Background
The high incidence of IUGR and its low recognition lead to increasing perinatal morbidity and mortality for which prediction of IUGR with timely management decisions is of paramount importance. Many studies have compared the efficacy of several gestational age independent parameters and found that TCD/AC is a better predictor of asymmetric IUGR.
Aim
To compare the accuracy of transcerebellar diameter/abdominal circumference with head circumference/abdominal circumference in predicting asymmetric intrauterine growth retardation after 20 weeks of gestation.
Materials and Methods
The prospective study was conducted over a period of one year on 50 clinically suspected IUGR pregnancies who were evaluated with 3.5 MHz frequency ultrasound scanner by a single sonologist. BPD, HC, AC and FL along with TCD were measured for assessing the sonological gestational age. Two morphometric ratios- TCD/AC and HC/AC were calculated. Estimated fetal weight was calculated for all these pregnancies and its percentile was determined.
Statistical Methods
The TCD/AC and HC/AC ratios were correlated with advancing gestational age to know if these were related to GA. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and diagnostic accuracy (DA) for TCD/AC and HC/AC ratios in evaluating IUGR fetuses were calculated.
Results
In the present study, linear relation of TCD and HC in IUGR fetuses with gestation was noted. The sensitivity, specificity, PPV, NPV & DA were 88%, 93.5%, 77.1%, 96.3% & 92.4% respectively for TCD/AC ratio versus 84%, 92%, 72.4%, 95.8% & 90.4% respectively for HC/AC ratio in predicting IUGR.
Conclusion
Both ratios were gestational age independent and can be used in detecting IUGR with good diagnostic accuracy. However, TCD/AC ratio had a better diagnostic validity and accuracy compared to HC/AC ratio in predicting asymmetric IUGR.
Fetal cerebellum, Gestational age, Growth restriction, Ultrasound
Introduction
The high incidence of intrauterine growth retardation (IUGR) in general obstetric population (~10%) and its low recognition (< 40%) together lead to increasing perinatal morbidity and mortality. Regular surveillance and timely management decisions is cornerstone for optimum outcome in these cases, which rely mainly on accurate determination of gestational age [1].
Transcerebellar diameter (TCD) is the maximum transverse diameter of the fetal cerebellum. The fetal cerebellar hemispheres are located in the posterior cranial fossa which is resistant to external pressure and growth deviations, thus making it a better indicator for determination of gestational age [1]. Conversely, fetal abdominal circumference (AC) is the earliest affected parameter in the process of impaired fetal growth. Thus, a ratio of TCD/AC which is gestational age independent is very useful in predicting IUGR. Head circumference is another parameter which remains minimally affected by external pressure effects causing deformation of fetal head and by growth alterations. HC/AC ratio is another gestational age independent parameter which may be used in predicting IUGR.
Many studies have compared the efficacy of several gestational age independent parameters and found that TCD/AC is a better predictor of asymmetric IUGR.
Aim of The Study
To compare the accuracy of transcerebellar diameter/ abdominal circumference with head circumference/abdominal circumference in predicting asymmetric intrauterine growth retardation after 20 weeks of gestation.
Ultrasound Appearance of Cerebellum [
1]
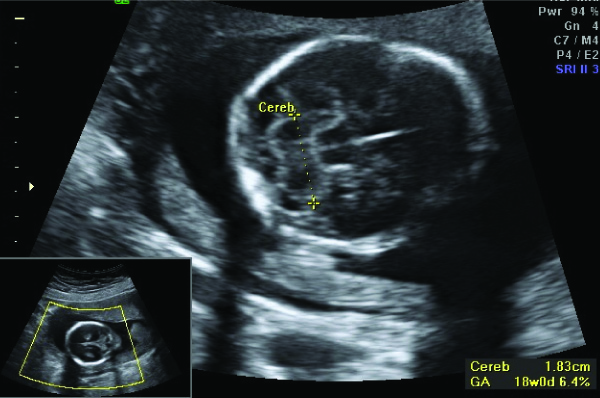
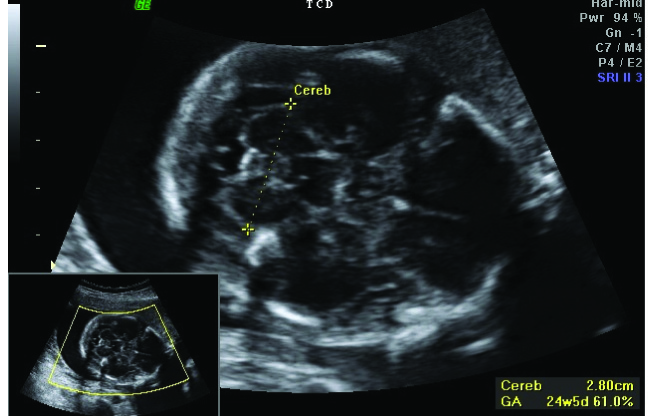
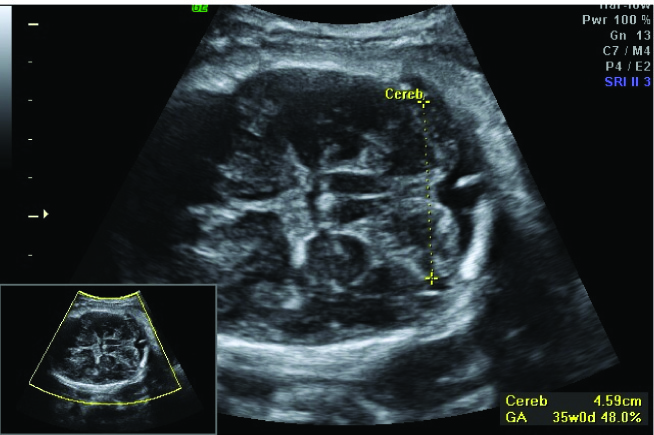
The fetal cerebellum has a characteristic appearance on ultrasound which changes gradually in shape and echogenicity with advancing gestational age. It has been graded based on its shape as grade I with ‘eyeglass’ [Table/Fig-1] at 12–16 weeks, grade II with ‘dumbbell’ [Table/Fig-2] at 16 – 28 weeks and grade III with ‘fan’ shape [Table/Fig-3] during third trimester and early postnatal life. There is gradual increase in echogenicity from hypoechoic changing to slightly echoic and finally to homogeneously hyperechoic in third trimester.
Grade I cerebellum. The cerebellum is seen between the calipers
Grade II cerebellum. The cerebellum is seen between the calipers
Grade III cerebellum. The cerebellum is seen between the calipers
Cerebellar View: Obtained by rotating the transducer in the axial plane centred on the thalamus to show the cerebellar hemispheres. This view shows the cerebellum, the cisterna magna, the cavum septi pellucidi and frequently, the anterior horns of the lateral ventricles.
Transverse cerebellar diameter (TCD): TCD is measured by placing callipers on the outer margins of cerebellum visualised in the above mentioned plane.
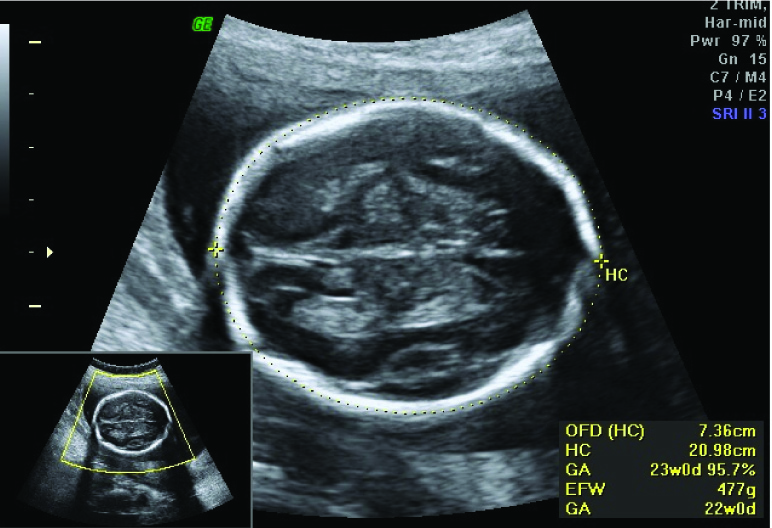
Head circumference (HC): [Table/Fig-4] HC is measured on an axial plane traversing thalami and cavum septum pellucidum with the transducer perpendicular to the central axis of the head. The cerebral hemispheres and calvaria should appear symmetric and the cerebellar hemispheres should not be visible on this plane. The ellipse must be drawn with calipers around the outer aspects of the calvarium.
Head circumference (HC) measurement
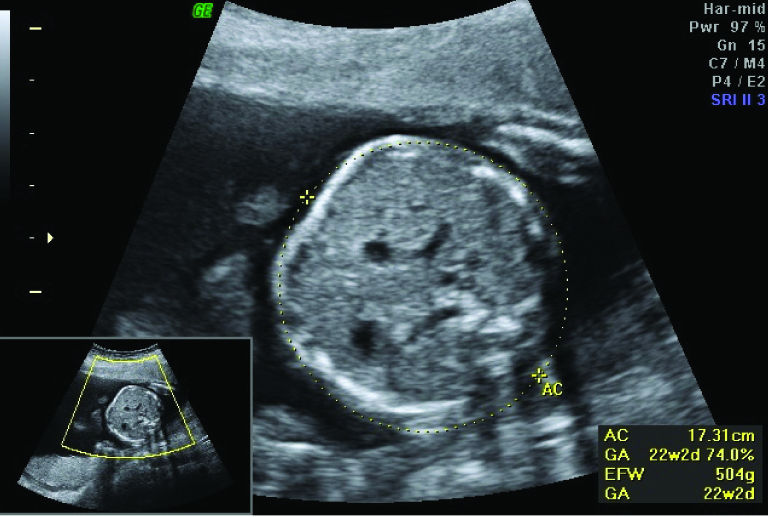
Abdominal Circumference (AC): [Table/Fig-5] AC is measured on axial plane containing fetal stomach bubble, umbilical vein and portal sinus. The calipers should be on the skin surface.
Abdominal circumference measurement
TCD/AC Ratio: The cerebellum is located in the posterior cranial fossa well protected within the strong bones (petrous temporal and occipital bones) forming it, thus withstanding the extrinsic pressure better than the parietal bones [2]. It is relatively resistant to hypoxia due to brain sparing phenomenon leading to maintained blood supply to brain at the cost of systemic supply [3]. Abdominal circumference reflects the size of the liver (which correlates with the degree of fetal malnutrition) as well as the volume of subcutaneous plane. Therefore, AC predicts growth restriction more accurately than either BPD or FL [4]. However, of the four basic ultrasound measurements the AC generally had the largest reported variability. This is partly attributed to the fact that AC is more acutely affected by growth disturbances than the other basic parameters [5]. Hence, a morphometric ratio of TCD/AC can be used to predict asymmetrical IUGR.
HC/AC Ratio: This ratio compares the preserved organ in the malnourished fetus, the brain, with the most compromised, the liver and is of significant value in identifying asymmetric IUGR fetuses.
Materials and Methods
A prospective study was conducted over a period of one year from June 2012 to May 2013 on 50 clinically suspected IUGR pregnancies after ethical clearance. We included all singleton, non anomalous pregnancies beyond 20 weeks of gestation presented with favourable lie to visualise posterior fossa.
The exclusion criteria included multiple gestation, anomalous pregnancies, moderate to severe polyhydramnios, previous irregular menstrual cycles, maternal age <18 or >35 years, symmetrical IUGR, doubtful or unknown last menstrual period. The clinical history, LMP, period of gestation of pregnancy was noted along with other available laboratory parameters. All the 50 patients underwent initial antenatal scan with a 2-5 MHz probe, optimising the frequency to 3.5 MHz for better visualisation of the fetus. Confirmation of singleton/multiple pregnancies, evaluation of fetal anomalies was done. Liquor volume and placental location were also confirmed. Routine parameters like BPD, HC, AC and FL were measured for assessing the sonological gestational age and correlated with last menstrual period. The TCD was obtained by rotating the transducer in the axial plane centering on the thalamus to delineate the cerebellar hemispheres and placing the callipers on the outer margins of cerebellar hemispheres. The TCD, HC and AC obtained at the time of scan were used to provide two morphometric ratios - TCD/AC and HC/AC. Estimated fetal weight was calculated for all these pregnancies and its percentile was determined. All measurements were performed by the same sonologist.
Statistical Methods
The TCD/AC and HC/AC ratios were correlated with advancing gestational age to know if these morphometric ratios were related to gestational age. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and diagnostic accuracy for TCD/AC and HC/AC ratios in evaluating IUGR fetuses were calculated.
Results
In the present study, 50 pregnant women between 18-35 years of age showing asymmetrical foetal IUGR were examined with majority of them (28%) being in the age group 27-29 years [Table/Fig-6]. In majority of these pregnancies, the gestational age was between 34 to 36 weeks, accounting for 30% of population [Table/Fig-7]. Seventy percent of patients were primigravida [Table/Fig-8].
Age distribution of patients studied in IUGR pregnancies
| Age group year | N (number of patients) | Percentage (%) |
|---|
| 18-20 | 11 | 22 |
| 21-23 | 12 | 24 |
| 24-26 | 10 | 20 |
| 27-29 | 14 | 28 |
| 30-32 | 2 | 4 |
| 33-35 | 1 | 2 |
| Total | 50 | 100 |
Period of gestation among IUGR pregnancies
| Gestational period | N (number of cases) | Percentage (%) |
|---|
| 20-21wk 6d | - | - |
| 22-23w 6d | - | - |
| 24-25w 6d | - | - |
| 26-27w 6d | 1 | 2 |
| 28-29w 6d | 3 | 6 |
| 30-31w 6d | 4 | 8 |
| 32-33w 6d | 8 | 16 |
| 34-35w 6d | 15 | 30 |
| 36-37w 6d | 13 | 26 |
| 38-39w 6d | 6 | 12 |
| Total | 50 | 100 |
Gravidity distribution in IUGR pregnancies
| Gravidity | N (number of patients) | Percentage (%) |
|---|
| Primi | 35 | 70 |
| Multi | 15 | 30 |
| Total | 50 | 100 |
TCD/AC ratio [Table/Fig-9]: The study showed that there is poor correlation (r2=0.13, p>0.05) between TCD/AC and gestational age after 20 weeks. Therefore, even though there was slight increase in the TCD/AC ratio with gestational age, this increase is insignificant suggesting that this ratio will be constant at any gestational age. The mean TCD/AC was 13.63±1.2% (2SD). In the present study, TCD/AC ratio in predicting IUGR had sensitivity of 88%, specificity of 93.5%, with positive predictive value of 77.1%, and negative predictive value of 96.3% and overall diagnostic accuracy was 92.4%.
Scatter graph showing variation of TCD in advanced pregnancies (beyond 20 weeks) among IUGR fetuses
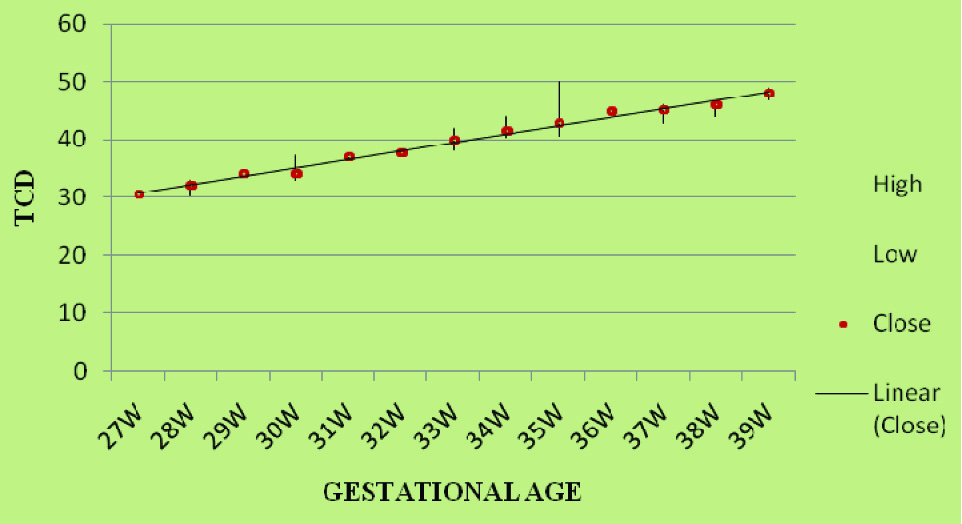
TCD/AC ratio was an age independent parameter that was used in diagnosis of IUGR due to good diagnostic accuracy (92.4%) and specificity (93.5%). The p-value for this study is <0.0001, suggesting that this study is significant.
HC / AC ratio [Table/Fig-10]: In our study, HC/AC ratio in predicting IUGR had sensitivity of 84%, specificity of 92%, with positive predictive value of 72.4%, and negative predictive value of 95.8% and diagnostic accuracy of 90.4%. HC/AC ratio was also an age independent parameter that was used in diagnosis of IUGR due to good diagnostic accuracy (90.4%) and specificity (92%). The P-value for this study is <0.0001, suggesting that this study is significant.
Scatter graph showing variation of HC in advanced pregnancies (beyond 20 weeks) among IUGR foetuses.

Comparison of various parameters of TCD/AC with HC/AC in diagnosing asymmetrical IUGR
| Parameters | TCD / AC % | HC / AC % |
|---|
| Sensitivity | 88 | 84 |
| Specificity | 93.5 | 92 |
| PPV | 77.1 | 72.4 |
| NPV | 96.3 | 95.8 |
| Diagnostic accuracy | 92.4 | 90.4 |
In our study, linear relation of transverse cerebellar diameter in IUGR fetuses with gestation was noted with correlation coefficient (r) being 0.99464 and the coefficient of determination (r2) being 0.98931. We also noted a linear relation of head circumference in IUGR fetuses with gestation with correlation coefficient (r) being 0.97307 and the coefficient of determination (r2) being 0.94867. TCD/AC ratio had a better diagnostic validity and diagnostic accuracy compared to HC/AC in predicting asymmetric IUGR. The fact that TCD is least affected in fetal growth restriction supports the hypothesis that human cerebellar growth is relatively resistant to chronic hypoxemia as a result of the brain sparing phenomenon.
Discussion
The transcerebellar diameter (TCD) is a measurement in posterior cranial fossa which is relatively resistant to external compression due to its strong bony walls. It is also less affected than the head circumference suggesting a preferential mechanism in the preservation of cerebellar growth relative to other cerebral structures [6]. In view of this fact sonographic measurement of TCD serves as an independent and reliable correlate of gestational age (GA) against which potential deviations of growth may be compared [7]. In a normally developing fetus the TCD increases with advancing gestational age. Several studies demonstrated good correlation between TCD and AC [8]. Many studies have shown that TCD/AC ratio is a stable, gestational age independent parameter after 20 weeks of gestation [9,10]. Increased TCD/AC values are suspicious of fetal growth restriction [3,11] and may be useful in the early detection of fetal IUGR. It can be used to calculate gestational age in IUGR cases with better accuracy [12,13].
Bansal M et al., in their study involving 650 pregnant patients between 14 to 40 weeks, found TCD (mm) equivalent to GA of fetus. The Karl Pearson correlation coefficient between GA & TCD was 0.972305 with p-value of <0.001 (highly significant). Linear relationship of TCD was observed with advancing GA in both normal and IUGR pregnancies [14]. Sharma C et al., conducted a prospective study on 100 normal and 52 IUGR cases where TCD was correlated with other parameters. This revealed significant correlation between TCD and period of gestation with a correlation co efficient of +.9612. In normal pregnancies, GA predicted by all parameters was within normal range. In IUGR pregnancies all parameters including BPD, HC & FL were showing disparity of > 3 weeks except TCD which in both groups were nearer to GA [15].
Benson et al., and Divon WJ et al., in their studies have shown good diagnostic validities for HC/AC ratio in predicting asymmetric IUGR [16,17].
Meyer WJ et al., studied 825 low-risk obstetric patients and 250 patients having risk factors for growth retardation (n = 158) and showed that fetal TCD/AC ratio to be an accurate, gestational age-independent method of identifying the small-for-gestational-age with better diagnostic validity compared to other morphometric ratios including HC/AC and FL/AC ratios [18]. Haller et al., studied 635 well-dated, normal pregnancies and demonstrated a strong correlation between GA determined by LMP and both fetal TCD (r2 = 0.91338) and AC (r2 = 0.89361) in fetuses with birth weights between the 10th and 90th percentiles. In spite of poor correlation of TCD/AC ratio with gestational age (r2 = 0.15788), a slight increase with TCD/AC ratio > 15.5 was present in 80% of SGA infants with increasing gestation [19]. Hill LM et al., conducted a study on 675 women with normal gestations between 14 and 42 weeks and estimated the reference curves for the AC/HC, AC/FL, AC/TCD ratios. The ratios of 34 fetuses with IUGR and 28 macrosomic fetuses to the control group were compared and it was found that, of the three ratios that were investigated, AC/TCD was the most efficacious [20].
Cabbad M et al., in another study with ultrasound examination in patients with suspected IUGR showed that fetal weight was affected to a greater extent than the cerebellar diameter, leading to discordance between TCD and fetal weight, identifying almost all IUGR fetuses with a sensitivity of 95.6% and specificity of 96.3%. In contrast, the HC/AC ratio remained normal in more than 50% foetuses [21]. Chavez MR et al., in a large study of 2597 normal singleton fetuses and 55 IUGR fetuses, found that concordance between the actual and predicted GA (based on published singleton TCD nomogram) was high for IUGR fetuses with the predicted GA within 3 days in 97.5% in the second trimester and 93.3% in the third trimester [22]. Prasad BS et al., conducted a study on 100 pregnant women (80 normal and 20 IUGR pregnancies) between 15 to 40 weeks of gestation and showed that in 17/20 patients the TCD measurements were within the normal range and only in 3 patients it was less than 5th percentile. BPD and FL was less than 5th percentile in 18/20 patients whereas AC, HC measurements were less than 5th percentile in all the 20 patients [23]. Comparison with other studies [Table/Fig-12,13].
Comparison of various parameters of TCD/AC in diagnosing asymmetrical IUGR with other studies
| Authors | Gestational age | Cut-off | Sensitivity | Specificity | PPV | NPV | p- value |
|---|
| Vinkenstein et al., [3] | - | - | 82 | - | - | - | - |
| Campbell et al., [8] | 15-38 | >15.9 | 71 | 77 | 79 | 68 | <0.0001 |
| Dhumale H et al., [10] | 18 – 34 | 13.56±1.21 | - | - | - | - | - |
| Meyer et al., [18] | 14-42 | 13.68±0.96 | 83.9 | 96.2 | 94.5 | 88.2 | <0.0001 |
| Hill et al., [20] | 14-42 | - | 52.9 | - | - | - | - |
| Present study | >20 | >13.63±1.2 | 88 | 93.5 | 77.1 | 96.3 | <0.0001 |
Comparison of various parameters of HC/AC in diagnosing asymmetrical IUGR with other studies.
| Authors | Gestational age | Cut-off | Sensitivity | Specificity | PPV | NPV | p- value |
|---|
| Benson et al., [16] | - | Elevated | 82 | 94 | 62 | 98 | - |
| Divon et al., [17] | 16-40 | >2SD | 36 | 90 | 67 | 72 | - |
| Meyer et al., [18] | 14-42 | >2SD | 49.3 | 87.6 | 75.6 | 69 | <0.0001 |
| Kurjak et al., [24] | 16-40 | >2SD | - | - | 80 | - | - |
| Present study | >20 | >2SD | 84 | 92 | 72.4 | 95.8 | <0.0001 |
Limitations
One of the important limitations in the ultrasound study is dependency on operator for precise measurement. In the present study all measurements were taken by a single operator thus decreasing inter operator variability. With prospective study design, we have decreased the possibility of inherent bias for the radiologist while measuring the fetal biometric parameters. Other technical limitation is the dense shadowing in posterior fossa in third trimester, which may limit adequate visualisation of cerebellum.
Conclusion
Both morphometric ratios – TCD/AC and HC/AC, were gestational age independent parameters and can be used in detecting IUGR with good diagnostic accuracy. However, TCD/AC ratio had a better diagnostic validity and accuracy compared to HC/AC ratio in predicting asymmetric IUGR.
[1]. Hasimito K, Shimizu T, Shimoya K, Kanzaki T, Clapp JF, Murata Y, Fetal cerebellum: US appearance with advancing gestational ageRadiology 2001 221:70-74. [Google Scholar]
[2]. Goel P, Singla M, Ghai R, Jain S, Budhiraja V, Babu CSR, Transverse Cerebellar Diameter: A Marker for Estimation of Gestational AgeJ Anat Soc India 2010 59(2):158-61. [Google Scholar]
[3]. Vinkensteijn AS, Mulder PG, Wladimiroff JW, Fetal transverse cerebellar diameter measurements in normal and reduced fetal growthUltrasound Obstet Gynecol 2000 15(1):47-51. [Google Scholar]
[4]. Galan HL, Pandipati S, Filly RA, Ultrasound evaluation of fetal biometry and normal and abnormal fetal growth. In: Callen PWUltrasonography in obstetrics and gynecology 2008 5th ediPhiladelphiaSaunders:225-66. [Google Scholar]
[5]. Campbell WA, Nardi D, Vintzileos AM, Rodis JF, Turner GW, Egan JFX, Transverse cerebellar diameter/abdominal circumference ratio throughout pregnancy: A gestational age-independent method to assess fetal growthThe Am Coll Obstet Gynecol 1991 77(6):893-97. [Google Scholar]
[6]. Behrman RE, Lees MH, de Peterson EN, Lannoy CW, Seeds AE, Distribution of the circulation in the normal and asphyxiated primateAm J Obstet Gynecol 1970 108:956-96. [Google Scholar]
[7]. Reece EA, Goldstein I, Pilu G, Hobbins JC, Fetal cerebellar growth unaffected by intrauterine growth retardation: a new parameter for prenatal diagnosisAm J Obstet Gynecol 1987 157(3):632-38. [Google Scholar]
[8]. Campbell WA, Vintzileos AM, Rodis JF, Turner GW, Egan JF, Nardi DA, Use of the transverse cerebellar diameter/abdominal circumference ratio in pregnancies at risk for intrauterine growth retardationJ Clin Ultrasound 1994 22:497-502. [Google Scholar]
[9]. Chawanpaiboon S, Kanokpongsakdi S, Vantanasiri C, Predicting Fetal Intrauterine Growth Retardation by Using Reference Centile Charts for the Ratio of Fetal Transverse Cerebellar Diameter to Abdominal Circumference in a Thai PopulationSiriraj Med J 2008 60:316-19. [Google Scholar]
[10]. Dhumale H, Pujar YV, Shravage JC, Bellad MB, Sherigar BY, Durdi GS, Fetal Transcerebellar Diameter to Abdominal Circumference Ratio (TCD/AC) in the Assessment of Normal Fetal GrowthDonald School Journal of Ultrasound in Obstetrics & Gynecology 2010 4(4):448-50. [Google Scholar]
[11]. Khan N, Chaudhri R, Nazir T, Role of Transverse Cerebellar Diameter in Diagnosis of Asymmetrical Fetal Growth RestrictionJournal of Rawalpindi Medical College (JRMC) 2013 17(2):231-33. [Google Scholar]
[12]. Dilmen G, Toppare MF, Turhan NO, Ozturk M, Isik S, Transverse cerebellar diameter and transverse cerebellar diameter/abdominal circumference index for assessing fetal growthFetal Diagn Ther 1996 11(1):50-56. [Google Scholar]
[13]. Singhakom N, Chawanpaiboon S, Titapant V, Reference centile charts for ratio of fetal transverse cerebellar diameter to abdominal circumference in a Thai populationJ Med Assoc Thai 2004 87(3):S54-58. [Google Scholar]
[14]. Bansal M, Bansal A, Jain S, Khare S, Ghai R, A study of Correlation of Transverse Cerebellar Diameter with Gestational Age in the Normal & Growth Restricted Fetuses in Western Uttar PradeshPJSR 2014 7(2):16-21. [Google Scholar]
[15]. Sharma C, Bhardwaj A, Sharma Lines, Kharkwal S, Fetal Transcerebellar diameter measurement for prediction of gestational age: A more dependable parameter even in IUGRInternational Journal of Gynae Plastic Surgery 2014 6(1):13-18. [Google Scholar]
[16]. Benson CB, Belville JS, Lentini JF, Saltzman DH, Doubilet PM, Intrauterine growth retardation: diagnosis based on multiple parameters: a prospective studyRadiology 1990 177:499-502. [Google Scholar]
[17]. Divon MY, Boldes R, Gahan JPM, Assessment of intrauterine growth retardation. In Gahan J P M, Porto MDiagnostic obstetrical ultrasound 1994 2nd edMontanaLippincott Williams and Wilkins:278-91. [Google Scholar]
[18]. Meyer WJ, Gauthier D, Ramakrishnan V, Sipos J, Ultrasonographic detection of abnormal fetal growth with the gestational age-independent, transverse cerebellar diameter/abdominal circumference ratioAm J Obstet Gynecol 1995 171(4):1057-63. [Google Scholar]
[19]. Haller H, Petrovic O, Rukavina B, Fetal transverse cerebellar diameter/abdominal circumference ratio in assessing fetal sizeInternational Journal of Gynaecology and Obstetrics 1995 50(2):159-63. [Google Scholar]
[20]. Hill LM, Guzick D, DiNofrio D, Maloney J, Merolillo C, Nedzesky P, Ratios Between the Abdominal Circumference, Head Circumference, or Femur Length and the Transverse Cerebellar Diameter of the Growth-Retarded and Macrosomic FetusAmer J Perinatol 1994 11(2):144-48. [Google Scholar]
[21]. Cabbad M, Kofinas A, Simon N, King K, Lyttle E, Fetal weight- cerebellar diameter discordance as an indicator of asymmetrical fetal growth impairmentThe Journal of Reproductive Medicine 1992 37(9):794-98. [Google Scholar]
[22]. Chavez MR, Ananth CV, Smulian JC, Vintzileos AM, Fetal transcerebellar diameter measurement for prediction of gestational age at the extremes of fetal growthJ Ultrasound Med 2007 26:1167-71. [Google Scholar]
[23]. Prasad SBS, Likhitha S, Cerebellar Measurements with Ultrasonography in the Evaluation of Fetal AgeIOSR-JDMS 2014 13(9):49-56.Ver. IV: [Google Scholar]
[24]. Kurjak A, Kirkinen P, Latin V, Biometric and dynamic ultrasound assessment of small-for-dates infants: report of 260 casesObstet Gynecol 1980 56:281-84. [Google Scholar]