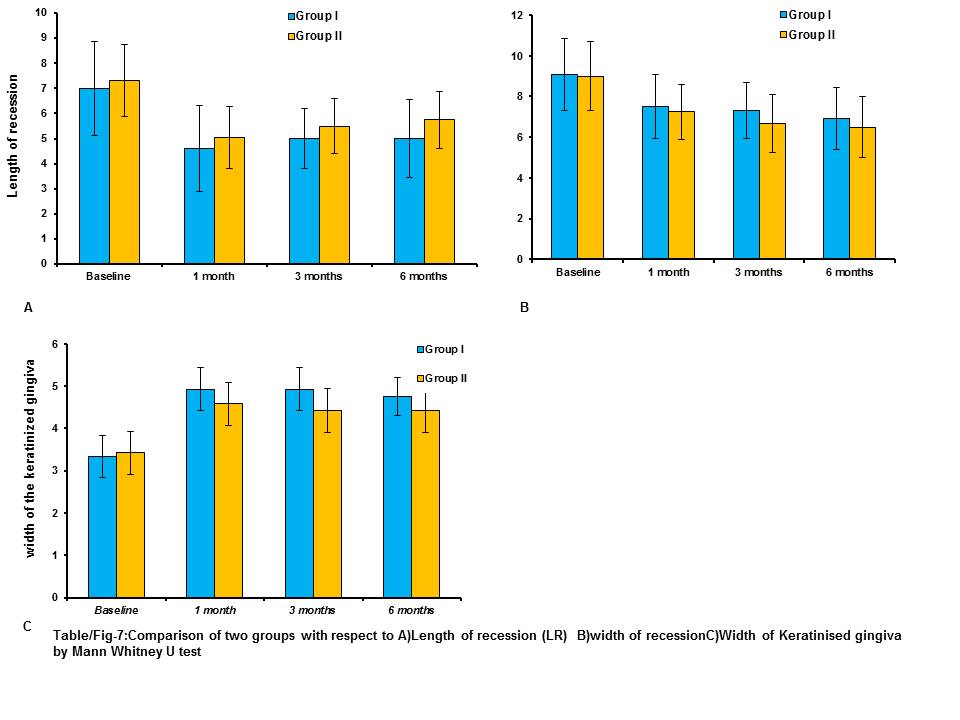
Intergroup comparison [Table/Fig-6,7] for length of recession showed statistically significant difference in both the groups at 1 month (p = 0.038) relating to mean gain of root coverage but no significant differences seen in both the groups at 3 months and 6 months. Comparison of two groups with respect to width of recession (WR) statistically significant difference was seen in both the groups at 3 months (p = 0.001) relating to reduction in width of recession and also at 6 months (p = 0.001). There was increase in the width of keratinized gingiva in both the groups. Comparison showed statistical significant difference at 3 months (p = 0.068) but no significant difference was observed at 6 months (p = 0.356) postoperatively.
Comparison of two groups with respect to Length of recession (LR), width of recession and width of keratinised gingival
| Length of recession | Width of recession | Width of keratinized gingiva |
|---|
| Time period | Chorion site | Amnion site | p-value | Chorion site | Amnion site | p-value | Chorion site | Amnion site | p-value |
|---|
| Baseline | 7.00±1.86 | 7.33±1.44 | 0.023* | 9.08±1.78 | 9.00±1.71 | 0.001* | 3.33±0.49 | 3.42±0.51 | 0.454 |
| 1 month | 4.60±1.71 | 5.05±1.24 | 0.038* | 7.50±1.57 | 7.25±1.36 | 0.190 | 4.92±0.51 | 4.58±0.51 | 0.533 |
| 3 months | 5.00±1.81 | 5.50±1.08 | 0.177 | 7.33±1.37 | 6.67±1.44 | 0.001* | 4.92±0.51 | 4.42±0.51 | 0.068§ |
| 6 months | 5.00±1.54 | 5.75±1.14 | 0.125 | 6.92±1.51 | 6.50±1.51 | <0.001* | 4.75±0.45 | 4.42±0.51 | 0.356 |
*- Significant difference p<0.05 Mann-Whitney U test §- Significant difference p>0.05 Mann-Whitney U test
Comparison of two groups with respect to: a) Length of recession (LR); b) width of recession C)Width of Keratinised gingiva by Mann Whitney U-test
Discussion
Increasing awareness and high esthetic needs of patient are primary reason for the root coverage procedures. Predictable root coverage of exposed roots is the important aspect of treatment approach.
Coronally advanced flap is a simple procedure that fulfills patient’s expectations in terms of preventing discomfort to the palate, as happens with free gingival graft or connective tissue graft and avoids a second surgery. The CAF technique was shown to be a predictable method for gingival recession coverage with clinically satisfactory results [14,15]. The greatest recurrence of recession and poor long term stability seems to occur after coronally advanced flap therapy alone, while the interposition of a graft seems to enhance the stability of the gingival margin [11,16].
Patients reported minimal pain, discomfort postoperatively and uneventful soft tissue healing was observed in both the groups. These results suggest that both amnion membrane and chorion membrane is relatively safe material for clinical use. Mean gain of attachment level at 6 months for amnion and chorion treated sites was 2.17 mm and 1.58 mm respectively. Statistically significant gain in attachment was seen in both the groups at 1 month (p = 0.050) however no significant difference was seen at 3 months (p = 0.282) and 6 months (p = 0.594). Brain Gurisky et al., [4], reported a range of 1.2±1.51mm of clinical attachment gain with amnion membrane which compares well with the results obtained in the present study.
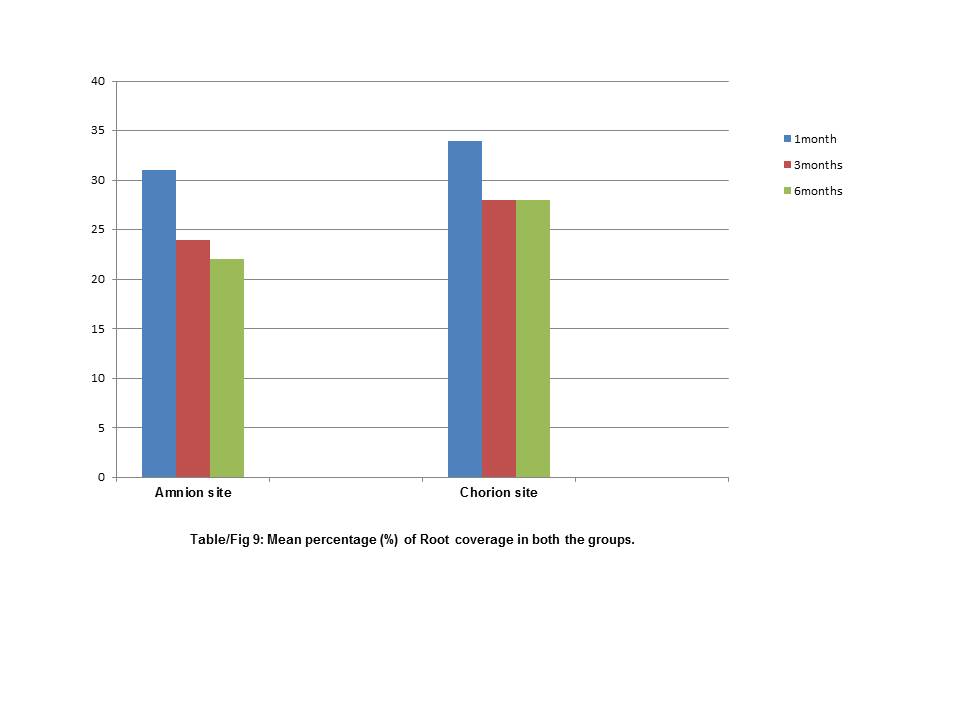
The mean gain of root coverage at 6 months for amnion site was 1.58 mm and 2mm for chorion site. There was statistically significant difference seen in both the groups at 1 month (p = 0.038) relating to mean gain of root coverage but no difference was seen in both the groups at 3 months and 6 months. But the overall mean percentage of root coverage for amnion and chorion group was 22% and 34% respectively [Table/Fig-8,9]. In the present study depth of recession was in the range of 2-3mm, as reported by Pini Prato sites with deeper recession defects tend to respond more favourably than shallower sites [17,18]. However the difference in the percentage of root coverage between the groups could be related to the physical properties of the chorion membrane, presence of mitogenic factors and anti-inflammatory proteins. Reduction in the width of recession was statistically significant between both the groups from baseline to 1 month, 3 months and 6 months. The recession width reduction compares well within the range of the results obtained by Evandro [19].
Mean Percentage of Root Coverage
| Group | 1 month | 3 months | 6 months |
|---|
| Group I Amnion site | 31% | 24% | 22% |
| Group II Chorion site | 34% | 28% | 28% |
Mean percentage (%) of Root coverage in both the groups
Comparison of two groups with respect to Relative attachment level (RAL)
| Relative attachment level | Group I | Group II | p-value |
|---|
| Baseline | 9.00+1.86 | 9.331+1.44 | 0.023* |
| 1 month | 7.17+1.90 | 8.00+1.41 | 0.050* |
| 3 months | 7.08+1.73 | 7.83+1.27 | 0.282 |
| 6 months | 6.83+1.53 | 7.75+1.22 | 0.594 |
*- Significant difference P<0.05 Mann-Whitney U test
The mean increase in width of attached gingiva was 1 mm at amnion site and 1.42 at chorion site by 6 months. There were statistically significant difference seen in both the groups at 3 months (p = 0.068) relating to gain in width of attached gingiva but no statistically significant difference seen at 6 months (p = 0.356). Brain Gurinsky et al., [4] reported 3.2 mm gain of attached gingiva at 3 months postoperative using amnion membrane.
The advantages of using this membrane are: adequate amount membrane available for single use, avoids second surgical site, limits post-operative morbidity, non-immunogenic, available in different dimensions and good shelf life (2 years) [20]. Data suggests the amnion basement membrane closely mimics the basement membrane of human oral mucosa [21,22]. Acellular dermal matrix which is an acellular biocompatible human connective tissue matrix; this allograft of human skin is processed to eliminate the epithelium and all cellular components of the connective tissue and then freeze-dried. A histology study in human samples compared therapy with connective tissue grafts, acellular dermal matrix grafts and coronally advanced flap, and identified the formation of a dense layer of collagen attached to the root surface and unaffected underlying alveolar bone in the three groups and concluded that acellular dermal matrix grafts can be successfully and safely used for root coverage [23].
Both amnion membrane and chorion membrane showed improvements in the various clinical parameters which include, decrease in recession depth, recession width, increase in width of attached gingiva, gain in attachment level and excellent gingival colour match but chorion membrane had better handling properties compared to amnion membrane as Chorion is thicker than amnion membrane.
Compared to other allografts membrane the thickness of amnion and chorion is less, however an added advantage with amnion and chorion allograft is to self-adhere at the site which aids in the stabilization of the membrane [4]. Although not specifically recorded during this study, processed amnion and chorion allograft demonstrated excellent esthetic results in terms of texture and colour match. Both the membranes have good shelf life, easily available, support healing and cost effective compared to other allografts, hence not an added cost for the patient. Keeping in mind the results of the study, both amnion and chorion membrane seem to be favourable allograft to be used in root coverage procedures.
Conclusion
Within the limitations of the study both amnion and chorion allografts seem to be promising novel tissue engineered biomaterials. Rich source of stem cells, enhancement of healing and self-adhering property make these membranes an effective option for root coverage procedures. However randomised control trials with longer followup period need to be carried out to assess the long term benefits of amnion and chorion allografts.
*- Significant difference p<0.05 Mann-Whitney U test §- Significant difference p>0.05 Mann-Whitney U test
*- Significant difference P<0.05 Mann-Whitney U test