The distal articulating surface of the ulna and radius should be at the same level for optimal function of the radio-carpal, intercarpal and carpo-metacarpal joint complex [1].
Minor modifications in the inferior radio-ulno-carpal complex leads to significant load changes which may result in various pain syndromes [1]. The length of ulna as compared to that of the radius is not constant among individuals during a lifetime [1]. This variation of level of distal articulating surface of ulna with respect to distal articulating surface of radius is known as ulnar variance (UV). It is determined by age, genetics, loading, wrist and elbow pathology [2].
UV affects the forces’ distribution across the wrist, and for this reason it can be an important feature of wrist disorders or wrist pathology, since the percentage of load transmitted through the distal epiphysis of the radius increases with a shorter ulna. The load sharing between radius and ulna in a person with neutral UV is in the ratio of 80:20, which would change significantly with the increase or decrease in values of UV [3]. A negative UV or a short ulna has been shown to have a causative influence in the occurrence of avascular necrosis of the scaphoid, lunate and scapho-lunate dissociations [4–6].
A positive UV, on the other hand, predisposes the wrist to triangular fibrocartilaginous cartilage complex (TFCC) injury [7] and cartilaginous wear of the carpal bones (ulnar impaction syndrome) [8] as well as early degenerative arthritis of the wrist [9].
Measurement of UV requires standardized technique of radiography and a reliable and reproducible method of measurement. Many measurement techniques have been described including method of perpendiculars, concentric circles method and project a line technique [10]. On reviewing the literature it was observed that there is paucity of data on UV and its implications on wrist pathologies in Indian subjects.
The current study has been initiated as a pilot project for evaluation of UV in a regional subset of Indian population. This study has also tried to compare two techniques of measurement of UV viz. method of perpendiculars and modification of the concentric circles method.
Materials and Methods
Ethical approval was sought from Institutional Ethics Committee. The period of the current study was from 1st May 2014 to 30th September 2014. Thirty patients attending the Orthopaedic outpatient clinics, seeking consultation for Orthopaedic ailments related to the elbow, forearm, wrist and hand were included in the study. Informed consent was taken from all subjects.
Adult subjects of either gender aged 18 and above attending the Orthopaedic outpatient clinics with complaints related to the elbow, forearm, wrist and hand and apparently normal wrists were included in the study. Subjects less than 18 years of age, with history of any pathology in the wrist for which he/she was actively taking treatment or had undergone medical or surgical treatment in the past 6 months and those with metabolic bone disease and neuromuscular problems were excluded from the study.
The patients were evaluated with the standard antero-posterior X-ray of the wrist with shoulder in 90o of abduction and elbow in 90o flexion. The X- rays were viewed as DICOM images using radiant viewer. Two methods of measurement were used. The measurements were done using software from GE TEJAS 6000XR.
Measurement using method of perpendiculars: In this method, a line was first drawn along the longitudinal axis of radius. Then, a line was drawn at the apex of the cortical rim of distal ulnar aspect of the radius and another line at the apex of the distal cortical rim of ulna, both of which were perpendicular to the first line. The distance between these two lines were then measured [Table/Fig-1].
Image showing measurement using method of perpendiculars

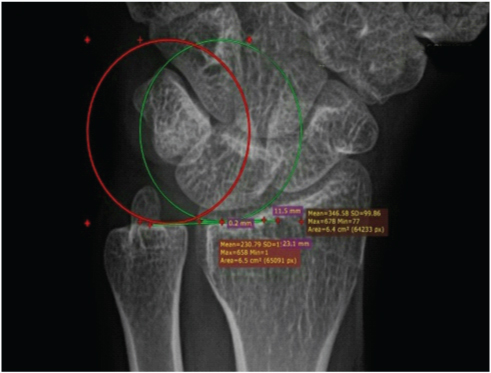
Measurement using modified circle method: In this method, we have drawn two successive circles one touching the concavity of distal radial sclerotic line and other touching the distal cortical rim of the ulnar head. Then the tangential lines were drawn at both of these points and the distance between the two was measured [Table/Fig-2].
Image showing measurement using modified circle method
The measurements using method of perpendicular were labeled as UVA and measurements using modified circle method were labeled as UVB. After the measurements were done, data was recorded and analysed using SPSS version 22.0. Descriptive analysis was done. Paired t-test was used to compare means of UVA with UVB as well as to compare means of UVA and UVB with gender. Pearson correlation coefficient was used to find a correlation of UV with age.
Results
The study population had a mean age of 36 years (18-65 years) [Table/Fig-3]. Fifty three percent were male and forty seven percent were females [Table/Fig-4].
Graph showing age distribution

Diagram showing proportion of males and females
The mean UV using methods of perpendiculars (UVA) was found to be 0.387 mm with a standard deviation of 1.635 (ranging from -3.6 to 3.2 mm). The mean UV using modified circle method (UVB) was found to be 0.507mm with a standard deviation of 1.506 (ranging from -2.9 to 3.1mm) [Table/Fig-5].
Measurement of mean ulnar variance
| N | Minimum | Maximum | Mean | Std. Deviation |
|---|
| Age (in years) | 30 | 18 | 65 | 35.90 | 14.209 |
| UV A (in mm) | 30 | -3.6 | 3.2 | .387 | 1.6349 |
| UVB (in mm) | 30 | -2.9 | 3.1 | .507 | 1.5063 |
| Valid N (list wise) | 30 | | | | |
The mean UV for males using method of perpendiculars was 0.200mm and mean UV using same methods for female was 0.700mm. The mean UV for males using modified circle method was 0.300mm but the mean UV as measured for females using this method was same as that was by method of perpendiculars i.e. 0.700 mm. The two methods of measurements were compared and no statistically significant difference was observed (p-value, 0.250) [Table/Fig-6].
Comparison of ulnar variance by two techniques
| Method of perpendiculars group (n = 30) i.e. UVA | Modified circle method (n=30) i.e. UVB | p-value | Mean difference |
|---|
| Ulnar variance (mm) | 0.387 (1.634) | 0.507 (1.506) | 0.25 | -0.12;95% CI (-0.332, 0.0925) |
As the mean age of patients in the current study was 36 years, the study group was sub-divided as subjects < 36y (group 1) and subjects > or = 36y (group 2). Using methods of perpendiculars, the mean UV was found to be 0.04 in group 1 and 0.730 for group 2. Using the modified circle method, the mean UV in group 1 was 0.170 and in group 2 was 0.840.
There was no statistically significant correlation between UV and age by either methods i.e. method of perpendiculars (p-value, 0.905) and modified circle method (p-value, 0.960) [Table/Fig-7].
Correlation between Age (age =35.9) and UVA and UV B
| Mean ulnar variance | r | p-value |
|---|
| UV A | 0.387 (1.634) | 0.023 | 0.905 |
| UV B | 0.507 (1.506) | -0.009 | 0.960 |
The mean UV measured by either method with respect to the gender of the subjects also did not show any statistically significant difference: UVA (p-value, 0.406) and UVB (p-value, 0.352) [Table/Fig-8].
Comparison of ulnar variance according to sex by methods of perpendiculars Note: Figures expressed are mean and standard deviation, CI= Confidence interval
| Ulnar variance (mm) | Male (n=16) | Female (n=14) | p-value | Mean difference |
|---|
| UV A | 0.657 (1.444) | 0.150 (1.797) | 0.406 | 0.50795%CI (-0.724, 1.738) |
| UV B | 0.263 (1.577) | 0.786 (1.425) | 0.352 | 0.53295%CI (-0.608, 1.654) |
Discussion
Measurement of ‘Ulnar Variance’ requires a standardized technique of radiography and a reliable and reproducible measurement technique. Many methods of measurement have been described in various literatures namely project a line technique, method of perpendiculars and Palmer’s concentric circle method [10].
In the present study, two methods of measurement, namely methods of perpendiculars and modified circle method, were used to measure UV. The sample size was 30. Sixteen were male and 14 were female. Various studies in the literature have used various sample sizes. Ando et al., [11] studied 20 wrists while Goldfarb et al., [12] evaluated 138 wrists in his study evaluated 38 wrists in his study.
The mean age in the current study was 36 years. The mean ulnar variance in this regional subset of patients using method of perpendiculars was 0.387 mm and using modified circle method was 0.507mm. Different authors have reported different values depending on type of population and associated pathology studied [Table/Fig-9].
Mean ulnar variance reported by various authors
| Author | Year | Number (N) | Mean UV |
|---|
| Chan [13] | 1980 | 400 | 0.830 |
| Czitrom [14] | 1987 | 65 | -0.380 |
| Nakamura [15] | 1991 | 325 | 0.200 |
In the study on Malaysian population by Chan et al., the ulnar variance averaged – 0.100 ± 1.310mm. Out of the population studied, 38% of patients had neutral variance, 29% had negative variance while 33% of patients had positive UV [16].
The present study observed a higher prevalence of positive ulnar variance as compared to negative UV in the population studied. Schuurman et al., [17] in their study on Dutch patients also documented a higher predominance of positive UV. However, Elsaftawy [18] in his study on 196 cases observed a positive ulnar variance in 44 patients (17%), negative variance in 63 (24%) subjects and neutral ulnar variance accounted for the biggest group of other 158 (60%) patients. He also concluded that there was no correlation between gender and UV in his study.
No statistically significant difference was observed between age and gender with respect to UV in the current study. However researchers have documented a statistically significant difference in UV between males and females. Bonzar M [19] observed that UV decreased significantly with increasing age and showed that gender did not influence UV. However, Nakamura [15] reported a significant difference in gender and a positive correlation between UV and age in normal wrists.
An exhaustive literature search revealed that there is no standard method for measurement of UV and researchers modified the available methods from time to time in search for a more accurate method. In the present study a modified circle method was used, as we observed that there is no fixed reference point of measurement in the concentric circle method described by Palmer [20]. The reference point keeps changing depending on positive and negative UV as circles of different radii of curvature need to be used as reference circles for measurements involving a positive, neutral or a negative UV in the method described by Palmer and colleagues. We used the same landmarks that were used in concentric circle method but instead of using concentric circles we used successive/overlapping circles so that the radii of curvature of the reference circles and thereby the point of reference remains the same.
The basic implication of this study was the association of UV with various wrist pathologies. A negative UV (ulna projects more proximally) or a short ulna has been shown to have a causative influence in Kienbock’s disease, avascular necrosis of the scaphoid as well as in scapho-lunate dissociations [4–6]. A positive UV (ulna projects more distally), on the other hand, predisposes the wrist to triangular fibrocartilaginous cartilage complex (TFCC) injury and cartilaginous wear of the carpal bones (ulnar impaction syndrome) as well as early degenerative arthritis of the wrist [7,8]. In 1990, Boulas and Milek [7] showed the use of ulnar shortening to relieve ulnolunate impingement in patients with ulnar positive or neutral wrists. In 2005, Tomaino and Elfar [8] suggested that static or dynamic UV is likely to play a role in ulnar impaction syndrome. The above researchers opined that there is a definite role of positive UV as a predisposing factor in triangular fibrocartilaginous complex tears and ulnar impaction syndrome. As the present study is a pilot study with a short follow up the clinical implications of the UV cannot be commented upon and a longer term clinical study is required.
Limitations
There were certain limitations in the current study. The number of subjects was only 30; probably a larger number of subjects would be needed to conclude the relationship between various parameters observed. Our study employed only two methods of measurement. Many other measurement techniques can be used to see the suitability and reliability of each technique.
The measurements were done by only one observer and the software used may also have some inherent errors; to reduce this, we could have used multiple observers which would have increased the reliability of the study as has been shown by other authors. Steyers and Blair [10] have used three observers and each observer measured the UV three times and the inter-observer and intra-observer reliability was seen. All data was measured manually. Another limitation of the present study was that measurement of UV was done in standard neutral position of the wrist but studies have shown that wrist position and grip may have a role in the measurement of UV [18].
Conclusion
In the regional subset of Indian population studied, there is a higher incidence of positive ulnar variance as compared to negative ulnar variance and there is no correlation between ulnar variance with respect to age and gender of the subjects. However, a larger sample size with a longer follow up is required to suggest a correlation of ulnar variance with clinically symptomatic disease.