Pleomorphic Adenoma in Subcutaneous Plane of the Neck: A Rare Entity
Bharat Kamath1, Pooja Kamath2, Prasad Bhukebag3
1 Assistant Professor, Department of Surgery, Seth V.C. Gandhi & M.A. Vora Municipal General Hospital, Rajawadi, Ghatkopar (E), Mumbai, India.
2 Associate Professor, Department of Oral Pathology & Microbiology, D.Y. Patil Dental College & Hospital, Sector 7, Nerul, Navi Mumbai, India.
3 Consultant Surgeon, Hira Mongi Navneet Hospital, Valji Ladha Road, Mulund(W), Mumbai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pooja Kamath, 301, La-Belle, St Anthony’s street, Vakola, Santacruz(East), Mumbai-400055, India. E-mail : poojabhat82@gmail.com
Heterotopic Salivary Gland Tissue (HSGT) is salivary tissue found in locations not normally host to it. Neoplasms occurring in these heterotopic tissues are very rare. Review of literature has revealed the neck to be host to HSGT and rarely, tumourigenic changes in these inclusions have been observed.
We present a clinically unsuspected case of an ectopic pleomorphic adenoma of lower neck in which the ectopic salivary tissue was found in subcutaneous plane, which to the best of our knowledge has not been reported and was proved only on cytology and histopathology. There is a probability of this tumour undergoing malignant transformation. Therefore, these tumours need to be promptly diagnosed, adequately treated and should be included in the differential diagnosis of neck masses.
Ectopic pleomorphic adenoma, Heterotopic salivary gland tissue, Neck mass, Salivary gland tumour
Case Report
A 39-year-old male presented with a painless swelling on right side of the lower neck, at the anterolateral border of sternocleidomastoid muscle leading to an unaesthetic appearance. The swelling was present since birth, initially innocuous and gradually increasing to the present size of 4x2x2 cm; was firm, partly fixed to the skin but movable on deeper structures. There were no other symptoms or relevant medical history.
Ultrasonographic examination of the neck showed a 4x2 cm heterogenous lesion in the right paratracheal region of the neck in the subcutaneous plane [Table/Fig-1], with normal vascularity on Doppler colour scan. Fine needle aspiration cytology was done with reported suspicion of a salivary gland tumour [Table/Fig-2].
Ultrasonographic image of heterogenous well circumscribed lesion in the subcutaneous tissue (arrow)

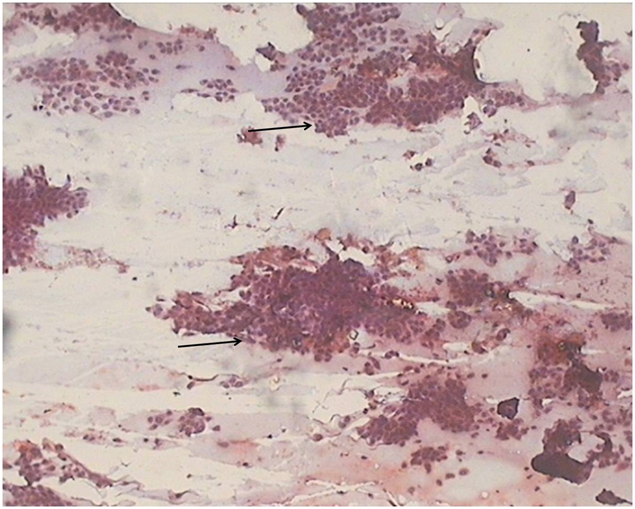
Photomicrograph shows FNAC smear showing cohesive clusters of ductal cells (arrow) (MGG stain X100)
The lesion was excised with safety margins under general anaesthesia. It was subcutaneous, superficial to the cervical fascia and was excised completely with adequate margins.Grossly, the specimen was well circumscribed, measuring 5x2x2 cm and had a shiny, white and myxoid cut surface.
Histopathology revealed an encapsulated lesion comprising of epithelial and connective tissue components [Table/Fig-3]. Epithelial cells were arranged in the form of nests, cords and strands. Multiple ductal areas enclosing mucoid material were seen [Table/Fig-4]. The connective tissue was myxo-chondroid [Table/Fig-5]. The features were clearly suggestive of a benign mixed tumour of ectopic salivary tissue origin.
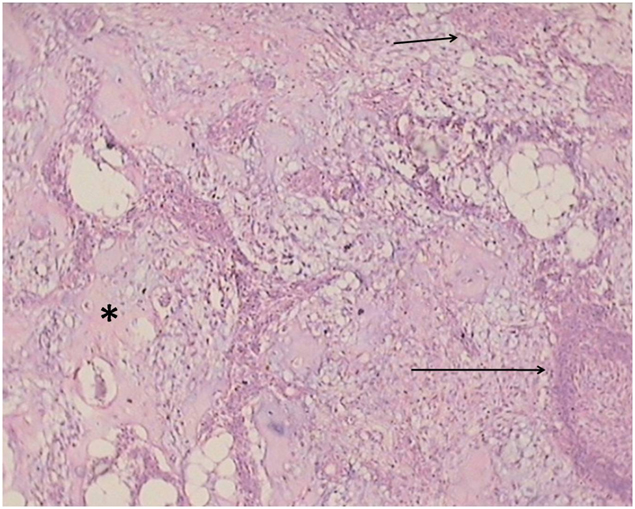
Photomicrograph shows an encapsulated tumour mass (asterix) with tumour cells arranged as ducts (short arrow) and chords (long arrow) (H&E stain X100)

Photomicrograph shows small nests (short arrow) and strands of tumour cells (long arrow) interspersed in a chondro-myxoidstroma (asterix) (H&E stain X100)
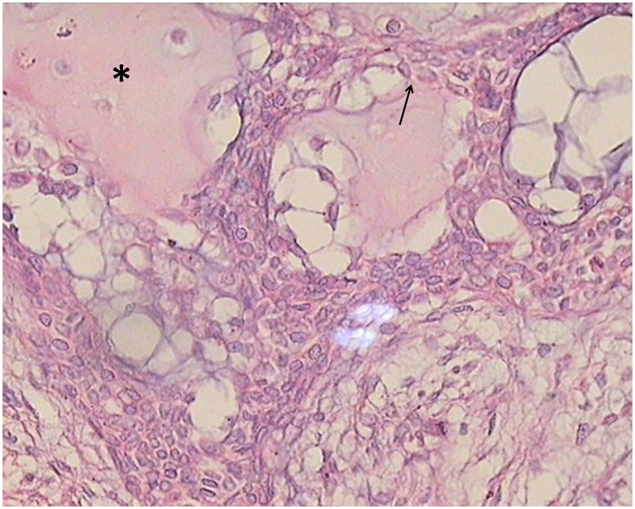
Photomicrograph shows chords of tumour cells (arrow) in chondro-myxoidstroma (asterix). (H&E stain X400)
The patient has been followed up over a period of one and half years, with no recurrence or any symptoms.
Discussion
Heterotopic salivary gland tissue (HSGT) is an architecturally normal arrangement of salivary tissue found in locations external to major and minor salivary glands [1]. The occurrence of HSGT in the neck is rare, mostly found in deeper tissue planes and it may manifest as a mass, cyst or a draining sinus [2]. Heterotopias have been described in lymph nodes, external auditory canal, hypophysis, mandible, mastoid bone, middle ear, tongue, sternoclavicular joint, thyroid and parathyroid glands and in upper and lower neck regions [2].
Embryogenesis of HSGT is not clear and is related to the anatomic site. Normally, migration of parotid and submandibular glands is limited to the region of the mandible and therefore cannot account for appearance of salivary tissue in the lower neck. The location of heterotopic salivary gland elements in the lower neck, suggests a relationship to the branchial apparatus, particularly the precervical sinus. In the 6th week embryo, growth of the 1st and 2nd branchial arches exceeds and encloses 3rd and 4th arch in an ectodermal pouch, thus forming a sinus. The sinus is normally obliterated by the end of 2nd month, failure of which leaves cystic vestiges in the neck. These ectoderm derived cysts are postulated to be capable of giving rise to salivary tissue [3,4].
Neoplasms arising from HSGT are uncommon with a histologic picture similar to that of lesions arising from normal salivary tissue [5]. Review of previous literature has suggested that heterotopic salivary tissue neoplasms found in the neck were often seen in the upper neck and Warthins tumour was the most common benign neoplasm followed by Pleomorphic Adenoma [2]. Pleomorphic adenoma is the most common neoplasm affecting parotid gland and accounts for 40 to 70 percent of minor salivary gland tumours. Occasionally, pleomorphic adenoma may arise from salivary glands in unusual locations [6]. Pleomorphic adenomas occurring in HSGT present in deeper tissue planes of the upper neck and around the anterior border of sternocleidomastoid muscle have been reported [7,8], but its occurrence in the lower neck and that too in the subcutaneous plane as in our case is extremely rare and makes it noteworthy. The distinctive location of Pleomorphic Adenoma in this case could be accounted for by one of the explanations given by Willis in 1968. Willis proposed 3 main hypotheses to explain this kind of heterotopias. These were: an abnormal persistence and development of vestigial structures; dislocation of portion of a definitive rudiment during mass movement and development; and abnormal differentiation of the local tissues (heteroplasia) [2].
Treatment modality for pleomorphic adenoma is resection with tumour free margins. Inspite of being a benign neoplasm, inadequate management of pleomorphic adenoma may lead to problems like local recurrence and malignant transformation into Carcinoma Ex-Pleomorphic Adenoma (CEPA) or carcinosarcoma [9], and even more rarely metastasizing pleomorphic adenoma may occur [10].
Thus ectopic appearance of salivary tissue in an unusual location can pose a diagnostic dilemma to the surgeons and a thorough pathologic diagnosis is essential. The nature of the lesion needs to be ascertained and if benign it should be promptly and adequately eliminated. Detection of malignancy warrants a thorough investigation to validate whether it is a primary tumour in ectopic site or metastasis from a primary tumour of the normal salivary glands followed with neck dissection and subsequent radiotherapy.
Conclusion
Neck is prone to a multitude of swellings with a varied differential diagnosis. Rarely a tumour of apparent salivary gland origin may be seen in the neck. Our case is a reiteration of previous reports, that tumour of heterotopic salivary gland tissue should be included in the differential diagnosis of neck swellings. A thorough pathologic confirmation is required. Detection of a malignant tumour demands investigations followed with appropriate treatment.
[1]. Singer MI, Applebaum EL, Loy KD, Heterotopic salivary tissue in the neckThe Laryngoscope 1979 89:1772-77. [Google Scholar]
[2]. Daniel E, McGuirt WF, Neck masses secondary to heterotopic salivary gland tissue: a 25 year experienceAmerican Journal of Otolaryngology 2005 26:96-100. [Google Scholar]
[3]. Ferlito A, Bertino G, Rinaldo A, Mannara GM, Devaney KO, A review of heterotopia and associated salivary gland neoplasms of the head and neckThe Journal of Laryngology and Otology 1999 113:299-303. [Google Scholar]
[4]. Youngs A, Scofield H, Heterotopic Salivary Gland Tissue in the lower neckArch Pathol 1967 83:550-56. [Google Scholar]
[5]. Pesavento G, Ferlito A, Benign mixed tumour of heterotopic salivary gland tissue in upper neck. Report of a case with a review of the literature on heterotopic salivary gland tissueJ LaryngolOtol 1976 90:577-84. [Google Scholar]
[6]. Ellis GL, Auclair PL, Gnepp DR, Surgical pathology of the salivary glands 1991 PhiladelphiaW B Saunders:14:15:166:167 [Google Scholar]
[7]. Testa D, Staibano S, Guerra G, Mascolo M, Galera F, Iovine R, Pleomorphic adenoma in ectopic salivary tissue of the neckThe Open Otorhinolaryngology Journal 2008 2:13-5. [Google Scholar]
[8]. Arunkumar KV, Kumar S, Bansal V, Saxena S, Elhence P, Pleomorphic adenoma – unusual presentation of a salivary gland tumour in the neck of a childQuintessence International 2011 42(10):879-82. [Google Scholar]
[9]. Papadogeorgakis N, Kalfarentzos EF, Petsinis V, Parara E, Kopaka ME, Multinodular neck recurrence of parotid gland pleomorphic adenoma: a case reportOral Maxillofac Surg 2012 16(1):137-40. [Google Scholar]
[10]. Santaliz-Ruiz LE, Morales G, Santini H, Sánchez-Santiago M, Arroyo A, Metastasising pleomorphic adenoma: a fascinating enigmaCase Rep Med 2012 doi: 10.1155/2012/148103 [Google Scholar]