Falciparum Malaria predominantly contributes to morbidity and mortality associated with malaria. Appropriate drug treatment at early stage and adherence, can significantly reduce mortality in this dangerous condition. National Antimalarial programme of India has recommended artemether and lumefantrine combination (AL) as the drug of first choice for the management of Uncomplicated P Falciparum Malaria for North eastern states. Some studies prove that significant number of patients with Vivax malaria do not complete the medication course [1]. Information, education and communication (IEC) is a vital step to improve drug adherence in many chronic disorders like AIDS [2]. Proper instruction regarding use of ACT and its adherence is essential for better drug action and complete cure of the disease.
Present study was undertaken to evaluate whether well designed drug bags added with verbal information and education, can improve proper ACT adherence in patients of uncomplicated P. Falciparum Malaria.
Materials and Methods
The study was conducted in Medicine and Paediatric Out –Patient Departments (OPDs) of SCB Medical College Hospital, Cuttack and headquarter hospital of Cuttack district.
One hundred fifty two diagnosed patients of Uncomplicated P. Falciparum infection being prescribed with AL were included in the study. The study protocol was approved by Institutional ethics committee of SCB Medical College, Cuttack. Informed consent was obtained from the participants before enrolment into the study. Both paediatric and adult population were included to reach the sample size. Thirty three patients could not be followed up for re-evaluation at 4th day even after telephonic call. Nineteen patients were enrolled as control population who received the ACT combinations but were not given any form of IEC. Information regarding drug adherence, demographic characteristic, socio-economic status, educational background and geographical location of the patients were entered into a predesigned format.
Intervention with IEC
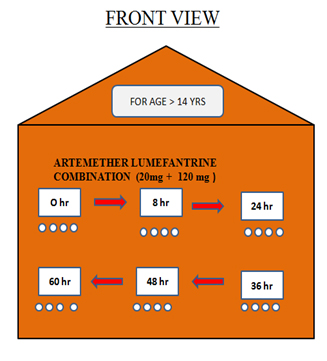
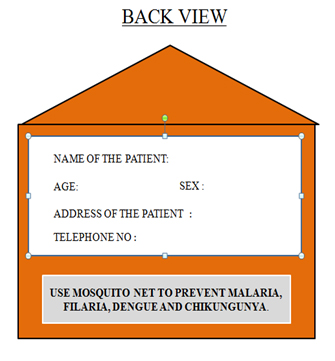
Designed Drug bags made out of hard paper with coloured diagrams to show the number of tablets and time interval of taking the pills served as the primary IEC material for this study [Table/Fig-1]. The fixed structured verbal communication to be given along with the drug bags was also prepared before and was rehearsed before starting this clinical experiment. Verbal communication included information on drug bags, importance of completing the full course of medicine (Artemether+ Lumefantrine), consequence of not taking full course of Antimalarial medicines, importance of taking the medicines at appropriate time interval, importance of taking this medicine along with food, knowledge about the disease (transmission) and preventive measures for malaria.
Four different coloured drug bags were used, three for paediatric age group. Age group (0-3, 3-8,8-14) and other for adults. Both verbal information and drug bags was provided either to patients (> 14 years) or to the accompanied guardian during the first OPD visit after being diagnosed positive for Falciparum Malaria. Patients or guardians were instructed to keep the full course of medicine in the drug bag provided free of cost. Drug bags also highlighted the importance of taking the medicine along with fatty food or milk and using mosquito nets. All the patients were requested to turn up on fourth day to measure drug adherence. The patients those who were not able to turn-up for follow up were interviewed telephonically regarding drug adherence and clinical improvement. The patient was considered adherent when he/she was able to answer the first four questions correctly [Table/Fig-2].
Questionnaire used for evaluating adherence and knowledge
| 1. | How many tablets of your medicine you require for the total cure of your disease? |
| 2. | At what time of the day you are supposed to start the medicine? |
| 3. | What will you do if you miss one dose? |
| 4. | Is it important that you complete the total course even if your fever has subsided? |
| 5. | What are the possible adverse reactions to this drug? |
| 6. | Is there any relation of food to the action of your medicine? If Yes at what time? |
| 7. | What will you do if adverse drug reaction appears? |
Statistical Analysis
The data was expressed as percentage of adherence or non- adherence between the two groups. Data was computed for statistical analysis using Chi-square test and p-value < 0.05 was considered to be significant.
Results
Adherence to ACT was significantly higher in patients receiving IEC compared to control group (81%). Analysis of demographic profile of patients adherent to artemether lumefantrine combinations reveals that 53 out of 61 male patients enrolled in the study were adherent to IEC whereas 28 out of 39 female patients adhered to AL. No significant difference between males or females in terms AL adherence was observed in our study (p > 0.05).
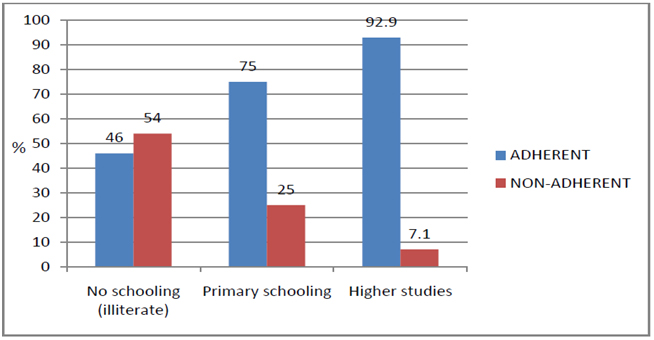
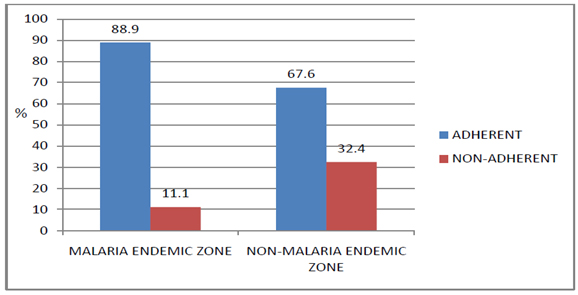
Maximum AL adherence was observed in paediatric age-group between 3-8 years. As the age group of the patients increased from 8-14 or more than 14 years (adults), drug adherence gradually decreased from 90.5% to 84% and 78% respectively. When adherence to IEC was compared between adults and paediatric group, no significant difference was observed (p> 0.05). However, educational status of the patient or accompanying guardians played significant role in terms of AL adherence and was reflected in the form of better drug adherence. Patients or guardians with higher education had significantly better drug adherence compared to no education group (p < 0.05) [Table/Fig-3]. However, no significant difference in terms of drug adherence could be observed between primary schooling and higher studies group. Geographical origin of the patient also was found out to affect AL adherence to a significant extent [Table/Fig-4]. There was no significant correlation between good knowledge about malaria and adherence to ACT.
Impact of educational background of patients on act adherence
Impact of geographical location of patients on act adherence
Discussion
Malaria is one of the most important public health problems in Odisha, reporting approximately 40% of Plasmodium Falciparum Malaria cases and 50% of malaria deaths in the country [3]. The epidemiological pattern of malaria is changing very quickly with high incidence of Falciparum Malaria and increasingly severe presentation of Vivax malaria. Early diagnosis and prompt treatment with effective antimalarials is the only life saving intervention for people affected with malaria. Pharmacological management of malaria is threatened by resistance of Falciparum Malaria to Chloroquine and Sulfadoxine-Pyrimethamine, due to irresponsible use of these medicines. In the recent past, management of Uncomplicated Falciparum Malaria has been changed, with the introduction of ACT. Death rate in cases of moderately severe malaria goes up to 3% compared to less than 1% in uncomplicated P. Falciparum Malaria. Thus these patients need to be treated in appropriate time on an urgent basis. AL should be taken after a fatty meal for better efficacy. Further successful completion of the total dose in appropriate time is very important for successful eradication of parasite because of additional gametocidal action of artemisinin derivatives. Measuring adherence is a very important yet difficult area as techniques used for measuring adherence have many draw backs [4]. Though we have a national guideline for malaria management, patients’ non-adherence to the prescribed therapeutic dose and to treatment schedules pose a serious challenge to effective disease management and increase the risk of resistance. Different studies have proved that non-adherence to drug and its schedule is a very common finding particularly in very busy OPD centres where doctors get very less time to interact with patients [5]. To add the problem, our patients don’t take the medicine properly even if diagnosed and prescribed at right time due to poor socioeconomic condition and lack of proper knowledge and educational background. IEC can empower individuals, family, group and organizations to play active role in achieving and sustaining health [6].
Our study proves that well designed drug bags for keeping medicines when supplemented by verbal communication can improve drug adherence significantly. Our finding goes with similar observation of Anthony A who has shown that, use of different designed drug bags can be a very good tool for proper adherence of medicines as well as improving compliance of medicines in the elderly subjects [7,8]. Some studies done in Thailand, has revealed that use of drug bags can improve adherence to Antimalarial drugs for P. Vivax infection [1].
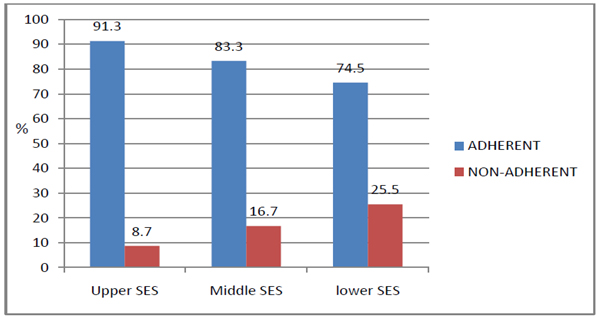
Demographic parameters like age and sex had no significant association with antimalarial adherence in our study. This finding matches with Simsek Z et al., who have observed similar findings [9]. Socio-economic status of the patients was stratified as per Kuppuswamy classification. Our study shows that upper, upper-middle and middle economic groups were more adherent to AL (ranging from 91.3% in upper class to 83.3 in middle class). As the socio-economic conditions went down from upper-lower to lower, Al adherence was decreased to 74.5% [Table/Fig-5].
Impact of socio-economic status of patients on act adherence
In terms of geographical location, when adherence to IEC was analysed, AL adherence in malaria endemic zones was found out to be significantly more compared to non-malaria endemic zones.(p<0.05) Knowledge about, malaria transmission, breeding places, protective methods and signs/symptoms of malaria had no significant correlation with AL adherence. Patient related factors that affected adherence to ACTs were patients’ knowledge on the dosage, efficacy and side effects of the ACTs used for the management of malaria [10,11]. Studies have proved that there exists no significant relationship between adherence and patients’ knowledge on the causes, signs, and symptoms of malaria [12,13]. This study stresses the fact that there is a need for pharmacy staff to stress on these variables when counselling patients on Antimalarials. The strength of our study is that, it looks at other social factors affecting drug adherence for treatment of Falciparum Malaria. Provision of verbal instruction addition to the drug bags is another added factor of this work. However, there may be information biases due to language and interpretation issues.
Conclusion
It’s a challenging task to change human behaviours to increase adherence and to maintain it. Our study proves that IEC can be an excellent tool to overcome this challenge. The study result has given us insights into the social factors associated with adherence to antimalarial drugs and can, thus provide baseline data for planning new strategies to improve adherence to antimalarial medications.