Background
The incidence of cancer is increasing throughout the world. One of the prime aims of its management is early diagnosis and therapeutic intervention. Factors causing delay to either of these goals should be identified and rectified.
Aim
To identify the factors causing delayed initial diagnosis and subsequent management in patients presenting to the Oncology department.
Materials and Methods
Three hundred proven cancer patients were prospectively evaluated for the pattern of presentation to the outpatient Department of Radiation Oncology of a Government Medical College (MC) in Central India.
Results
The mean age of presentation was 51.05 years (range 7 months-77 years). The number of male patients was 168 while females were 132. The duration of symptoms ranged from 20 days to 3 years. The number of patients with little/no education presented mainly in advanced stages as compared to their educated counterpart and this difference was statistically significant (p<0.001). The number of patients presenting directly to the department was 108, those diagnosed outside and referred to us was 84 while those diagnosed and received some form of oncologic treatment outside and referred thereafter was 108. The difference in the primary delay between patients presenting directly to the MC versus those diagnosed outside was significant (p=0.0126). The mean duration of starting definitive treatment after presentation to the outpatient was 4.68 days (range 0-22 days) and was very significantly (p< 0.001) less than the secondary delays caused to the other two subsets of patients.
Conclusion
Factors causing delayed presentation are both patient and system related. It is imperative to educate the common people regarding the early signs and symptoms of cancer. At the same time, the system needs to overhaul its efficiency to avoid secondary delays that adversely affect the treatment outcome. An upgradation of the existing oncology facilities in the public sector can achieve this target efficiently.
Introduction
Cancer is one of the leading causes of death in many countries despite the advancement in cancer treatment and diagnosis [1]. During the last 20 years, India has emerged as a fast growing economy with changes in lifestyle-related behaviour partially responsible for the increasing cancer burden and is among top three killers among adults in both rural and urban India [2]. Cancer incidence rates, while still lower compared with many western countries have been changing over recent decades [2]. One of the main reasons for this changing trend is delay in diagnosis or initiation of treatment at advanced stage [3]. Prolonged duration of diagnosis and treatment increases the proportion of advanced stages in cancer patients and has an impact on poor prognosis and quality of life [4].
Different types of delay can occur in total duration from onsets of symptoms to start of cancer treatment [4] and has classically been defined as primary (duration between onset of symptoms to first presentation to clinician) and secondary (from first presentation to clinician until start of treatment) [5]. Primary delay (PD) is also referred to as patient delay owing to the various factors responsible on the patient’s end that may include lack of information, poor socio-economic support, financial constraints etc. while secondary or clinician delay (SD) takes into account the patient’s characteristics and is also associated with doctor and system related factors [6–10].
The aim of this study was to assess the problem of delayed presentation of cancer patients to the Department of Radiation Oncology of a government Medical College (MC) of central India. The institute caters to a vast urban as well as rural population. We also aimed at identifying the patient and system related factors causing the delay and to propose possible means to rectify them.
Materials and Methods
The patients included in the study were 300 newly registered patients presenting to the Department of Radiation Oncology of a Government MC of central India. Case history was elucidated exhaustively with special reference to the duration of symptoms, duration of time to definitive diagnosis and any subsequent delays. Patients were evaluated for their level of education (illiterates/ attended primary school only/ completed school education/educated beyond schooling) as well. The timing of presentation was defined as early (T1/T2 stages) or delayed (T3/T4) stages and was correlated with the educational level of the patients. PD was defined as the duration from appearance of symptom, to the first consultation and arriving at the definitive diagnosis [11]. SD was defined as duration between diagnoses to the start of definitive treatment [11]. In addition, any delay caused after the start of treatment was also considered as a SD and reason identified. The patients were analysed for their presentation based on level of education and subsequently classified into 3 subgroups: (A) those presenting directly and being diagnosed in the MC; (B) those diagnosed outside and referred to the MC for further management and; (C) those diagnosed outside, and referred to MC following workup/incomplete treatment. These three subgroups of patients were further analysed for the duration of symptoms, PD, SD and the causative factors for the same. Online Graph Pad software was used for statistical analysis. A value of p < 0.05 was considered significant.
Results
In [Table/Fig-1], a total of 300 patients presenting to the outpatient prospectively were included for the present analysis. Of that, 56% (168/300) were males and 44% (132/300) were females. The overall mean age was 51.05 years (range 7 months-77 years). The mean age was 51.09 years in males (range 10 months-77 years) and 51 years in females (range 7 months- 70 years) respectively. Total number of patients < 30 years were 24 (8%), 31-60 years were 201 (67%) and >60 years were 75 (25%). The range of duration of symptoms was <3 months in 117 (39%) patients, 3-6 months in 93 (31%) patients and >6 months in 90 (30%) patients. Majority (135/300, 45%) patients had a diagnosis of head and neck cancer (HNC), followed by gastro-intestinal (16%), gynaecologic (15%), breast (12%), genito-urinary (4%), lymphomas (3%) and others (5%). 235 patients (78.33%) had a T3/T4 disease at presentation. The different educational level of the patients seen in the present analysis were, 93 (31%) patients were illiterates, 114 (38%) patients had attended primary school only, 54 (18%) patients had completed school education and 39 (13%) patients were educated beyond schooling . On correlating the incidence of early (T1/T2) versus advanced (T3/T4) disease at presentation with patients having no/ little education (n=207) or being educated (n=93) it was found that the educated subgroup (66.15%) presented chiefly in earlier stages while those having little or no education (77.87%) presented in advanced disease stages [Table/Fig-2]. This difference was found to be statistically significant (p<0.001) using Fisher’s exact test.
| Characteristic | n (%) |
|---|
| Total number of patients | 300 (100) |
| Males | 168 (56%) |
| Females | 132 (44%) |
| Age distribution |
| <30 years | 24(8%) |
| 31-60 years | 201 (67%) |
| >60 years | 75 (25%) |
| Mean age (overall) | 51.05 years (range 7 months-77 years) |
| Mean age (males) | 51.09 (range 10 months-77 years) |
| Mean age (females) | 51 years (range 7 months-70 years) |
| Educational levels |
| Illiterate | 93 (31%) |
| Primary schooling only | 114 (38%) |
| Complete schooling | 54 (18%) |
| Higher education | 39 (13%) |
| Pattern of presentation |
| Presenting directly to the MC | 108 (36%) |
| Diagnosed outside and then referred to MC | 84 (28%) |
| Diagnosed outside and received treatment outside and then referred to MC | 108 (36%) |
| Site wise distribution of cancers |
| Head and neck cancers | 135 (45%) |
| Gastro-Intestinal cancers | 48 (16%) |
| Gynaecological cancers | 45 (15%) |
| Breast cancer | 36 (12%) |
| Genito-Urinary cancers | 12 (4%) |
| Lymphomas | 09 (3%) |
| Others | 15 (5%) |
MC= Medical College
Distribution of early versus advanced disease presentation in different educational levels

The number of patients presenting directly to our institute (Group A) were 108 (36%). The mean PD in this subgroup was 4.30 months (range 15 days-12 months) while the mean time taken to start definitive treatment was 4.68 days (range 0-22 days) [Table/Fig-3].
Primary and secondary delays (months)
PD= Primary delay; SD= Secondary delay
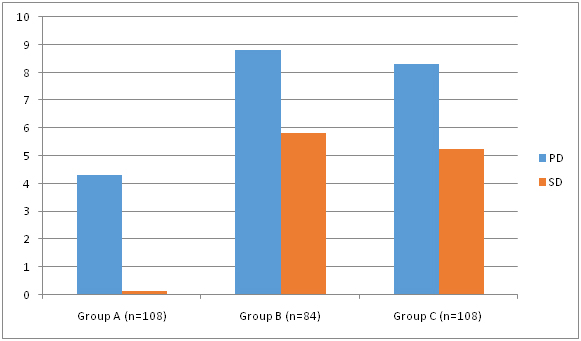
The number of patients diagnosed outside (Group B) and then referred to us was 84 (28 %). The mean PD in this subgroup was 8.82 months (range 1-36 months) whereas the mean time taken by the patients to present to the outpatient of our institution (SD) was 5.83 months (range 15 days-24 months).
The third subgroup (Group C) comprised of 108 patients (36%) who were diagnosed outside and either underwent diagnostic workup only, or started on definitive treatment in private institutions and then referred mid treatment citing financial exhaustion. The mean PD in this subgroup was 8.30 months (range 1-36 months) whereas the mean SD to present to the outpatient of our institute was 5.25 months (range 15 days-24 months).
On statistical analysis, the difference between the PD in Group A patients versus those of Group B and C was significant (p=0.0126). The SD caused after initial diagnosis and direct referral to the MC versus that after workup/treatment initiation followed by referral was not found to be significant (p=0.4076). However, the mean duration of starting definitive treatment after presentation to the outpatient was 4.68 days (range 0-22 days) and was very significantly (p< 0.001) less than the SD caused to the other two subsets of patients.
Discussion
Cancer has become a major and growing problem in today’s world. The appropriate management of cancer requires a complex Diagnostic evaluation, is a stepwise process [12] and invariably prone to delays. This problem is more pronounced in a developing country like ours owing to limitation of resources. There is growing evidence supporting an association between the duration of PD, stage at diagnosis and the subsequent patient survival. It also forms a key component of cancer control programmes worldwide [13]. Although early detection is one of the primary goal under the cancer control programs world-wide, but screening programs aimed to reduce the diagnostic delay are only amenable for a few cancer sub sites [14]. Prolonged duration of diagnosis and treatment increases the proportion of advanced stages in cancer patients and impacts on poor prognosis and quality of life [15–19]. Majority (235/300) of the patients in the current analysis presented in advanced stages of cancer.
The time lapse occurring between onset of symptoms to initiation of treatment is usually referred to as “stages of delay”. Most of the studies addressing this factor have differed in their study designs, definitions, analysis and reporting the study findings. In addition, most of these studies have been site specific and none has tried to correlate the various delays along with the causative factors in common cancer patients. [4,20–22]. Diagnostic delays can occur both due to patient not reaching to the provider or due to inappropriate referrals by provider, but the former has been found to be a major factor responsible [23,24]. Although there is no precise length of duration defined in literature that constitutes delay, in our analysis we observed the patient delay to be high in all the subgroups of the patients (4.30, 8.82 and 8.30 months respectively in groups A, B and C). Very often, a cancer symptom (unless grossly suspicious or obvious) is reported late to the clinician [25]. "Appraisal delay" refers to the time taken from symptom detection to recognizing the need to seek medical assistance. This delay has a higher occurrence in males and in the lower socioeconomic strata [26,27]. In our study, we observed a higher cancer occurrence in males than in females (56% versus 44%). Knowledge about cancer symptoms has been shown to be associated with paying more attention to symptoms and a shorter anticipated delay in help-seeking in the event of symptoms [25]. In the present analysis, most of the reasons for this delay comprised of unawareness regarding the signs and symptoms of cancer, consultation with unqualified local practitioners/no consultation, use of alternative medication, poor socio-economic conditions and lack of a proper referral infrastructure. These delays have been well documented in the past and are a known problem in developing nations [28–30]. However, an important variable discovered was that majority of the patients who were diagnosed outside claimed to be unaware of the available cancer management facilities in the government MC. In addition, the financial consideration required in getting treatment at the private institutions delayed their presentation. It appears to be a matter of grave concern and a novel finding of our analysis that mere ignorance and lack of proper directive to a government institution led to a significant difference in the PD between patients presenting directly to the MC versus those diagnosed outside. (p= 0.0126). To the best of our knowledge, this particular matter of being unaware of cancer treatment facilities in a government MC has not been addressed in the Indian setting.
The three subgroups identified represent the prevalent presentation patterns to our department. There is a relative paucity of literature addressing the association of delays caused by clinician, and associated factors in the management of cancer patients [27] as well as a scarcity of literature from developing countries in this regard. No study exists from India that provides an estimate for various levels of delay and their associated factors in cancer till date [4]. Various factors such as stage of cancer, disease aggressiveness, and patient and clinician characteristics affect the parameters of treatment initiation and needful referral [31]. Hansen et al., have highlighted the essential role of general practitioners in the proper and timely diagnosis and referral of cancer patients [12]. All possible attempts are mandated in this regard to educate the general practitioners to aid in timely diagnosis and proper referral.
We found that the majority of group C patients suffered the loop of being provided with an estimate for financial assistance from the private hospitals, receiving financial assistance from government that was invariably exhausted in pre treatment workup or before the completion of definitive treatment and was followed by referral to the MC. This vicious loop caused a significant delay of 5.25 months (range 15 days-24 months). This subgroup of patients being referred mid treatment also did not find any reference in literature search and highlights the urgent intervention required to address it. The trend of referral from peripheral government setups directly to the private institutions appears to be incorrect both professionally and for the patient per se.
Proper education is an imperative tool in the battle against cancer. Higher overall cancer incidence rates have been reported in the uneducated population as compared to the educated counterpart [12,32]. In our study, we found that 66.15% of patients who were educated presented in early stages while 77.87% of the patients with little or no education presented in advanced stages of the disease. Similar estimate has been seen in an African study that found most of the HNC patients with little or no education [33]. Literacy rates have also been indirectly linked to the socio-economic condition of the patients causing delayed presentations [34]. The major cancer sub site in the patients evaluated by us was HNC (45%). Literature review reveals factors such as educational levels, availability of treatment resources and knowledge regarding cancer issues to be important factors affecting the delays in similar settings [35–38]. Education level independently has also been shown to affect treatment outcome in a large study of radiation regimens in HNC that revealed a significantly improved overall survival and loco regional control in patients with post-secondary education that was independent of stage of disease presentation [39]. To reduce secondary delay, there appears to be a need of intervention programs to make community more aware about cancer related information as well as to get the doctors more updated towards making confirmatory diagnosis of cancer [4]. General population, especially those residing in the rural regions need to be made aware regarding the common signs and symptoms of cancer, and more importantly that of the available cancer care facilities in the Government MC providing treatment free of cost. Also, the private institutions should accept a patient only after due understanding and willingness to provide the complete management, rather than stopping in between in lieu of financial reasons. If a person is eligible for financial assistance, the estimate should be able to cover the entire treatment cost rather than a fraction of it.
Our study supports the hypothesis that raising awareness of the early signs and symptoms of cancer through an improved education level may lead to early identification of cancer symptoms. If the PD is reduced and patients may present early to the MC, we hope to provide a better outcome. Also, as an observation from the present study, not all the educated patients presented early and not all the patients with little or no education presented in advanced stages of the disease. These results indicate the fact that that knowledge alone is insufficient to promote appropriate help-seeking [40] and addressing barriers to seeking medical care is an important target that requires action at both patient and provider level. Different types of barriers find reference in literature for varied cancer sites such as delayed symptom recognition and misconceptions in breast cancer patients [41,42] and diagnostic delays in cervical cancer patients [43]. Sachdeva et al., in their analysis of lung cancers described a wide range of factors causing delayed presentation that included not considering the symptoms serious, nobody to escort to health facility, financial constraints, preference for local practitioner, family commitments and fear of death [44]. Wahls and Peleg in their study for identifying barriers for early diagnosis of colorectal cancers reported frequent missed opportunities at the provider’s end causing delayed presentations [45]. All these factors, either alone or simultaneously appear to be involved at a basic level resulting in delayed presentations and management.
Limitation
This study has its drawbacks in not formulating any definitive association incorporating the financial status of the patient and not being site specific. In addition, this study did not take into account the clinical implications caused by the delay with respect to disease progression. The time lapse causing SD most certainly affects the treatment outcome adversely and needs to be studied in detail.
Conclusion
Management of cancer is a multi-speciality affair requiring the use of modalities like surgery, radiotherapy, chemotherapy, pathology, radiology. We believe that identifying the important co-factors that can be modifiable through appropriate intervention programs related to delay would not only reduce delays in diagnosis but also minimize time in initiating treatment. It is advisable to upgrade the existing facilities in the medical college so as to allow a comprehensive and world class cancer care that can cater to the poor and underprivileged population without an aim of financial gains, but those of patient welfare, comprehensive cancer management and paving a way of academic research. We recommend further studies pinpointing the causes of PD and SD and addressing the paradigm of the impact caused by incomplete treatment followed by referrals from corporate hospitals. The factors responsible should be managed accordingly in the best of patient’s interest.
MC= Medical College
[1]. World Health Organization (WHO) (2006) Cancer. Geneva, WHO [Google Scholar]
[2]. Badwe RA, Dikshit R, Laversanne M, Bray F, Cancer incidence trends in IndiaJpn J Clin Oncol 2014 44:401-07. [Google Scholar]
[3]. Neal RD, Do diagnostic delays in cancer matter?British Journal of Cancer 2009 101(Suppl 2):S9-S12. [Google Scholar]
[4]. Dwivedi AK, Dwivedi SN, Deo S, Shukla R, Pandey A, Dwivedi DK, An epidemiological study on delay in treatment initiation of cancer patientsHealth 2012 4(2):66-79. [Google Scholar]
[5]. Facione NC, Delay versus help seeking for breast cancer symptoms: A critical review of the literature on patient and provider delaySoc Sci Med 1993 36:1521-34. [Google Scholar]
[6]. Gorin SS, Heck JE, Cheng B, Smith SJ, Delays in breast cancer diagnosis and treatment by racial/ethnic groupArch Intern Med 2006 166:2244-52. [Google Scholar]
[7]. Salomaa ER, Sallinen S, Hiekkanen H, Liippo K, Delays in the diagnosis and treatment of lung cancerChest 2005 128:2282-88. [Google Scholar]
[8]. Allgar VL, Neal RD, Delays in the diagnosis of six cancers: Analysis of data from the national survey of NHS patients: CancerBr J Cancer 2005 92:1959-70. [Google Scholar]
[9]. Look M, Tan YY, Vijayan A, Teh CH, Low CH, Management delays for early gastric cancer in a country without mass screeningHepatogastroenterology 2003 50:873-76. [Google Scholar]
[10]. Amir Z, Kwan SY, Landes D, Feber T, Williams SA, Diagnostic delays in head and neck cancersEur J Cancer Care (Engl) 1999 8:198-203. [Google Scholar]
[11]. Caplan L, Delay in breast cancer: implications for stage at diagnosis and survivalFront Public Health 2014 2:87 [Google Scholar]
[12]. Hansen RP, Olesen F, Sorensen HT, Sokolowski I, Sondergaard J, Socioeconomic patient characteristics predict delay in cancer diagnosis: a Danish cohort studyBMC Health Serv Res 2008 8:49 [Google Scholar]
[13]. Dobson CM, Russell AJ, Rubin GP, Patient delay in cancer diagnosis: what do we really mean and can we be more specific?BMC Health Serv Res 2014 14:387 [Google Scholar]
[14]. Dodd S, Bassi A, Bodger K, Williamson P, A comparison of multivariable regression models to analyse cost dataJ Eval Clin Pract 2006 12:76-86. [Google Scholar]
[15]. Korsgaard M, Pedersen L, Laurberg S, Delay of diagnosis and treatment of colorectal cancer—A population-based Danish studyCancer Detect Prev 2008 32:45-51. [Google Scholar]
[16]. Hosseini SN, Mousavinasab SN, Moghimi MH, Fallah R, Delay in diagnosis and treatment of gastric cancer: From the beginning of symptoms to surgery–An Iranian studyTurk J Gastroenterol 2007 18:77-81. [Google Scholar]
[17]. Pitchers M, Martin C, Delay in referral of oropharyngeal squamous cell carcinoma to secondary care correlates with a more advanced stage at presentation, and is associated with poorer survivalBr J Cancer 2006 94:955-58. [Google Scholar]
[18]. Nyström L, Rutqvist LE, Wall S, Lindgren A, Lindqvist M, Rydén S, Breast cancer screening with mammography: Overview of Swedish randomized trialsLancet 1993 341:973-8. [Google Scholar]
[19]. Risberg T, Sørbye SW, Norum J, Wist EA, Diagnostic delay causes more psychological distress in female than in male cancer patientsAnticancer Res 1996 16:995-99. [Google Scholar]
[20]. Andersen BL, Cacioppo JT, Delay in seeking a cancer diagnosis: delay stages and psychophysiological comparison processesBr J Soc Psychol 1995 34:33-52. [Google Scholar]
[21]. Walter F, Webster A, Scott S, Emery J, The Andersen Model of Total Patient Delay: a systematic review of its application in cancer diagnosisJ Health Serv Res Policy 2012 17:110-18. [Google Scholar]
[22]. Almuammar A, Dryden C, Burr JA, Factors associated with late presentation of cancer: A limited literature reviewJournal of Radiotherapy in Practice 2010 9(2):117-23. [Google Scholar]
[23]. Mitchell E, Macdonald S, Campbell NC, Weller D, Macleod U, Influences on pre-hospital delay in the diagnosis of colorectal cancer: a systematic reviewBr J Cancer 2008 98:60-70. [Google Scholar]
[24]. Macdonald S, Macleod U, Campbell NC, Weller D, Mitchell E, Systematic review of factors influencing patient and practitioner delay in diagnosis of upper gastrointestinal cancerBr J Cancer 2006 94:1272-80. [Google Scholar]
[25]. Simon AE, Waller J, Robb K, Wardle J, Patient delay in presentation of possible cancer symptoms: the contribution of knowledge and attitudes in a population sample from the United kingdomCancer Epidemiol Biomarkers Prev 2010 19:2272-77. [Google Scholar]
[26]. de Nooijer J, Lechner L, de Vries H, Social psychological correlates of paying attention to cancer symptoms and seeking medical helpSoc Sci Med 2003 56:915-20. [Google Scholar]
[27]. Macleod U, Mitchell ED, Burgess C, Macdonald S, Ramirez AJ, Risk factors for delayed presentation and referral of symptomatic cancer: evidence for common cancersBr J Cancer 2009 101(Suppl 2):S92-101. [Google Scholar]
[28]. Ernst E, Cassileth BR, The prevalence of complementary/ alternative medicine in cancer: a systematic reviewCancer 1998 83(4):777-82. [Google Scholar]
[29]. Kumar S, Heller RF, Pandey U, Tewari V, Bala N, Oanh KT, Delay in presentation of oral cancer: a multifactor analytical studyNatl Med J India 2001 14:13-7. [Google Scholar]
[30]. Kumar S, Agarwal SP, Gupta CK, Investigation of factors causing delay in the treatment of oral mucosal cancerIndian J Oral Maxillofac Surg 1993 8(2):41-7. [Google Scholar]
[31]. Esteva M, Ramos M, Cabeza E, Llobera J, Ruiz A, Pita S, Factors influencing delay in the diagnosis of colorectal cancer: A study protocolBMC Cancer 2007 7:86 [Google Scholar]
[32]. Swaminathan R, Selvakumaran R, Vinodha J, Ferlay J, Sauvaget C, Esmy PO, Education and cancer incidence in a rural population in South IndiaCancer Epidemiol 2009 33:89-93. [Google Scholar]
[33]. Onyango JF, Macharia IM, Delays in diagnosis, referral and management of head and neck cancer presenting at Kenyatta national hospital, NairobiEast Afr Med J 2006 83(4):85-91. [Google Scholar]
[34]. Krishnatreya M, Kataki AC, Sharma JD, Nandy P, Rahman T, Kumar M, Educational levels and delays in start of treatment for head and neck cancers in North-East IndiaAsian Pac J Cancer Prev 2014 15:10867-69. [Google Scholar]
[35]. Amar A, Chedid HM, Franzi SA, Rapoport A, Diagnostic and therapeutic delay in patients with larynx cancer at a reference public hospitalBraz J Otolaryngol 2010 76:700-03. [Google Scholar]
[36]. Panzarella V, Pizzo G, Calvino F, Diagnostic delay in oral squamous cell carcinoma: the role of cognitive and psychological variablesInt J Oral Sci 2014 6(1):39-45. [Google Scholar]
[37]. Patel UA, Brennan TE, Disparities in head and neck cancer: assessing delay in treatment initiationLaryngoscope 2012 122:1756-60. [Google Scholar]
[38]. Lyhne NM, Christensen A, Alanin MC, Waiting times for diagnosis and treatment of head and neck cancer in Denmark in 2010 compared to 1992 and 2002Eur J Cancer 2013 49:1627-33. [Google Scholar]
[39]. Konski A, Berkey BA, Ang K, Fu KK, Effect of education level on outcome of patients treated on Radiation Therapy Oncology Group protocol 90-03Cancer 2003 98(7):1497-503. [Google Scholar]
[40]. Austoker J, Bankhead C, Forbes LJ, Atkins L, Martin F, Robb K, Interventions to promote cancer awareness and early presentation: systematic reviewBr J Cancer 2009 101(Suppl 2):S31-39. [Google Scholar]
[41]. Khan MA, Hanif S, Iqbal S, Shahzad MF, Shafique S, Khan MT, Presentation delay in breast cancer patients and its association with sociodemographic factors in North PakistanChin J Cancer Res 2015 27:288-93. [Google Scholar]
[42]. Pakseresht S, Ingle GK, Garg S, Sarafraz N, Stage at diagnosis and delay in seeking medical care among women with breast cancer, delhi, IndiaIran Red Crescent Med J 2014 16(12):e14490doi: 10.5812/ircmj.14490 [Google Scholar]
[43]. Gyenwali D, Khanal G, Paudel R, Amatya A, Pariyar J, Onta SR, Estimates of delays in diagnosis of cervical cancer in NepalBMC Womens Health 2014 14:29doi: 10.1186/1472-6874-14-29 [Google Scholar]
[44]. Sachdeva R, Sachdeva S, Delay in diagnosis amongst carcinoma lung patients presenting at a tertiary respiratory centreClin Cancer Investig J 2014 3:288-92. [Google Scholar]
[45]. Wahls TL, Peleg I, Patient- and system-related barriers for the earlier diagnosis of colorectal cancerBMC Fam Pract 2009 10:65doi: 10.1186/1471-2296-10-65 [Google Scholar]