Ectopic Spleen Presenting as Lump Abdomen: A Rare Case Report and Review of Literature
Bapurapu Rajaram1, Madipeddi Venkanna2, Dodda Ramesh Kumar3, Boda Kumaraswamy4, Bachannagari Srinivas Reddy5
1 Associate Professor, Department of General Surgery, Kakatiya Medical College/ Mahatma Gandhi Memorial Hospital, Warangal, Telangana, India.
2 Assistant Professor, Department of General Surgery, Kakatiya Medical College/ Mahatma Gandhi Memorial Hospital, Warangal, Telangana, India.
3 Professor, Department of General Surgery, Kakatiya Medical College/ Mahatma Gandhi Memorial Hospital, Warangal, Telangana, India.
4 Assistant Professor, Department of General Surgery, Kakatiya Medical College/ Mahatma Gandhi Memorial Hospital, Warangal, Telangana, India.
5 Junior Resident, Department of General Surgery, Kakatiya Medical College/ Mahatma Gandhi Memorial Hospital, Warangal, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. B. Rajaram, 2-2-23/B2, Heritage Residency, Behind Rang Restaurant, Nayeem Nagar, Vidyaranyapuri, Hanamkonda, Warangal, Telangana - 506001, India. E-mail : paulrajaram@yahoo.com
Ectopic spleen is due to failure of fusion of the mesogastrium and the lining body wall epithelium, resulting in lax or absent supporting ligaments of spleen, making it abnormally mobile. This case presented as lump abdomen with history of recurrent attacks of abdominal pain. Clinical diagnosis was unidentified abdominal mass. The radiological imaging was suggestive of the diagnosis, and the exploration of abdomen has clinched the diagnosis.
Mobile spleen, Torsion of spleen, Unidentified abdominal mass
Case Report
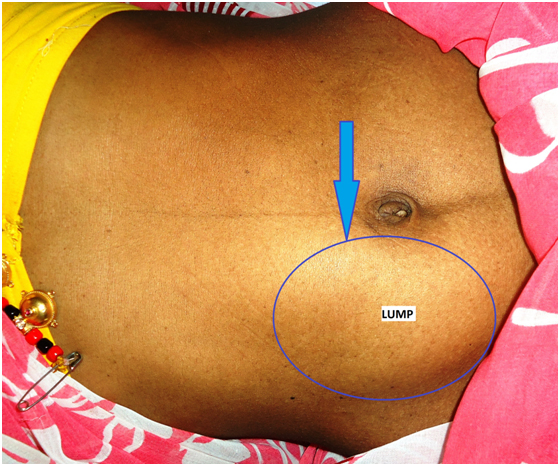
A 24-year-old woman presented to the out-patient Department of General Surgery, Kakatiya Medical College/Mahatma Gandhi Memorial Hospital, Warangal, Telangana state, India with complaint of lump abdomen and chronic intermittent pain abdomen. On physical examination, her vital signs were within normal limits. There was no history of bowel or urinary symptoms. Patient underwent two times caesarean section. Examination of the abdomen revealed a freely mobile intra abdominal mass in right lumbar, right iliac fossa and umbilical regions [Table/Fig-1].
Clinical photograph demonstrating lump in right lumbar, umbilical and right iliac fossa regions,
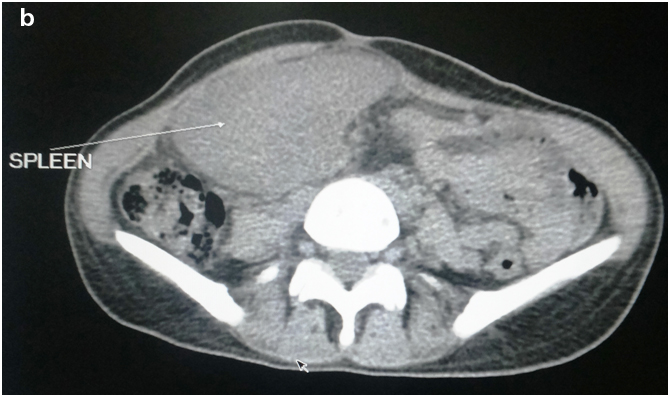
On abdominal ultrasonography (USG), the spleen was not found to be in its normal anatomic position, and bowel loops were observed in the left upper quadrant of the abdomen with normal position of kidneys and ovaries. An enlarged spleen extending to the pelvis from right lumbar region with large hypoechoic area was noted. No blood flow in the splenic artery and vein was observed on Doppler USG. On abdominal intravenous contrast-enhanced computed tomography (CT) scan, the spleen was not seen in its normal anatomic position, but rather was located in right lumbar region, extending to the right adnexal region. The splenic parenchyma showed a non-homogeneous enhancing area suggestive of infarction [Table/Fig-2a,b]. Complete blood picture was normal.
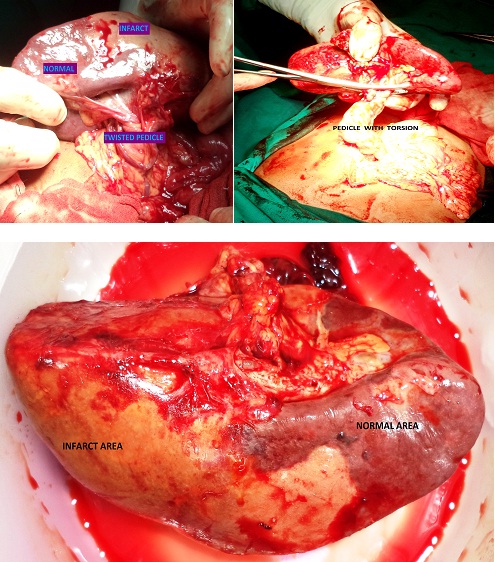
Based on physical examination USG and CT findings, a laparotomy through a midline vertical incision was performed. It was intraoperatively noted that the spleen lacked its normal ligamentous attachments and was suspended only by an elongated vascular pedicle in right lumbar, umbilical and right iliac fossa regions with adhesions to liver and bowel loops. The pedicle of spleen was twisted two times (720 degrees). There was mild free fluid in abdomen; the left hypochondrium was filled with bowel loops. Adhesions were released, spleen was derotated. The surface of the spleen has shown clear infarcted area even after derotation. Hence splenectomy was done [Table/Fig-3]. The postoperative course was uneventful. Patient was given vaccines. Patient was discharged after recovery.
Coronal and sagittal sections of computed axial tomography scan showing spleen in right lumbar, right iliac fossa, umbilical regions with non enhancing areas suggestive of infarction

Axial computed tomography scan showing an ectopic spleen (S) in right lumbar region and umbilical regions
Intraoperative findings of torsion and infarction of spleen
Discussion
Ectopic spleen is a rare entity. The incidence of torsion is estimated to be less than 0.2% [1]. Incidence is higher among multiparous woman [2]. Most cases are diagnosed in adults aged between 20 to 40 years [2]. So far, about 500 cases have been reported [1].
The clinical presentation of an ectopic spleen is variable. Affected patients may be asymptomatic and this condition may be incidentally discovered on physical examination, or on imaging studies performed for other unrelated reasons, as an abdominal or pelvic mass that may or may not be accompanied by gastrointestinal or urinary symptoms [3–5]. Differential diagnosis includes adenopathy, lymphoma, extramedullary haematopoeisis. The patient may become symptomatic due to abnormal mobility, torsion and compromised blood supply. Patients may have mild, intermittent abdominal pain due to splenic congestion with intermittent torsion and spontaneous derotation, as well as splenomegaly as a result of vascular congestion [4,5]. Patients may present with an acute abdomen due to torsion of the splenic pedicle with subsequent infarction [2]. Differential diagnosis includes acute appendicitis, ovarian torsion, cholecystitis. The splenic torsion is sometimes associated with gastric or pancreatic tail volvulus. The intestinal obstruction by splenic flexure volvulus is the only colonic manifestation reported [6]. In the present case, patient presented with lump abdomen associated with chronic intermittent pain abdomen.
In general, laboratory tests are usually non-specific; however, they may occasionally reveal pancytopenia as evidence of hypersplenism or functional asplenia, by evaluating peripheral smear for Howell-Jolly bodies or other particles [4]. In the present case complete blood picture was normal.
To detect a suspected ectopic spleen with torsion, various diagnostic modalities can be used: Technitium–99m sulphur colloid scintigraphy, Ultrasonography, Doppler ultrasonography, CT scans, CT angiography and MRI [3–5]. In present case Ultrasonography, Doppler ultrasonography and CECT Abdomen were performed to diagnose the condition.
Historically, splenectomy has been the treatment for symptomatic ectopic spleen [4]. Now the treatment is splenopexy or splenectomy depending on the viability of the spleen. Preservation of the spleen by different surgical techniques has been the focus of modern therapeutic concepts for the treatment of ectopic spleen [3,7]. In present case splenectomy was done because of infarction. Most authors now support the use of splenectomy if there is torsion, splenic vein thrombosis, splenic infarction and hypersplenism. Conversely, splenopexy is preferred when a viable ectopic spleen is found at laparotomy [3]. Splenopexy by means of the extraperitoneal pocket creation appears to allow anatomic placement of the spleen along with the protection of the rib cage without the employment of biomaterials [6]. Presently, splenic surgery by laparoscopic approach is an extensively used and a preferred technique because it is less painful and allows for better cosmesis, early ambulation, overall less morbidity, and a faster return to work. The methods include creating a pouch in the omentum, stomach, or colon and the use of absorbable mesh to fix the spleen in its normal anatomical location [8].
Conclusion
Ectopic spleen, with or without torsion is a rare clinical entity. Imaging modalities play an important role in the diagnosis. Early diagnosis and treatment of an ectopic spleen may reduce the frequency of splenectomy. Therefore, if there is no spleen at the normal anatomic location by imaging studies, one should consider the possibility of an ectopic spleen in patients who present with palpable abdominal mass, with or without pain abdomen.
[1]. Sharma A, Salerno G, A torted wandering spleen: a case reportJ Med Case Rep 2014 8:133 [Google Scholar]
[2]. Maksoud SF, Swamy N, Khater NH, Tale of a wandering spleen: 180 degree torsion with infracted spleen and secondary involvement of liverJ Radiol Case Rep 2014 8(6):18-26. [Google Scholar]
[3]. Cho SA, Choh NA, Dar I, Jehangir M, Yousuf R, Wandering spleen presenting as recurrent abdominal pain in a young femaleIndian J Pediatr 2008 75(11):1182 [Google Scholar]
[4]. Feroci F, Miranda E, Moraldi L, Moretti R, The torsion of a wandering pelvic spleen: a case reportCases J 2008 1(1):149 [Google Scholar]
[5]. Misawa T, Yoshida K, Shiba H, Kobayashi S, Yanaga K, Wandering spleen with chronic torsionAm J Surg 2008 195(4):504-05. [Google Scholar]
[6]. El Bouhaddouti H, Lamrani J, Louchi A, El Yousfi M, Aqodad N, Ibrahimi A, Torsion of a wandering spleenSaudi J Gastroenterol 2010 16(4):288-91. [Google Scholar]
[7]. Soleimani M, Mehrabi A, Kashfi A, Fonouni H, Buchler MW, Kraus TW, Surgical treatment of patient with wandering spleen: report of six cases with a review of the literatureSurg Today 2007 37(3):261-69. [Google Scholar]
[8]. Faridi MS, Kumar A, Inam L, Shahid R, Wandering spleen- a diagnostic challenge: case report and review of literatureMalays J Med Sci 2014 21(6):57-60. [Google Scholar]