Time is of the essence and that certainly holds true for a histopathology practice. Decalcification of hard tissues, namely bone and tooth specimens, forms an important aspect of routine histopathology practice, but is often a time-consuming procedure that may lead to undue delay in diagnosis. There are several methods that have been used for decalcification such as use of acids, chelation, electrolysis and microwaves. Each has its advantages as well as drawbacks. Though faster, use of acids and microwave radiation may potentially result in damage to tissues. Chelation and electrolysis preserve tissues better but are slow processes and impractical in routine use. Determination of the choice of decalcification technique entails a balance between speed of decalcification and maintenance of tissue morphology and quality of staining.
Heat and agitation are two simple methods known to accelerate the decalcification process [1–3]. Through the present study we compared the rate of decalcification of bone and teeth specimens using the conventional method (with Gooding and Stewart’s fluid comprised of 10% formal formic acid) [1] and two modifications of the same, namely heating to 45oC and physical agitation using a magnetic stirrer. In addition, we compared the cellular characteristics and staining quality among the three aforementioned methods in order to assess efficacy of heat and agitation of acid solution versus acid solution alone in decalcification procedures in a routine histopathology laboratory setup.
Materials and Methods
Fifteen weight-matched specimens each of teeth and bone fragments of caprine origin dentate jaw of a single domestic goat (Capra hircus) was obtained thereby ensuring uniformity in the tissue quality of the study sample. The distribution of the sample is depicted in [Table/Fig-1]. The study was performed in the year 2014 in the Department of Oral Pathology, Manipal College of Dental Sciences, Mangalore, Manipal University, Karnataka, India.
Soft tissue specimens obtained from archival non-lesional human skin were also placed along with the bone specimens in order to assess the effect of acid treatment on soft tissues. All the specimens were initially fixed in 10% neutral buffered formalin for at least 48 hours. Hard tissues were subjected to decalcification by three techniques:
Gooding and Stewart’s fluid, {100 ml of Gooding Stewart fluid, composed of 90% formic acid (10ml), 40% formaldehyde (5ml) and distilled water (85ml)} [1],
Gooding and Stewart’s fluid heated to 45oC in a hot air oven for 6 hours daily and
Gooding and Stewart’s fluid agitated using a magnetic stirrer for 6 hours daily.
The volume of decalcifying fluid was not less than 20 times that of the specimen and the fluid was replaced daily till the completion of decalcification. The end point of decalcification was determined by the chemical end-point test (Clayden, 1952) whereby absence of precipitate for 30 minutes marked the completion of decalcification [2]. The difference in rate of decalcification, effect of acid on tissue staining properties and tissue integrity between the three techniques were compared using the variables described in [Table/Fig-2].
| Tissue | Parameter | Scoring |
|---|
| Teeth | a) Pulp shrinkage | Present= 0 |
| Absent= 1 |
| b) Nuclear-cytoplasmic contrast of pulp cells | Poor= 0 |
| Average= 1 |
| Good= 2 |
| c) Odontoblast layer | Missing= 0 |
| Intermediate= 1 |
| Distinct= 2 |
| Bone | a) Folds | Present= 0 |
| Absent= 1 |
| b) Osteocyte retraction | Missing osteocytes= 0 |
| Intermediate= 1 |
| Minimum retraction= 2 |
| c) Bone marrow cellular nuclear-cytoplasmic contrast | Poor= 0 |
| Average= 1 |
| Good= 2 |
| Soft tissue | a) Eosinophilia | Weak= 0 |
| Moderate= 1 |
| Intense= 2 |
| b) Nuclear-cytoplasmic contrast | Poor= 0 |
| Average= 1 |
| Good= 2 |
| c) Chromatin condensation | Indistinct= 0 |
| Distinct= 1 |
Statistical Analysis
The mean time period taken for complete decalcification was compared between the three techniques using Kruskal Wallis test followed by Bonferroni’s post-hoc analysis. Qualitative variables were compared using Fisher’s exact test. P-value less than 0.05 was considered as significant.
Results
There was significant reduction in time taken for decalcification in the modified methods that used heat and mechanical agitation/stirring along with Gooding Stewart’s fluid as compared to conventional method (Gooding Stewart’s fluid only). For bone specimens, decalcification was fastest by the agitation method (median=7days), followed by heating (median=8 days) and the conventional method (median=11 days). On comparison it was found that this difference was statistically significant in conventional vs. heating method; as well as between conventional vs. agitation methods. For teeth, heating method was fastest (median=7 days) followed by stirring (median=8 days) and the conventional method (median=10 days) [Table/Fig-3]. Decalcification of teeth was significantly faster by use of heating than conventional and stirring techniques.
Comparison of rate of decalcification between the conventional technique of decalcification and modifications using heat and mechanical stirring. (Kruskal Wallis test)
| | n (days) | Minimum (days) | Maximum (days) | Median | Mean Rank | Chi-Square | df | Asymp. Sig. | Posthoc Bonferroni’s test |
|---|
| BONE | Conventional | 5 | 10 | 11 | 11 | 13 | 11.509 | 2 | 0.003 | Conventional is significantly different from heat and stirring. |
| Heat | 5 | 7 | 9 | 8 | 7.3 |
| Stirring | 5 | 6 | 8 | 7 | 3.7 |
| TEETH | Conventional | 5 | 8 | 11 | 10 | 12.2 | 10.233 | 2 | 0.006 | Heating is significantly different from conventional and stirring |
| Heat | 5 | 6 | 8 | 7 | 3.4 |
| Stirring | 5 | 8 | 9 | 8 | 8.4 |
The cytomorphologic details of tissues were evaluated by way of variables described [Table/Fig-2] to assess the effect of acid treatment in the three techniques used. Modified methods using heat and mechanical agitation showed higher proportion of artefacts in bone in terms of folds (p=0.5) and poorer bone marrow cell nuclear details (p=0.201). However, the method employing stirring demonstrated less osteocyte retraction (p=0.045); [Table/Fig-4,5].
Comparison of staining and cellular characteristics of bone, teeth and soft tissue sections in decalcification by the three methods. (Fishers exact test)
| TISSUE | FEATURES | ASSESSMENT | CONVENTIONAL | HEAT | STIRRING | FISHERS EXACT | p-value |
|---|
| Count | Column n % | Count | Column n % | Count | Column n % |
|---|
| BONE | BONE MARROW CELL NUCLEAR DETAILS | Poor | 1 | 20 | 4 | 80 | 4 | 80 | 4.438 | 0.201 |
| Average | 4 | 80 | 1 | 20 | 1 | 20 |
| Good | 0 | 0 | 0 | 0 | 0 | 0 |
| FOLDS | Present | 2 | 40 | 4 | 80 | 4 | 80 | 2.184 | 0.500 |
| Absent | 3 | 60 | 1 | 20 | 1 | 20 |
| OSTEOCYTE RETRACTION | Missing osteocytes | 0 | 0 | 3 | 60 | 0 | 0 | 8.509 | 0.045 |
| Intermediate | 1 | 20 | 2 | 40 | 2 | 40 |
| Minimum retraction | 4 | 80 | 0 | 0 | 3 | 60 |
| TOOTH | PULP SHRINKAGE | Present | 2 | 4 | 2 | 40 | 3 | 60 | 0.709 | 1.000 |
| Absent | 3 | 60 | 3 | 60 | 2 | 40 |
| PULP NUCLEAR CONTRAST | Poor | 0 | 0 | 0 | 0 | 0 | 0 | 8.087 | 0.021 |
| Average | 0 | 0 | 4 | 80 | 4 | 80 |
| Good | 5 | 100 | 1 | 20 | 1 | 20 |
| ODONTOBLAST STATUS | Missing | 0 | 0 | 2 | 40 | 1 | 20 | 4.16 | 0.500 |
| Intermediate | 1 | 20 | 2 | 40 | 1 | 20 |
| Distinct | 4 | 80 | 1 | 20 | 3 | 60 |
| SOFT TISSUE | EOSINOPHILIA | Weak | 1 | 20 | 2 | 40 | 0 | 0 | 6.101 | 0.162 |
| Moderate | 1 | 20 | 2 | 40 | 0 | 0 |
| Intense | 3 | 60 | 1 | 20 | 5 | 100 |
| NUCLEAR CONTRAST | Poor | 1 | 20 | 0 | 0 | 4 | 80 | 7.975 | 0.065 |
| Average | 3 | 60 | 3 | 60 | 0 | 0 |
| Good | 1 | 20 | 2 | 40 | 1 | 40 |
| CHROMATIN | Poor | 5 | 100 | 3 | 60 | 2 | 40 | 4.187 | 0.251 |
| Average to good | 0 | 0 | 2 | 40 | 3 | 60 |
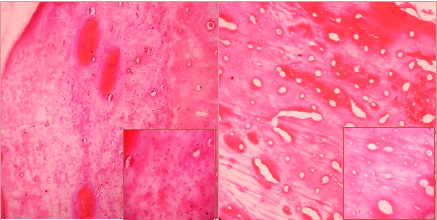
Left: Bone specimen decalcified by the conventional method exhibiting intact osteocytes within lacunae. Right: Bone specimen decalcified by the heat method exhibiting osteocyte retraction. (H&E, 100X) Inset shows magnified image (400X)
On assessment of teeth specimens decalcified by the three methods, it was seen that nuclear-cytoplasmic contrast of pulp cells significantly deteriorated on both heating and stirring wherein most specimens demonstrated only average nuclear-cytoplasmic contrast. All teeth specimens decalcified by the conventional technique exhibited good nuclear-cytoplasmic contrast (p=0.021); [Table/Fig-6]. However, no significant difference was seen in the amount of pulp shrinkage between the three methods. A trend for increased pulp shrinkage was noted with the stirring technique. It was also noted that the odontoblast layer was distinct in 20% of the specimens subjected to decalcification by heat in contrast to 80% and 60% in the conventional and stirring methods respectively [Table/Fig-4].
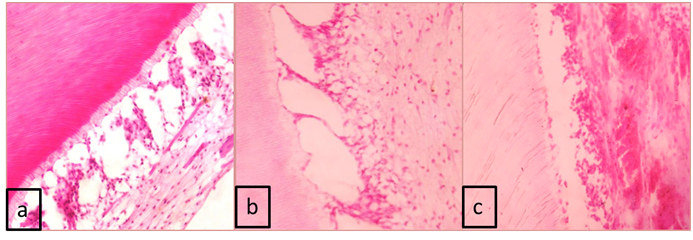
Tooth decalcified by the conventional method: (a) exhibiting pulp cells which demonstrate good nuclear contrast. Nuclear contrast of pulp cells was diminished in the (b) stirring and (c) heating methods. (H&E, 400X)
In soft tissue sections, increased eosinophilia was seen in the conventional and stirring methods, with intense eosinophilia in all cases in the latter technique (p=0.162). There was no significant difference in nuclear contrast and chromatin visualisation between the three methods [Table/Fig-4].
Discussion
The process of decalcification is aimed at removal of calcium salts from mineralised tissue such as bone and teeth, while preserving the organic portions, thus enabling ease of quality sectioning and subsequent microscopic visualisation of diagnostic utility. There are several methods of decalcification such as chelation, acid decalcification and electrolysis [1–3].
The choice of an appropriate decalcifying agent is essentially conciliation between speed of decalcification and diagnostic quality of the sections. Each method carries with it, advantages and drawbacks. While chelation using EDTA shows excellent preservation of tissues and gives a good histologic impression, it is limited by the fact that it is a very slow process which renders it impractical in routine diagnostic practice [1,3]. This was demonstrated by authors who compared efficacy of formic acid, nitric acid and EDTA as decalcifying agents [4,5]. Strong acids such as hydrochloric acid and nitric acid can decalcify rapidly but they lead to damage to tissues and cause deleterious changes in tissue morphology and stainability [4,6]. Formic acid (a weak acid) is the preferred decalcifier, which while being relatively slower in action, is less damaging to tissues [3,5]. With the aid of simple modifications, acid decalcification can be accelerated as has been evaluated in the present study where we employed formic acid along with factors such as heat and mechanical agitation.
The duration of decalcification is critical for timely diagnosis and treatment planning. The diagnosis of many cysts, intraosseous tumours and fibro-osseous tumours is dependent on assessment of decalcified tissue sections. Information pertaining to the relation of soft tissue to a tooth (in case of dentigerous cyst), involvement of bone by tumour (when determining involvement of surgical excisional margins), resorption pattern and remodelling of bone (in lesions like fibrous dysplasia) etc decide the optimal management of the lesion. Thus, striking the right balance between speed and quality of staining is essential for accurate and timely diagnosis that benefits the clinician and the patient [4,7].
Acid decalcification is the routinely used method in most laboratories. Among the major factors influencing acid decalcification are concentration of the acid, temperature and agitation. Decalcification procedures can be accelerated by employing additional factors such as increase in temperature and mechanical agitation of the decalcifying fluid. Such simple modifications possess the potential to enhance the rate of decalcification. Physical agitation acts dually by increasing diffusion of fluids into specimens and preventing the layer of fluid around the specimen from becoming saturated with calcium, thus driving the chemical reaction involved in acid decalcification forward [1,2,8]. Verdenius and Alma in 1958 compared various methods of decalcification and their modifications namely, different acids, different temperatures, use of vacuum, electric current and physical movement. They observed that the end-point of decalcification was reached in two-thirds the time when agitation was performed as compared to controls [9]. In the present study, mechanical stirring of formic acid solution with the aid of a magnetic stirrer reduced the time of decalcification by four days for bone specimens and by three days for teeth in comparison to conventional technique. Bone is porous and agitation of the decalcifying fluid accelerates the diffusion of decalcifying fluid resulting in faster removal of mineral. Agitation also increases the interaction between the specimen and surrounding decalcifying fluid [9].
Heat is also known to accelerate decalcification as it increases the rate of diffusion and increases the rate of chemical reaction [1,2,9]. In their study, Verdenius and Alma also observed that the time required for decalcification reduced as temperature was increased from 13oC to 25oC to 40oC [9]. Similar findings were noted in the present study where intermittent heating to 45oC in a hot air oven showed fastest decalcification of teeth specimens (4 days shorter than conventional method; [Table/Fig-2]). Agitation was slower than heating by 1 day, but the cellular details of the pulp were better. The presence of pulp in a confined chamber surrounded by enamel (less porous than bone) may have contributed to the better staining quality.
Microwave-aided decalcification has been popularised as another method of hastening the process of decalcification [6,8]. Pitol et al., compared decalcification of maxillary jaw fragments of Wistar rats using 8% Warshawsky solution with constant agitation in one set of specimens and microwave irradiation in another set. They observed increased speed with use of microwave irradiation which was attributed to increased kinetic energy, alteration of electric fields and generation of heat homogenously within the tissue, which in turn enhances diffusion of decalcifying solution [8]. Thus the benefit of accelerated decalcification through microwave irradiation is due to heat generation. It has also been suggested that effective decalcification cannot be carried out in commonly available domestic microwave ovens in the absence of a temperature regulation system [10], as elevation of temperature beyond 55oC to 60oC is deleterious to tissue morphology [8]. Chaudhari et al., in their study on comparison of conventional vs. microwave techniques noted that microwave-aided decalcification using formic acid was not effective as it resulted in either under-decalcification, or over-heating leading to tissue damage [10].
Acids also affect stain ability of tissues and cause morphological alterations such as oedema, shrinkage, vacuolation, disruption and fraying not attributable to the pathologic condition [4,7]. Regardless of the method of decalcification employed, it is imperative that the chosen technique has the least possible adverse effect on staining quality and tissue integrity. To the best of our knowledge, the cytomorphological variables described in [Table/Fig-2] have not been previously compared between conventional acid decalcification technique and its modifications employing heat and agitation. Therefore, along with assessment of speed of decalcification, we aimed to compare cellular detail and staining quality in the three methods.
Although heat can speed up decalcification, increased temperature is also known to cause maceration of tissues. The deleterious effect of acid decalcification as revealed by osteocyte retraction in bone specimens was observed to be significantly increased in the heating method whereas minimal osteocyte retraction was seen in the stirring technique (p=0.045). This could be explained by the fact that the tissue was in contact with acidic solution for the least time in the stirring technique. On the other hand, agitation and heat may have contributed to relatively higher damage to tissues than by the conventional technique, resulting in a higher number of artefacts.
In decalcified teeth specimens, increased exposure to heat may be responsible for the loss of the odontoblast layer of pulp. Most of the tooth specimens subjected to agitation by stirring showed less damage to the odontoblast layer probably due to the relatively protected environment provided by the enclosure by dentin. It is reportedly often difficult to simultaneously achieve optimal microscopic visualisation of mineralised and non-mineralised tissues [7]. Though the nuclear-cytoplasmic contrast was reduced in both the modified methods, it was found to be adequate for histologic assessment in the present study. The choice of accelerated decalcification method must be exercised keeping in view the relative need for examining soft tissue and hard tissue components of the specimens. It is perhaps more suitable to adopt the conventional technique rather than heat or stirring if nuclear and cellular details of soft tissues are pivotal to the diagnosis. In addition, increased agitation which in turn causes increased diffusion of the decalcifying fluid into the tissues may be accountable for the shrinkage of inherently delicate pulpal tissue away from the dentinal wall, as observed in the present study.
We observed an increase in eosinophilia in decalcified tissue which may be ascribed to the fact that staining by acidic dyes is enhanced subsequent to acid treatment [4]. Heat, a factor that is known to impair subsequent staining [11], may explain the absence of increased eosinophilia in specimens that were subjected to the heating method as compared to the conventional and stirring methods. Haematoxylin staining is generally poorer after acid-decalcification as nucleic acids are particularly intolerant to acid decalcification resulting in poor nuclear-cytoplasmic contrast and poor visualisation of chromatin [2,4].
The present study evaluates two factors accelerating the rate of acid decalcification namely heating and agitation of decalcifying fluid with the conventional method using decalcifying fluid alone. It also compares various cytomorphological variables among the three. Our findings suggest that physical agitation of decalcifying fluid may be an acceptable technique of accelerating the rate of decalcification of tooth and bone specimens while obtaining satisfactory quality of tissue morphology and staining. Heating, on the other hand, may result in impaired staining and loss of cellular detail. However, the findings should be supported by further research on larger samples and human specimens. Further work comparing other techniques such as chelation and microwaves alongside acids will aid in identifying practical and effective decalcifying techniques.
Conclusion
Decalcification, an essential procedure in a histopathology practice, often delays the time-bound delivery of histopathological diagnosis. A simple modification to routine decalcification methods such as intermittent physical agitation of the decalcifying fluid with the aid of a magnetic stirrer may be a feasible and practical adjunct in accelerating the process of decalcification of tissues, while simultaneously preventing undue damage to tissue integrity and staining quality.