Miles to Discover in Histological Grading of Odontogenic Tumours
Anjali Narwal1, Anju Devi2, Achla Bharti Yadav3, Virender Singh4
1 Associate Professor, Department of Oral Pathology, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
2 Assistant Professor, Department of Oral Pathology, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
3 Assistant Professor, Department of Oral Pathology, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
4 Professor, Department of Oral Surgery, Post Graduate Institute of Dental Sciences, Rohtak, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anjali Narwal, Associate Professor, Department of Oral Pathology, Post Graduate Institute of Dental Sciences, Rohtak - 124001, Haryana, India.
E-mail: anjalinarwal@yahoo.com
Encapsulated tumour, Sessile mass
Odontogenic tumours (OTs) are lesions of great interest and importance to oral pathologists and maxillofacial surgeons alike, who for several decades have studied, catalogued these lesions and developed modalities for adequate treatment [1]. Ameloblastoma is the most common and most intriguing of all odontogenic tumours. Although benign it is highly polymorphic, due to its ability to undergo various forms of metaplasia. This has given rise to variants of ameloblastoma in which the stimulus for metaplastic change is poorly understood and has been attributed to the multipotentiality of odontogenic epithelium [2].
In the indexed case, 12-year-old boy presented with the complaint of gradually increasing painless growth in lower front teeth region since 8 months. No evident extraoral swelling or asymmetry was noticed. Regional lymph nodes were not clinically palpable and there was no history of trauma to the same site. Intraoral examination revealed approximately a 2.5x4cm, non tender mucosal sessile mass on lingual aspect of anterior mandible extending from central incisor to second premolar on left side obliterating the lower labial vestibule [Table/Fig-1].
Intraoral picture reveals a sessile mass on lingual aspect of anterior mandible

There was a faintly palpable anterior lingual expansion. The mandibular incisors, canine and premolar of left side were found to be non vital on thermal testing. Orthopantomograph (OPG) revealed a well circumscribed unilocular radiolucency in the anterior mandible extending from 44 to 35 without cortication. Thinning of lower border of mandible was seen. Root resorption of associated teeth due to pressure was evident [Table/Fig-2]. Considering the benign nature of the lesion, its site of occurrence i.e. anterior to first molars and unilocular appearance, central giant cell granuloma was considered as provisional diagnosis and excisional biopsy was done.
OPG showing a well circumscribed unilocular radiolucency in the anterior mandible with thinning of lower border

Histopathological sections of this case showed well encapsulated tumour mass with extensive areas of squamous differentiation and features of plexiform ameloblastoma [Table/Fig-3].
Photomicrograph reveals a well encapsulated tumour mass with extensive areas of squamous differentiation mixed with plexiform pattern (H&E, 10X)
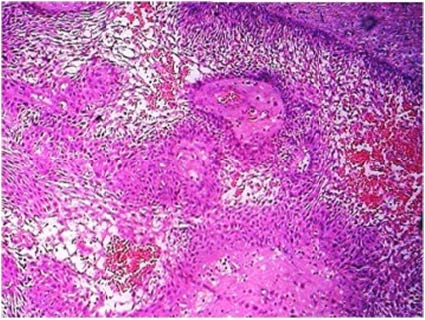
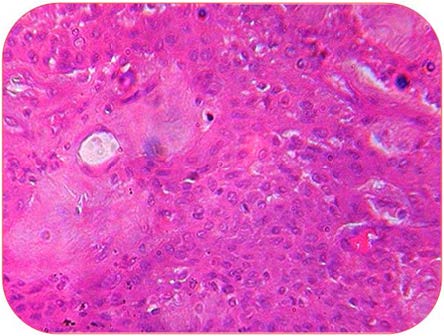
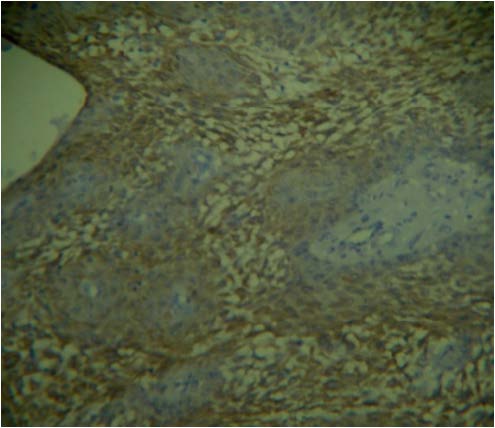
Few areas showed material secretion in the tumour matrix which were suggestive of calcifying epithelial odontogenic tumour but when stained with Congo red, came out to be negative [3]. Calcifications or even multinucleated giant cells were not evident in the submitted tissue. Keratin pearl formation was not seen but individual cell keratinization and squamous differentiation were evident throughout the stroma. The tumour appeared to be in biphasic pattern where at one end the tumour cells appeared to be stretched out making the intercellular ridges prominent whereas at the other end, tumour showed squamous differentiation, loss of intercellular bridges and cohesive tumour cells arranged in thick sheets [Table/Fig-4]. Tumour cells were positive for cytokeratin whereas surrounding material was negative [Table/Fig-5].
Photomicrograph reveals area of cohesive tumour cells with squamous differentiation & loss of intercellular bridges (H&E, 10X)
Photomicrograph shows cytokeratin positivity in tumour cells (H&E, 10X)
After extensive search in literature only three odontogenic tumours which show keratinization or squamous metaplasia were found. Acanthomatous ameloblstoma exhibit squamous metaplasia of stellate reticulum with or without keratin pearl formation [4]. However, in the present case frank keratin or squamous metaplasia was not seen but only squamous differentiation and individual cell keratinization were seen.
Squamous odontogenic tumour also shows squamous metaplasia [5] but in the present case tumour was not arranged in follicles as well as material secretion by tumour cells did not appear to be keratin and tumour cells were not flattened squamous or cuboidal arranged in follicles.
Keratoameloblastoma is a heterogenous group of odontogenic neoplasms which exhibit keratin formation in the connective tissue stroma [6]. Such frank keratin formation was absent in the present case.
The index case is not of intraosseous squamous cell carcinoma as there was no dysplasia and few areas showed frank stellate reticulum like cells. Moreover, the present case is well encapsulated tumour supporting benign nature which is in contradiction to malignancy i.e. squamous cell carcinoma.
[1]. Philipsen HP, Peter A, Reichart. Classification of odontogenic tumours. A historical reviewJ Oral Pathol Med 2006 35:525-29. [Google Scholar]
[2]. Gardner DG, Some current concepts on the pathology of ameloblastomasOral Surg Oral Med Oral Pathol Oral Radiol Endod 1996 82:660-69. [Google Scholar]
[3]. Pindborg JJ, A calcifying epithelial odontogenic tumourCancer 1958 11:838-43. [Google Scholar]
[4]. Anneroth G, Heimdahl A, Wersall J, AcanthomatousameloblastomaInt J Oral Surg 1980 9(3):231-36. [Google Scholar]
[5]. Badni M, Nagaraja A, Kamath VV, Squamous odontogenic tumour- a case report and review of literatureJ Oral MaxillofacPathol 2012 16(1):113-17. [Google Scholar]
[6]. Adeyemi BF, Adisa AO, Fasola AO, Akang EE, Keratoameloblastoma of the mandibleJ Oral Pathol 2010 14(2):77-79. [Google Scholar]