The term “Periodontal Diseases” is a collective term used to explain the inflammatory and diseased conditions of the periodontal structures. It can include an early case of gingivitis where the damage is very limited to an advanced case of aggressive periodontitis where there is an extensive damage to periodontium resulting in loss of connective tissue attachment, alveolar bone and associated tooth mobility. One of the most significant approaches to deal with “Periodontal Diseases” is timely and correct detection [1].
At present, in most of the clinical setups periodontitis is diagnosed almost entirely based on a variety of clinical parameters or measurements, which include probing depth (PD), clinical attachment level (CAL), bleeding on probing (BOP), plaque index (PI) and radio graphical changes or findings. These traditional methods have some advantages & disadvantages [2,3].
Advantages associated with these methods include being easy to use, cost-effective and relatively non-invasive. However, the major disadvantage of these techniques is that they are static diagnostic parameters, indicating the disease history and not the current status of the disease [4]. By the time these parameters reach the minimum threshold value to be clinically detectable, considerable damage to periodontal structures have already taken place. So, there is a need for a biomarker that can be correctly & easily quantified and which can predict the diseased status of the periodontium much before any considerable damage is done to the periodontal structures including the alveolar bone. Such a biomarker will effectively enhance the prediction and treatment plan there by greatly improving the outcome of the periodontal treatment [5].
It has been stated that it is unlikely that any one single clinical or laboratory examination can address all issues concerning diagnosis, classification, comparison & prognosis of periodontal diseases. In such a scenario, whole saliva and its contents represent a promising diagnostic fluid for the screening of periodontal disease. Saliva acts as a cumulative diagnostics fluid in the oral cavity containing not only the constituents of the exocrine salivary glands but also the gingival crevicular fluids. Thus it has the advantage of providing overall idea about periodontal health status. Saliva collection is relatively easier than collecting serum or GCF and doesn’t need sophisticated instrumentation. Saliva collection is also not very technique sensitive. Saliva contains many biological ingredients that are produced in response to various diseased state of the human body. Identifying these biological ingredients can give clear-cut information on the current status of disease progression and allowing the periodontists to formulate a better treatment [6–13].
The present study involves the direct measurement of a potential biomarker in the human whole saliva of a bone-specific molecule called pyridinoline cross-linked carboxy-terminal telopeptide of Type I collagen (ICTP). The value of pyridinoline cross-links as markers of bone turnover is because of their specificity for bone [14].
ICTP concentration is currently being used as a diagnostic marker of active bone resorption in many systemic metabolic bone diseases such as postmenopausal osteoporosis, myxoedema, thyrotoxicosis, and primary hyperparathyriodism [15–18]. In the present study, an attempt has been made to compare the concentration of the salivary ICTP levels in periodontal health and disease.
The aim of the present study is to evaluate the concentration of ICTP in the salivary samples in order to assess its relation with periodontal health and diseased conditions.
Materials and Methods
Study Population
The study population comprised of randomly selected patients who visited the outpatient Department of Periodontics, Ragas Dental College and Hospital, Chennai, India. The Institutional Review Board of Ragas Dental College approved the study protocol. The study protocol was explained to the patients. The study was started on July 2013 and the time period of the study was six months. Before conducting the study, informed consent was obtained from each of the patients.
Inclusion criteria of patients
Patients who were systemically healthy.
Patients who were non-smokers.
No history of anti-microbial therapy for the past three months.
Exclusion criteria of patients
Pregnant ladies and Lactating Mothers.
Smokers.
Patients with history of systemic disease. Any underlying systemic disease will have effect on periodontal status.
Patients who have undergone periodontal therapy or antibiotic therapy in the past 6 months or any other drugs as there will be effect on the periodontal status.
Presence of any pre-existing oral infected condition. For e.g. – pulpal pathosis.
Any patient undergoing radiation therapy.
After excluding the patients based on the exclusion criteria a total of 43 patients were selected for the study.
The selected patients were allocated into three groups based on the traditional clinical parameters of Probing depth (PD), bleeding on probing (BOP), and clinical attachment loss (CAL)
Group A: Eleven periodontally healthy subjects [Table/Fig-1a] (3 males & 8 females of age 20-50 years (mean 35.6 years) showing no signs of periodontal disease diagnosed clinically by the absence of bleeding on probing (BOP), no clinical attachment loss (CAL) and probing depth of (PD) ≤ 3mm. No sign of any radiographic bone loss.
Intra-oral picture showing healthy gingiva in group A patients

Group B: Seventeen subjects with gingivitis [Table/Fig-1b] (8 males & 9 females) of age 20- 50 years (mean 36 years) with PD<3mm, no clinical attachment loss but presence of bleeding on probing (BOP) in at least 6 sites. No radiographic evidence of bone loss.
Intra-oral picture showing gingivitis in group B patients

Group C: Fifteen subjects with chronic periodontitis [Table/Fig-1c] (10 males & 5 females) of age 20-50 years (mean 36.7 years) exhibiting PD > 5 mm, CAL ≥ 3 mm and presence of BOP in at least six sites. Radiographic evidence of bone loss more than 30% of the tooth was seen.
Intra-oral picture showing periodontitis in group C patients

These parameters have been used regularly to distinguish between healthy and diseased periodontium [2]. Recording and evaluation of these parameters are relatively easy and they provide a quick assessment of the periodontal health status [3]. But these parameters are indicative of the periodontal damage that has already taken place. In many cases by the time a patient comes for evaluation, considerable damage to periodontal tissues have already taken place. In such cases the scope to restore the periodontal health becomes difficult [4]. Thus there is the requirement for a biomarker that can easily predict the underlying periodontal disease before there is extensive clinical damage to periodontal tissues.
Clinical Evaluation
William’s periodontal probe was used for clinical evaluation along with mouth mirror. Full mouth plaque score (FMPS) and Full mouth bleeding score (FMBS) were evaluated.
Saliva Collection
Salivary collection is done according to the technique proposed by Navazesh et al., [11] A special armamentarium including micropipettes was used [Table/Fig-2a,b]. Samples were collected in the morning hours before patients had taken breakfast. Patients were advised to refrain from intake of any food or beverage (water exempted) one hour before sampling. The subjects were also advised to rinse his or her mouth several times with (deionized) distilled water and then to relax for five minutes. The patient is asked to lean the head forward tilting over the container with the mouth slightly open and allow the saliva to drain into the container with the eyes open. Sterile disposable plastic containers were used for the collection of samples [Table/Fig-2c,d]. The duration of saliva collection was 5 minutes and the samples were then centrifuged at 2800 rpm and were stored at -20°C for future assessment.
(2a) Armamentarium used in the study (2b) Micro-pipette (2c) Container for saliva collection (2d) Procedure of saliva collection from the patient (2e) Salivary specimen in centrifuge (2f) Micro plate with salivary samples (2g) ELISA reader with micro plate containing salivary samples (2h) Human cross linked carboxy terminal telopeptide of type I collagen ELISA kit (2i) Standard solution (2j) Stop solution (2k) Chromogen A and B solution (2l) The ELISA procedure (2m) ELISA reader evaluating the salivary samples (2n) Automatic washer

Principle of the Method
The Bio source ELISA Kit used for this study is based on the principle of double-antibody sandwich technique to detect Human ICTP [Table/Fig-2e-n]. Assay preparation of ICTP and standard solution were prepared according to manufacturer’s instructions. Monoclonal antibody enzyme wells are pre-coated with Human Cross-linked Carboxy-terminal Telopeptide of type I, collagen (ICTP) monoclonal antibody. Samples are added to these monoclonal antibody enzyme wells.
Then, cross-linked carboxy-terminal telopeptide of type I collagen (ICTP) antibodies labelled with biotin were combined with Streptavidin-HRP to form immune complex. Wells were incubated for 60 minutes. After incubation, washing was done to remove the un-combined enzymes. Then chromogen Solution A, B were added and the colour of the liquid changed into blue. Due to the effect of acid, the colour finally became yellow.
The intensity of the coloured complex is dependent on the concentration of the ICTP present in the samples and standard. A standard curve is obtained by plotting the generated OD values for each standard against expected concentration. Evaluating the standard curve accurately we can determine the concentration of ICTP in the samples under investigation.
Statistical Analysis
The mean & standard deviation were calculated in periodontal health and disease. Kruskal Wallis test was used to compare the means of three groups followed by Mann Whitney test to make pairwise comparison. Correlation coefficient of saliva in relation to ICTP in periodontal health and disease was analysed using Pearson’s correlation. p< 0.05 was considered to be statistically significant.
Results
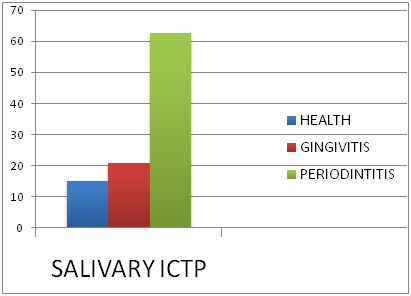
Results(Values of salivary levels of ICTP in periodontal health, gingivitis and periodontitis)
Mean and disease
The mean salivary ICTP level in health samples was 15.16ng/ml.
The mean salivary ICTP level in gingivitis samples was 20.88ng/ml.
The mean ICTP level in periodontitis samples was 62.63ng/ml.
There was statistically significant increase in the salivary ICTP level in disease when compared to health p = 0.001 (p < 0.05) [Table/Fig-3].
Mean salivary ictp levels
| Group | N | Mean ICTP | Std. Deviation | H value* | p-value |
|---|
| Health | 11 | 15.1688 | 4.89202 | 30.51 | 0.001 |
| Gingivitis | 17 | 20.8818 | 5.88650 |
| Periodontitis | 15 | 62.6380 | 10.31376 |
* Kruskall Wallis
Pairwise Comparison of Salivary ICTP Levels in the Periodontal Health and Disease Groups-
Pairwise comparison of ICTP levels between health and gingivitis showed statistical significance [p=0.03 (p < 0.05)].
Pairwise comparison of ICTP levels between gingivitis and periodontitis showed a statistically significant value. [p =0.001 (p < 0.05)].
Pairwise comparison of ICTP levels between health and periodontitis showed a statistically significant value. [p=0.001 (p < 0.05)].
There was also statistically significant increase in the levels of ICTP in the pair wise comparison of the samples of health & disease (gingivitis and periodontitis) [Table/Fig-4,5]. [Table/Fig-6,7,8,9,10,11 and 12] summarize the results of the study comparing the samples in health and disease.
Table showing mean MCD values of normal oral mucosa and different grades of oral squamous cell carcinoma
| Group | p-value* |
|---|
| Health Vs Gingivitis | 0.03 |
| Gingivitis Vs Periodontitis | 0.001 |
| Health VsPeridontitis | 0.001 |
*Mann Whitney test, Post Hoc Test for pair wise comparision
Correlation of salivary ictp with clinical parameters
| Group | FMPS | FMBS | PPD | CAL |
|---|
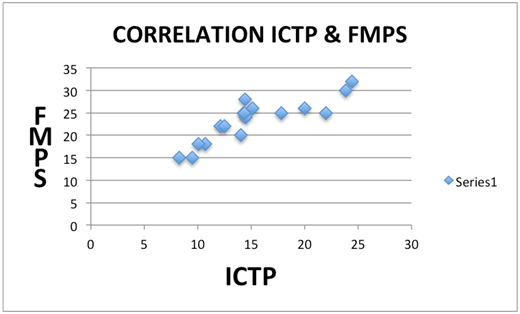
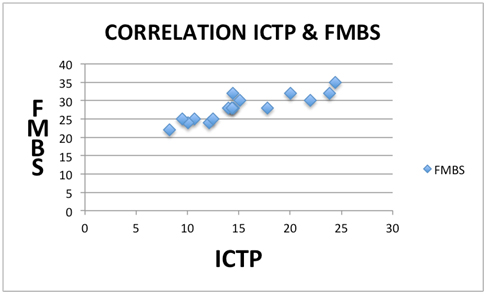
| Spearman’s Correlation | Gingivitis | ICTP | Correlation Coefficient | .902 | .905 | 0.08 | |
| Sig. | .001 | .001 | 0.79 | |
| n | 17 | 17 | | |
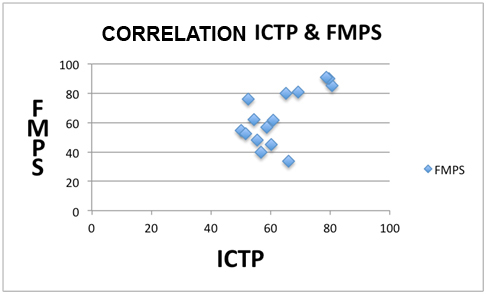
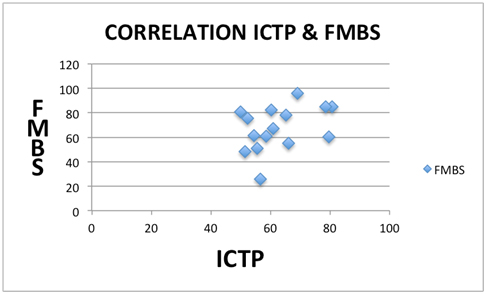
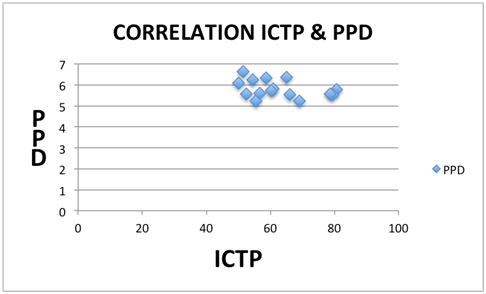
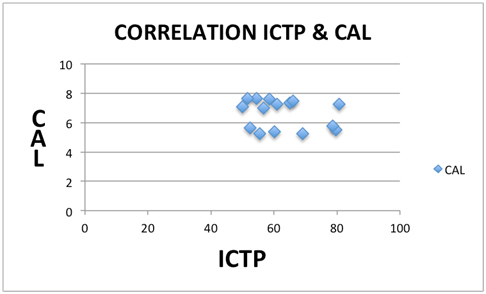
| Periodontitis | ICTP | Correlation Coefficient | .536 | .407 | -.361 | -.080 |
| Sig. | .04 | .132 | .187 | .776 |
| n | 15 | 15 | 15 | 15 |
Comparision of mean salivary ictp in health, gingivitis and periodontitis
Correlation between ICTP & FMPS in gingivitis samples
Correlation between ICTP & FMBS in gingivitissamples
Correlation between ICTP & FMPS in periodontitis samples
Correlation between ICTP & FMBS in periodontitis samples
Correlation between ICTP & PPD in periodontitis samples
Correlation between ICTP & CAL in periodontitis samples
Discussion
Periodontitis is a chronic inflammatory condition that leads to destruction of supporting periodontal structures. Loss of alveolar bone is considered as a classical sign of periodontitis [19].
In the present study saliva was used, as the diagnostic tool to identify the presence of ICTP. Sandwich ELISA technique was used for the detection of human ICTP in the salivary samples. This technique was used because of its more sensitivity and the chance to get more accurate results.
Traditionally GCF has been used as a diagnostic fluid for the assessment of the biomarkers that are produced in response to periodontal diseases. Other than being site specific GCF has the advantage of having inflammatory mediators and tissue destructive factors that can be evaluated to assess the extent of progress of the periodontal disease [20]. However analysis of GCF takes a lot of time, sometimes requiring multiple attempts at a particular site to collect an ideal sample not contaminated by blood. The process needs more effort and is highly technique sensitive that requires the use of sophisticated equipment to accurately calibrate the volume of the fluid. The laboratory based analysis for the GCF is also expensive and cannot be done chair side. The amount of GCF that can be collected from a particular site is usually very miniscule (around 1μL). Any slight contamination by blood, plaque and saliva can lead to the wastage of the entire sample unit and the whole procedure will then have to be repeated [7]. Considering the problems associated with GCF that we discussed above, saliva is gradually being preferred as a diagnostic fluid [7,8].
The crucial points that make saliva a credible diagnostic fluid over GCF are:
Saliva collection is a relatively non-invasive method for collecting biological samples.
Compared to collection of GCF, saliva collection is much simpler, less time consuming and cost effective.
There are more chances that biomarkers specific to bone resorption may be present in saliva.
GCF is collected in relation to a particular site & tooth. But saliva acts as a cumulative sample related to all the affected periodontal sites. Thus salivary samples provide an overall information on periodontal disease or health status of the subject as compared to the site specific information provided by GCF samples [7].
GCF is generally low in concentration in health but as periodontal disease progresses GCF is produced as inflammatory exudate at the affected sites. In many cases by the time adequate clinical level of GCF is produced that can firmly establish periodontal disease, tissue damage would already have taken place. In comparison saliva is produced in both periodontal health and disease. So detection of even minute traces of tissue loss biomarkers can help periodontists to predict periodontitis before any considerable clinical damage is done [7].
Saliva samples are not only easy to collect and store but also provide an overall picture of the periodontal health as it’s a collection of the fluid and biomarkers from all the affected sited. Compared to this GCF is only site specific. Because of this, saliva is being preferred more as a diagnostic fluid to be used in quick assay procedures that are gradually being use as point-of-care (POC) devices. This helps in performing rapid tests, quick diagnosis and early clinical treatment of periodontal disease [8].
Non-invasive methods are being preferred more and more as the ideal way to monitor health status, onset of disease and its progression and treatment outcome. In this regard use of saliva as a diagnostic medium to identify biomarkers for evaluating periodontal status is of great importance [6].
Loss of alveolar bone is considered as a classical sign of periodontitis. Traditionally, clinical parameters like pocket depth (PD), clinical attachment loss (CAL) and bleeding on probing (BOP) are still being used today to assess periodontal conditions of health and disease. However, considerable amount of bone destruction would have occurred before an effective diagnosis of periodontal disease can be established. They measure the damage from past episodes of destruction and require a 2 to 3 mm threshold changes before a site can be deemed, as having experienced significant breakdown [9].
The traditional parameters can be used to assess the post inflammatory damages but it cannot be used to predict the current progressive status of the disease and because of this multiple patients’ visits and recording of these parameters is needed. Another drawback of the traditional parameters is the inability to clearly identify a case of progressing gingivitis that can lead to periodontitis [4]. A marker that can give a real time assessment of periodontitis progression status before any considerable loss of hard and soft tissue will help in the early diagnosis of the disease. Early diagnosis will lead to a better treatment plan and better prognosis.
Pyridinoline cross-linked carboxy terminal telopeptide (ICTP) is a breakdown product of Type I collagen, which is the major constituent of alveolar bone [20]. In case of periodontitis there is accelerated osteoplastic resorption and collagen matrix degradation which results in the production of pyridinoline, deoxy-pyridinoline and amino & carboxy terminal cross linked telopeptides of type I collagen which then enter the circulation [21]. These molecules are produced as a result of post-translational modification of collagen molecules. Due to collagen matrix degradation in response to periodontal diseases, these molecules are released into the circulation and cannot be used again in the synthesis of collagen. With the increase in the severity of periodontal disease, there is an increase in the concentration of these products in the blood. Because of this ICTP is being considered as a specific biomarker of periodontal tissue breakdown [14]. In skin and other soft tissues Histidine cross-links of collagen are more in concentration [22]. But in alveolar bone the dominant form of type I collagen is ICTP (Pyridinoline cross-linked carboxy-terminal telopeptide of type I collagen. In progressive periodontal disease ICTP is degraded and released by the action of bacterial collagenase or pro inflammatory mediators [23]. Thus, ICTP is considered specific to alveolar bone loss and thus of special interest for timely diagnosis of periodontitis.
Because of this specificity as a by-product of alveolar bone destruction pyridinoline cross-links can be used as possible diagnostic markers to detect periodontitis. ICTP being a biomarker specific to bone degradation can be used clinically to differentiate gingival inflammation from progressive periodontitis [24].
Sandwich Enzyme-linked immune sorbent assay (ELISA) has been used in both experimental and diagnostic techniques [25]. This study was hence undertaken to assess the concentration of ICTP levels in the salivary samples of periodontal health and disease and to evaluate if there is a change in the concentration of salivary ICTP within the healthy and diseased samples of gingivitis and periodontitis.
The present study was cross sectional in nature where the salivary ICTP levels were assessed in all the three groups of health, gingivitis and periodontitis. The result of this study showed a significant increase in the concentration of ICTP in the saliva as we moved from the healthy samples to diseased samples of gingivitis and periodontitis. Also a pairwise comparison between the groups showed an increase in the concentration of ICTP in the diseased samples compared to health samples. The concentration of ICTP was highest in the samples of periodontitis.
Kinney et al., and Gursoy et al., found in their study that there is an increase in salivary ICTP concentration in periodontitis samples compared to healthy samples [9,26]. They concluded that increased ICTP levels could be used as an indicator of diseased periodontal status. Giannobile et al., in their study concluded that pyridinoline cross-links are active indicators of alveolar bone loss that is caused by periodontitis and their presence can be used to differentiate between active gingivitis from periodontitis [23]. Palys et al., reported in their study that there was a positive relationship between ICTP and the putative pathogens that are found in case of active periodontal disease [27]. Giannobile et al., established in their study that ICTP relates positively to indices of active periodontal bony destruction and suggested that these molecules may serve as predictive markers for future alveolar bone loss [23]. Gursoy et al., stated that ICTP are potential candidates in the detection of advanced periodontitis [28]. Calvo et al., concluded that pyridinoline crosslinks belong to a class of collagen-degrading molecules. The major collagen degradation molecules are pyridinoline, deoxypyridinoline, N-telopeptides and C-telopeptides [29]. Payne et al., have stated that ICTP concentration is significantly associated with alveolar bone density loss & alveolar bone height loss [30]. The present study was consistent with the finding of the above studies, indicating that the concentration of ICTP, a breakdown product of type I collagen present in alveolar bone, was present in more quantity in patients with periodontitis. The lowest concentration was found in periodontally healthy patients. However Thomas et al., in contrast have reported that they were unable to find any significant traces of detectable ICTP in the collected salivary samples of periodontitis patients [25].
Though the present study did provide a correlation between ICTP concentrations in saliva and periodontal health, however further studies with a bigger sample size from different demographics with further strengthen the findings. In the present study ICTP salivary concentrations in patients having periodontitis have not been evaluated post treatment. This evaluation may further give us information on the relation of salivary ICTP concentration to periodontal treatment.
Conclusion
The salivary levels of ICTP showed a significant increase between healthy and diseased samples. The pair wise comparison indicated that the concentration of salivary ICTP was more in the diseased samples of gingivitis and periodontitis compared to the healthy samples. The periodontitis samples had the maximum concentration of the salivary ICTP. Hence, the evaluation of the presence of ICTP in human saliva can be used as an indicator to assess the overall state of periodontal health and disease. More studies with larger sample size are needed to establish a correlation between the ICTP concentrations and individual clinical parameters.