A Rare Combination of Avulsion Fractures Around the Knee –A Case Report
Deepak Sampath1, Hanumantha Reddy2, Chirag Thonse3, Jayanth Kumar Bangalore Chikkanna4
1 Consultant, Department of Orthopaedic, St Martha’s Hospital, No. 5, Nrupathunga Road, Bangalore, Karnataka, India.
2 Resident, Department of Orthopaedic, St Martha’s Hospital, No. 5, Nrupathunga Road, Bangalore, Karnataka, India.
3 Consultant, Department of Orthopaedic, St Martha’s Hospital, No. 5, Nrupathunga Road, Bangalore, Karnataka, India.
4 Senior Consultant and Unit Chief, Department of Orthopaedic, St Martha’s Hospital, No. 5, Nrupathunga Road, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepak Sampath, No 139, 2B Cross, Ombr Layout, Banaswadi, Bangalore-560043, Karnataka, India. E-mail : drdeepuortho@gmail.com
Patella fractures, tibial spine avulsion and Segond fractures are mainly due to trauma to the knee which may be direct or indirect injuries. While each entity is well documented when occurring in isolation, but bilateral inferior pole patella fracture, tibial spine avulsion in the right knee and bilateral segond fracture in a same patient is a rare occurrence. We report a case of 24-year-old male with such an injury. The diagnosis was confirmed by X-ray, CT scan and MRI imaging of right knee. Then the patient was treated with arthroscopic anterior cruciate ligament (ACL) avulsion fixation with pull through technique and suture disc; bilateral inferior pole patella was treated conservatively with knee brace, segond fracture was treated conservatively similarly. To the best of our knowledge, this is the rare case in the medical literature with all these injuries occurring simultaneously.
Bilateral patella fracture, Segond fracture, Tibial spine avulsion
Case Report
A 24-year-old male presented to Department of Orthopaedics St. Martha’s hospital with a history of sustained injury to both his knees. While unloading heavy stone bars from a vehicle, the object fell on legs from behind forcing the both knee joints into flexion and external rotation, followed by hitting of his both knees to the wall in front of him. In emergency room, clinical examination revealed a marked effusion in knees, crepitus and tenderness over inferior pole patella on both sides. Lachman test was positive (grade 2) on right side and it was negative on left side, varus and valgus stress test was negative on both sides. Active extension of both legs was present. X-ray imaging of both knees showed a bilateral inferior pole of patella fracture with minimal displacement, bilateral small bony avulsion on the AP view which is elliptical in outline near the lateral tibial condylar articular margin suggested Segond fracture and tibial spine avulsion on right knee [Table/Fig-1,b&2a,b]. MR imaging [Table/Fig-3] and CT scan [Table/Fig-4] confirmed the ACL on right knee with avulsion fracture of patella with contusion of lateral tibial condyle. Further imaging of right knee was not undertaken as there was no clinical instability. Examination under anaesthesia revealed bilateral pivot shift test positive co-relating our radiological findings of bilateral ALL avulsion. Patient was treated by arthroscopic right ACL avulsion fixation with pull through technique over suture disc. Bilateral patella inferior pole fracture was treated conservatively with knee brace since the extensor mechanism was intact. Segonds fracture was treated conservatively with brace.
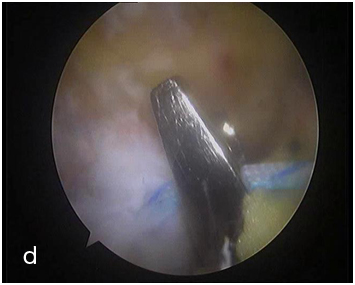
Surgical technique: Diagnostic arthroscopy was carried out to assess additional injuries like meniscal injury, chondral injury and other ligament tears. Fracture crater was adequately cleaned. Two drill holes were made with 2.7 mm guide wire with the help of ACL jig, medial and lateral to ACL and exiting out on medial tibial cortex. With the Arthroscope in lateral portal, 90 degree suture lasso was passed through medial portal and through the posterior half of ACL substance close to fragment and the suture loop retrieved through lateral portal. A ETHIBOND (no. 2) was passed through the loop and taken out through medial portal. This step was repeated in a similar manner through anterior half of substance of ACL [Table/Fig-5a,b,c,d, and e].
X-ray right knee showing Segond fracture

Plain x-ray left knee Segond fracture and ACL avulsion

X-ray lateral view of right knee showing lower pole patella fracture

X-ray lateral view of left knee showing lower pole patella fracture

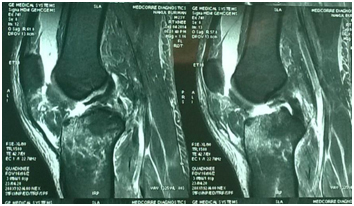
MRI of right knee showing ACL avulsion from tibial attachment
CT scan cut section of right knee showing segond fracture with tibial spine avulsion

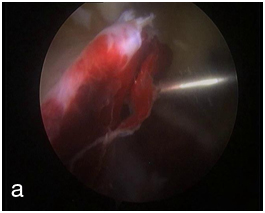
Intraoperative image showing ACL avulsion
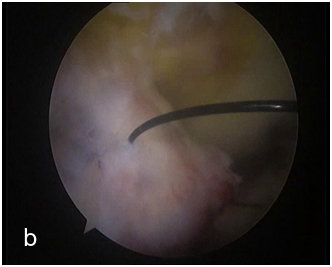
Arthroscopic image showing taking bite through the substance of ACL
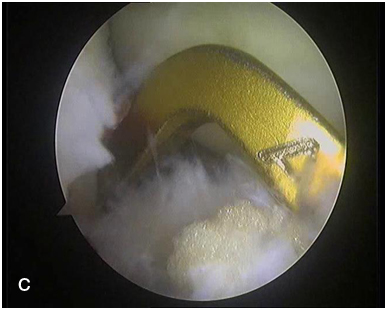
Intraoperative image showing usage of ACL Jig for tibial tunnel
Intraoperative image showing retrieval of suture through tibial tunnel with the help of suture retriever
Intraoperative image showing taught ACL without laxity after fixation
Spinal needle no 16 was passed through medial tibial drill hole. Once epidural needle was seen in the joint, ethilon loop (no.1) was passed through the needle for suture shuttle. Ethilon loop was retrieved through the medial portal. Both the ethibond sutures were passed through the ethilon loop outside the joint and then pulled out after holding lateral end of the suture with the haemostat. Both ethibond medial sutures were shuttled through the medial tibial tunnel. This step was repeated for lateral sutures and retrived through lateral tibial tunnel. Both ends of ethibond were held under traction and reduction was assesed. In full extension, roof impingement was checked. Then sutures were tied over suture disc in extension.
Patient was followed up at regular intervals with check x-rays at 3 weeks, 6 weeks and 12 weeks. Patient was put on sequential weight bearing on right side with a graduated knee bending programme and static exercises of knee.
On follow up at 6 weeks, both patella fracture and tibial spine fractures was uniting [Table/Fig-6] and ranges of movements attained such as – right knee 5-60o [Table/Fig-7] and left knee 0-120o. Full weight bearing mobilization was started after 6 weeks on left side, and at 8 weeks on right side. Lachman test was negative on right side. At 12 weeks follow up, the patient attained full range of movement of both knees, with good quadriceps strength. Radiographs revealed union of patella, tibial spine and segond on the right side and patella and segond on the left side. Patient at 1 year follow up had full range of movements and no instability [Table/Fig-8,9].
At 6 weeks follow up showing suture disc in place with union of both patella fractures

Clinical photograph showing right knee flexion of around 60 degrees

Clinical photograph showing right knee full extension at 6 weeks

Clinical photograph of left knee showing full range of motion at 6 weeks follow up

Discussion
Patella is the largest sesamoid bone of the body and lies within the fascia lata and the fibers of the quadriceps tendon. The most significance of patella fracture is loss of continuity of extensor mechanism and potential incongruity of the patello-femoral articulation [1]. Bilateral patellae fractures resulting from traumatic aetiology are very rare injuries. In most cases found in the scientific literature, they are described as stress fractures or as complications of chronic diseases such as osteoporosis, renal failure and secondary hyperparathyroidism. Pole fractures may indicate a significant disruption of the extensor mechanism. Distal pole fractures are bony avulsions of the origin of patellar tendon. Non operative treatment is indicated for fragment separation of less than 3mm and articular step-off of less than 2mm with intact extensor mechanism.
Segond fracture on conventional radiographs appears as tiny bony fragment elliptical in outline near lateral tibial condylar articular margin mainly visible on ap view. The relatively benign appearance of these small fragments may lead to potentially more severe underlying damage to the major stabilizing structures of the joint [2].
Segond fracture is an avulsion fracture of lateral tibial condyle at the middle third of the lateral capsular ligaments described by Paul Segond in 1879 [3]. Campos et al., described that fibers of the iliotibial tract and anterior oblique ligament of the fibular collateral ligament are the structure involved in pathogenesis of the segond fracture [4].
Recently Dodds et al., dissected 40 fresh frozen cadavers and found a consistent structure in the antero lateral compartment of the knee and named it as anterolateral ligament (ALL) which is the ligament avulsion associated with Segond fracture [5].
Numerous studies have demonstrated an association of the Segond fracture with tears of ACL (75%-100%), meniscal tears (66%-75%), damage to the structures of the posterio-lateral corner of the knee and other avulsion injuries. Thus the presence of a segond fracture may indicate substantial menisco-ligamentous injury, and anterolateral instability must be considered to be present until proven otherwise. Various methods of fixation are used in operative treatment of tibial spine avulsion fractures varying from retrograde wires/screws, ante grade screws, suture anchors, and a recently described suture bridge and K-wire and tension band wiring technique [6]. Arthroscopic suture fixation for all cases is recommended by some authors due to less risk of neurovascular involvement and less problem of implant prominence [7].
Conclusion
A combination of avulsion injuries around the knee is very unique and rare. Although an accurate patient history and careful examination can lead us to a correct diagnosis of capsular ligamentous injuries of the knee, X- ray imaging should always be undertaken to identify significant avulsion fractures. Segond fracture should also be looked for since it often indicates possible ACL involvement (total or partial rupture) or avulsion and meniscal injury. Hence MRI imaging should be undertaken in all cases of Segond fracture.
Further research on anatomy and biomechanics of Anterolateral ligament is required to know the instability associated with the ligament and the need for reconstruction of the ligament in the near future.
[1]. Vinay G, Zile K, Rakesh G, Gaurav S, Bilateral traumatic patellar fracture: a case report and review of literatureChin J Traumatol 2012 15(3):188-91. [Google Scholar]
[2]. Gottsegen CJ, Eyer BA, White EA, Avulsion fractures of the knee: imaging findings and clinical significanceRadiographics 2008 28(6):1755-70. [Google Scholar]
[3]. Segond P, Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorseProgress med 1879 7:297-9.:319-21.:340-1. [Google Scholar]
[4]. Campos J, Chung C, Lektrakul N, Pedowitz R, Trudell D, Yu J, Pathogenesis of the Segond Fracture: Anatomic and MR Imaging Evidence of an Iliotibial Tract or Anterior Oblique Band Avulsion1Radiology 2001 219(2):381-86. [Google Scholar]
[5]. Dodds A, Halewood C, Gupte C, Williams A, Amis A, The anterolateral ligament: Anatomy, length changes and association with the Segond fractureThe Bone & Joint Journal 2014 96B(3):325-31. [Google Scholar]
[6]. Vikram Sapre and Vaibhav Bagaria (2013). Tibial Spine Avulsion Fractures: Current Concepts and Technical Note on Arthroscopic Techniques Used in Management of These Injuries, Regional Arthroscopy, Dr. Vaibhav Bagaria (Ed.), ISBN: 978-953-51-1044-6, InTech, DOI: 10.5772/549 [Google Scholar]
[7]. Lubowitz J, Elson W, Guttmann D, Part II: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fracturesArthroscopy: The Journal of Arthroscopic & Related Surgery 2005 21(1):86-92. [Google Scholar]