Low Grade Fibromyxoid Sarcoma of the Palate: A Case Report
Srikanth Soma1, Shriram Bhat2, Sunil Kumar Shetty3
1 Senior Resident, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
2 Professor, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
3 Associate Professor, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Srikanth Soma, B-404, AMSRI Residency, Ameerpet, Hyderabad, Telangana-500016, India.
E-mail: soma_986@yahoo.co.in
Low-grade fibromyxoid sarcoma (LGFMS) are rare soft-tissue sarcomas that usually come to attention as slow growing masses. Males and females are affected approximately equally and typically arising in the soft tissue of the proximal extremities. Primary occurrence within the head and neck is exceedingly rare. We report a case arising from the hard palate of a 40-year-old male and according to our knowledge this is the first ever case of LGFMS involving the palate to be reported.
Fibromyxoidsarcoma, LGFMS, Soft tissue tumour
Case Report
A 40-year-old male presented to us with a growth over the hard palate since 3 months which had been rapidly progressing in size. It was associated with mild dull aching pain and no other symptoms of note. Patient was a known smoker and a regular tobacco chewer. No previous surgical history. No significant family history. A solitary proliferative growth measuring 4×3cm was noted lying in close proximity to the upper alveolus just behind the incisors to the left of midline. Externally the swelling was causing a bulge over the mid part of face. Swelling was non tender on palpation. Rest of the oral cavity examination was normal.
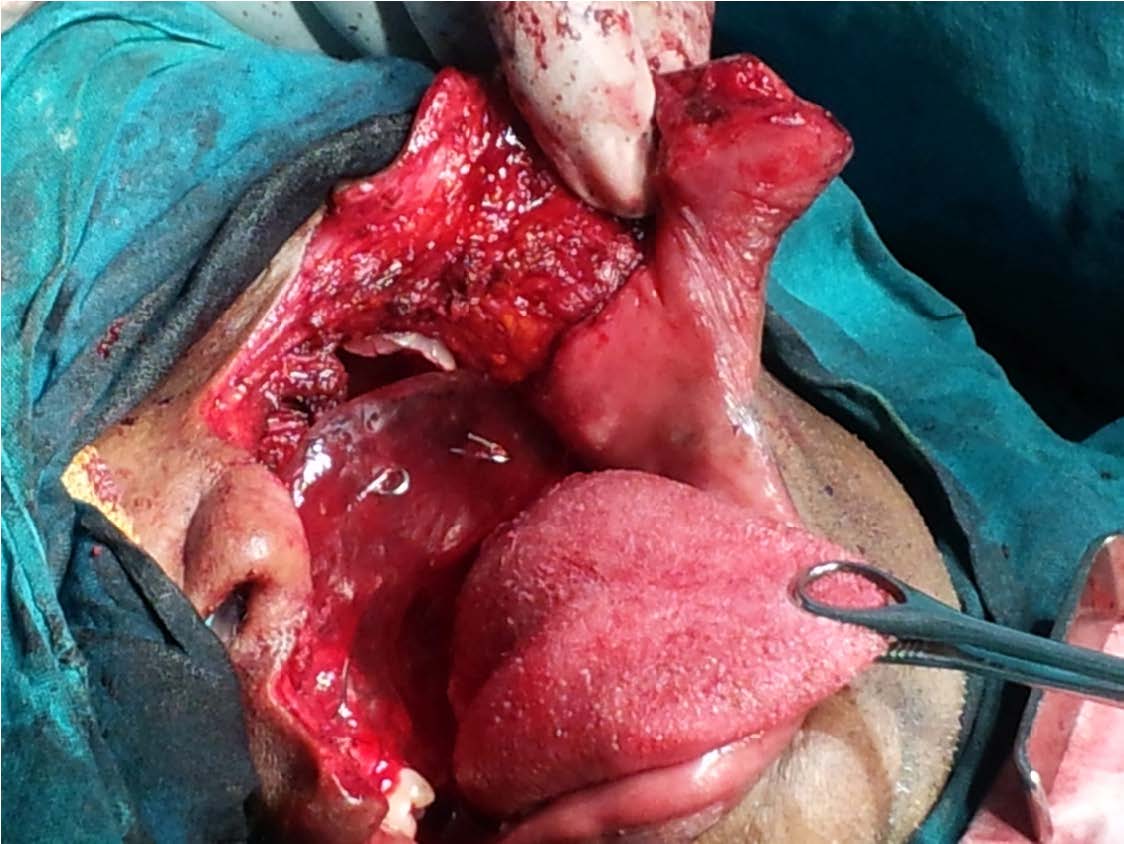
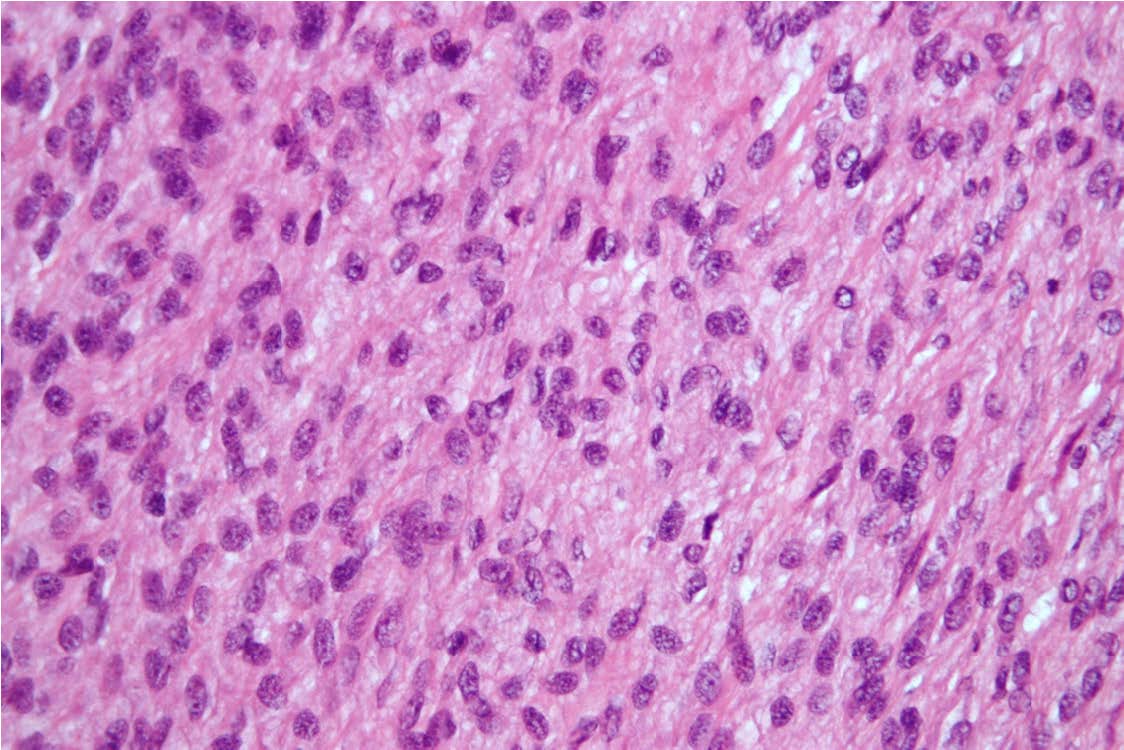
All the routine blood examinations was normal. Contrast enhanced computerized tomography (CECT) of the head and neck revealed a well circumscribed and isodense lesion measuring 5×4 cm involving the anterior half of the hard palate and causing compression of the left maxillary sinus. The patient underwent wide local excision of the tumour under general anaesthesia [Table/Fig-1,2 and 3]. On histopathologic examination, the tumour was multinodular and the nodules typically showed a myxoid character with dense fibrous areas interspersed between them. There was no nuclear pleomorphism/high cellularity/necrosis, and had few mitoses [Table/Fig-4]. The final diagnosis was LGFMS involving the hard palate.
Showing wide local excision of the tumour being performed

Showing the postoperative defect involving the palate being reconstructed with a removable dental prosthesis temporarily
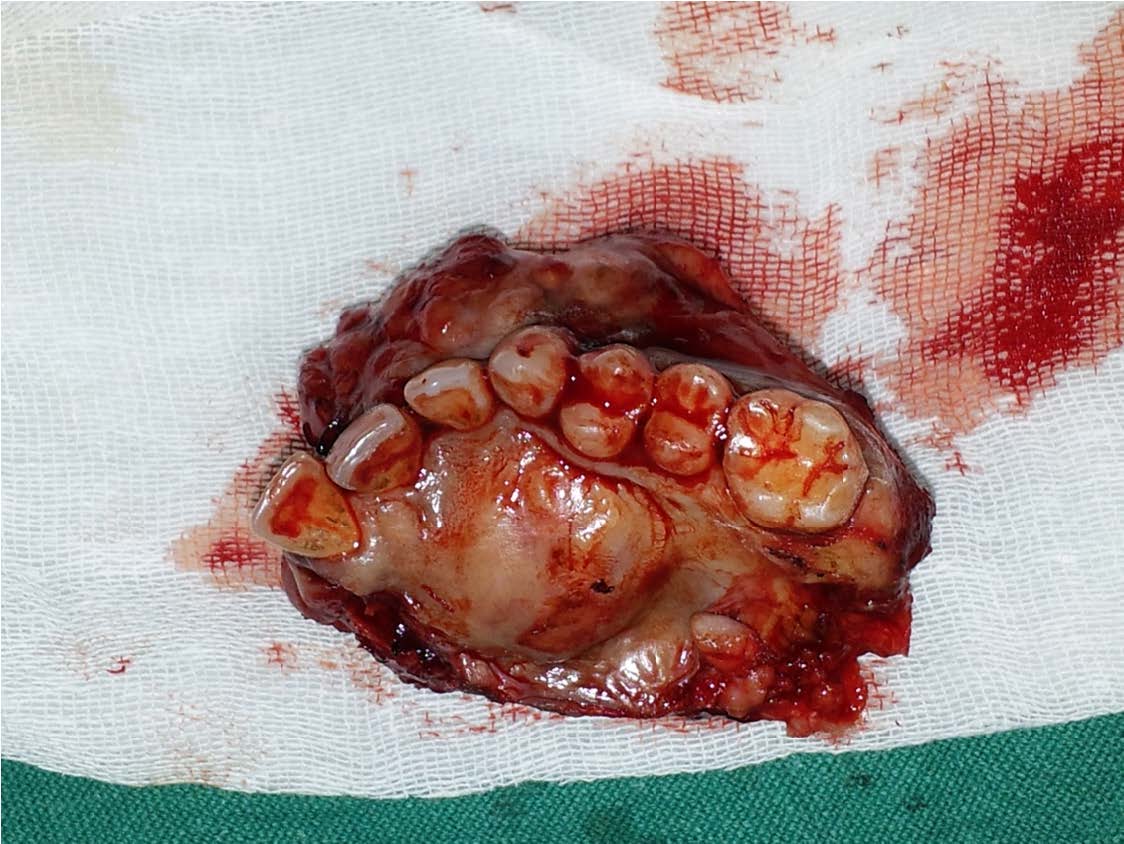
Showing the gross tumour specimen post wide local excision
Microscopic picture showing typical features of LGFMS under very high magnification
The patient was discharged with no adjuvant therapy postoperatively. The patient has been on regular follow up and disease free since 4 months.
Discussion
Low-grade fibromyxoid sarcoma (LGFMS) is a rare soft tissue tumour reported for the first time in the year 1987 by Evans [1]. In 1997, Lane et al., reported that a tumour, diagnosed as hyalinizing spindle cells with giant rosettes (HSCT), was considered a variant of LGFMS [2].
LGFMS, in the majority of cases arises in the deep soft tissue of the lower extremity especially the thigh [3,4]. Most of them arise in the skeletal muscle while a few of them are confined to subcutaneous tissue [3]. There have been cases of these tumours being reported in the chest wall, axilla, shoulder, inguinal region, buttock, neck etc [3,5–7]. Rare reports have also been reported in the retroperitoneum, bowel mesentery, pelvis, foot and the abdominal wall [8–13].
According to our knowledge and extensive search through literature never has been a case reported from hard palate. LGFMS must be differentiated from myxofibrosarcoma as both present clinically in a similar fashion but LGFMS has the propensity to metastasize more often [14]. The latter has uniformly myxoid stroma and does not show whorled pattern of arrangement of cells [9].
These tumours have been reported to recur and metastasize [3,7]. Metastasis also has been reported to occur frequently with lung being a common site. These patients have a prolonged survival even after metastasis disease [15].
Low-grade fibromyxoid sarcomas are soft tissue tumours with aggressive behaviour but with a benign appearance warranting long-term follow-up for all cases. High index of suspicion is required for this rare tumour since early diagnosis with definite surgical intervention is the only modality known to prolong survival while avoiding local recurrences.
Conclusion
In conclusion LGFMS is a very rare disease with multiple diagnostic challenges, as described in our case. Responses to chemotherapy have been poor for these tumours and at present, surgery is the only treatment modality that results in prolonged disease-free periods. Little is known regarding the occurrence of LGFMS in the hard palate and its definitive management. Our case shows that early surgical resection with negative margins will produce fair outcome in terms of survival.
[1]. Evans HL, Low-grade fibromyxoid sarcoma: A report of two metastasizing neoplasms having a deceptively benign appearanceAm J ClinPathol 1987 88:615[PubMed] [Google Scholar]
[2]. Lane KL, Shannon RJ, Weiss SW, Hyalinizing spindle cell tumor with giant rosettes: A distinctive tumor closely resembling low-grade fibromyxoid sarcomaAm J Surg Pathol 1997 21:1481 [Google Scholar]
[3]. Weiss SW, Goldblum JR, Benign fibro histiocytic tumours. In: Enzinger FM, Weiss SW Mosby, editorIn Soft tissue tumours 2001 4:409-39. [Google Scholar]
[4]. Ugai K, Kizaki T, Morimoto K, Sashikata T, A case of low-grade fibromyxoid sarcoma of the thighPathol Int 1994 44:793-99.[PubMed] [Google Scholar]
[5]. Husek K, Janicek P, Jelinek O, Low grade malignant fibromyxoid sarcoma [In Czech with English abstract]Cesk Patol 1998 34:139-34.[PubMed] [Google Scholar]
[6]. Zamecnik M, Michal M, Low-Grade Fibromyxoid Sarcoma: A Report of Eight Cases With Histologic, Immunohistochemical, and Ultrastructural StudyAnn Diagn Pathol 2000 4:207-17.doi: 10.1053/adpa.2000.8122. [PubMed] [Cross Ref] [Google Scholar]
[7]. Devaney DM, Dervan P, O’Neill S, Carney D, Leader M, Low-grade fibromyxoidsarcomaHistopathology 1990 17:463-65.[PubMed] [Google Scholar]
[8]. Evans HL, Low-grade fibromyxoid sarcoma. A report of 12 casesAm J Surg Pathol 1993 17:595-600.[PubMed] [Google Scholar]
[9]. Goodlad JR, Mentzel T, Fletcher CD, Low grade fibromyxoid sarcoma: clinicopathological analysis of eleven new cases in support of a distinct entityHistopathology 1995 26:229-37.[PubMed] [Google Scholar]
[10]. Vasudevan G, Shivamurthy A, Low Grade Fibromyxoid Sarcoma of the Mesentery, an Under Recognised Entity: A Case ReportJ Inter disciple Histopathol 2014 [cited June 17, 2015];2(4):228-31. doi:10.5455/jihp.20140612073245 [Google Scholar]
[11]. Shidham VB, Ayala GE, Lahaniatis JE, Garcia FU, Low-Grade Fibromyxoid Sarcoma: Clinicopathologic Case Report With Review of the LiteratureAm J ClinOncol 1999 22:150-55.doi: 10.1097/00000421-199904000-00009. [PubMed] [Cross Ref] [Google Scholar]
[12]. Jagtap SV, Nikumbh DB, Chougule PG, Bohra AO, Jagtap SS, Low grade fibromyxoid sarcoma presented with local recurrence and an extensive foot deformityJournal of Clinical and Diagnostic Research. [serial online] 2012 August [cited: 2015 Jun 17];6:1070-72 [Google Scholar]
[13]. van den Bossche MR, Van Mieghem H, Low-grade fibromyxoid sarcomaOncology 2000 58:207-09.doi: 10.1159/000012101. [PubMed] [Cross Ref] [Google Scholar]
[14]. Mentzel T, Katenkamp D, Fletcher CD, Low malignancy myxofibrosarcoma versus low malignancy fibromyxoid sarcoma. Distinct entities with similar names but different clinical course [in German with English abstract]Pathologe 1996 17:116-21.doi: 10.1007/s002920050142.[PubMed] [Cross Ref] [Google Scholar]
[15]. Folpe AL, Lane KL, Paull G, Weiss SW, Low-grade fibromyxoid sarcoma and hyalinizing spindle cell tumor with giant rosettes: a clinicopathologic study of 73 cases supporting their identity and assessing the impact of high-grade areasAm J SurgPathol 2000 24:1353-60.[PubMed] [Google Scholar]