Intramuscular Ossified Haemangioma: A Rare Case Report
Mano Ananth Arivazhagan Brinda1, Srinidhi Manjunath2, Kanakapura Srinivasamurthy Balasubrahmaniya3, R.D Manjunath4, Basavaraju Nanjaiah5
1 Post Graduate, Department of General Surgery, Mysore Medical College and Research Institute, Mysore, India.
2 Senior Resident, Department of General Surgery, Mysore Medical College and Research Institute, Mysore, India.
3 Associate Professor, Department of General Surgery, Mysore Medical College and Research Institute, Mysore, India.
4 Assistant Professor, Department of General Surgery, Mysore Medical College and Research Institute, Mysore, India.
5 Post Graduate, Department of General Surgery, Mysore Medical College and Research Institute, Mysore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mano Ananth Arivazhagan Brinda, Post Graduate, Department of General Surgery, Mysore Medical College and Research Institute, Mysore-570001, India.
E-mail: ananth.mano88@gmail.com
Haemangiomas are benign vascular neoplasm and intra muscular haemangioma constitutes 0.8% of all. Of these intramuscular ossified haemangioma is very rare. Here we are reporting a 30-year-old female admitted in our institute with complaints of pain and swelling in the medial aspect of right thigh for duration of one year. On evaluation CT showed well defined soft tissue lesion with calcification in vastus medialis which on guided aspiration showed numerous RBCs along with clusters of histiocytes with occasional calcified specs seen without presence of granulomas. The swelling was excised and histopathology confirmed intra muscular haemangioma with ossification. We hereby reporting a rare case of calcified intra muscular cavernous haemangioma which should be considered as differential diagnosis in any case of deep seated swelling with unexplained pain.
Calcifications, Vascular neoplasm, Haemangioma, Cavernous
Case Report
A 30-year-old female patient was admitted with complaints of pain and swelling in right thigh for duration of one year. Pain was insidious in onset, progressive in nature and the swelling gradually increased in size. No history of trauma and restriction of movements. On examination, an oval shaped swelling of size about 3 x 2 cm is noted in the medial aspect of lower third of right thigh. The swelling is tender, hard in consistency and moves horizontally.
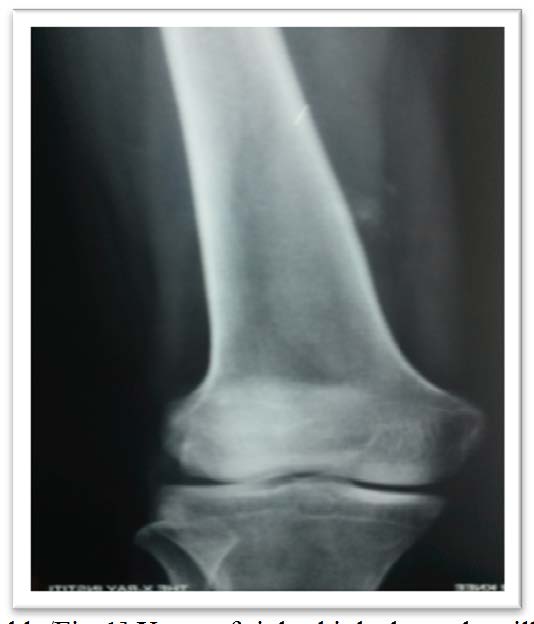
On imaging studies, x-ray right thigh revealed an ill defined calcific lesion near the periosteum of lower femur medially with mild periosteal reaction [Table/Fig-1]. CT of right thigh showed a well defined soft tissue lesion with calcification in vastus medialis [Table/Fig-2] which on guided aspiration showed numerous RBCs along with clusters of histiocytes with occasional calcified specs seen without presence of granulomas.
X-ray of right thigh showed an ill defined calcific lesion near the periosteum of lower femur medially with mild periosteal reaction
CT showed a well defined soft tissue lesion with calcification in vastus medialis


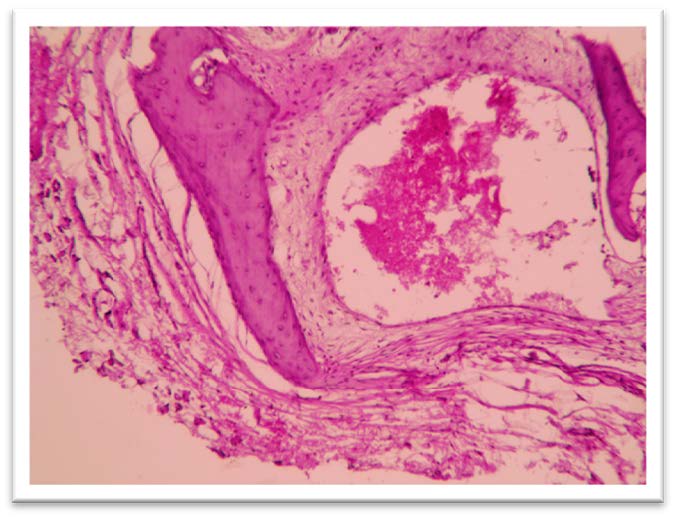
Patient’s blood picture was normal. Excision biopsy was done under spinal anaesthesia. Longitudinal skin incision made over the medial aspect of lower third of thigh and incision deepened in layers. Vastus medialis exposed and split along the line of fibres. A hard oval shaped swelling of about size, 3 x 2 cm found in the intramuscular location adherent to the surrounding tissue. Swelling excised and sent for histopathological examination [Table/Fig-3]. Postoperative period was uneventful. Histopathology was consistent with intramuscular cavernous haemangioma with ossification [Table/Fig-4].

Histomicroscopic magnification showed intramuscular haemangioma with ossification
Discussion
Haemangiomas are benign vascular tumour which is more common in infancy [1]. Common sites are skin and mucosa. Intra muscular haemangioma are rare which constitutes 0.8% of all haemangiomas. It may ossify due to dystrophic calcifications (25%) which is more commonly seen in cavernous type [2,3].
Haemangiomas are slow growing tumours which may get accelerated by growth spurt and trauma [4,5]. Malignant transformation is very rare [6,7]. About 94% of patients aged less than 30 years [8]. It is more common in females [9,10]. In intramuscular haemangiomas lower limbs are more commonly involved (42-45%) [4,8] and history of trauma is uncommon (17%) [8].
Clinically patients presents with pain (55%) [8] and swelling of duration ranging from 1-5 years. The swelling is usually palapable (98%). It presents as firm fluctuant mass which moves perpendicular to the line of muscle fibres. It may be pulsatile or bruit on auscutation. Skin over the swelling may have purpuric discolouration or dilated veins [11].
Dong et al., reported a similar case presented as myofascial pain syndrome which was initially treated with intramuscular electrical stimulation, acupuncture, intramuscular lidocaine and failed to alleviate symptom. After imaging studies intramuscular haemangioma was diagnosed and patients symptoms resolved after surgical excision [12].
Iftikar et al., reported another similar case presented with stiffness of knee joint and was treated with wide local excision [13]. Krithika et al., presented with a strange pain in masseter which later diagnosed as intra muscular haemangioma and cured with surgical excision [14]. Khodamorad et al., reported an intramuscular haemangioma in thigh with presented with extension contracture and thigh mass [15].
On imaging studies such as x ray shows calcifications along with increased periosteal reactions are also observed [2,3]. Typically intramuscular haemangiomas shows swiss cheese appearance which is formed due to presence of cavernous veins in between the ossified component. In contrast to that, Swiss-cheese-like appearance was not present in our case but an ill defined calcification was seen. Colour Doppler study shows intratumoural hypervascularity [15,16].
MRI is the investigation of choice which shows a mass of intermediate signal intensity with a fairly well-delineated margin on T1WI and high signal intensity on T2WI [16] Contrast-enhanced MRI shows serpentine or lattice like enhancement of the lesions [17].
As in our case computed tomography (CT) scan of ossified intramuscular haemangioma shows irregular increased density throughout the lesion, compatible with the ossification within the lesion. Decreased density may also be found around the lesion, indicative of the peritumoural fat attenuation. Post-contrast CT may fail to further enhance the lesion [2]. Arteriography may be needed to study communication with major vessels [15].
Differential diagnosis is myositis ossificans, early extraskeletal osteosarcoma, synovial sarcoma. Radiologically they are differentiated by zonal phenomenon in myositis ossificans which have calcifications in periphery and varies depending on the age of the lesion. Osteosarcoma have central ossifications, synovial sarcoma have stippled amorphous calcifications and haemangioma has central hypoechoic solid mass with peripheral hyperechoic fat and scattered hyperechoic ossifications [2].
Complications mainly in case of huge haemangiomas which causes compression to surrounding vital structures, cardiac complications if arteriovenous shunting is present and increased consumption of coagulation factors leads to consumptive coagulopathy (kasabach-meritt syndrome [18].
Excision is the treatment of choice with recurrence of about 9-28% due to infiltrating growth pattern [13–15]. RA Brown et al., reported a case successfully treated with repeated injections of sclerosants which couldn’t be surgically excised [19]. Sclerotherapy using STS, ethanol, hypertonic saline, sodium morrhuate or by using foamed sclerosants is indicated when excision is not possible i.e. when the lesion is too large; to reduce the bulk and when the patient is not willing for surgery [20]. Radiotherapy, holmium and YAG laser ablation, arterial embolization, and cryosurgery are the other modes of treatment available, Systemic corticosteroid therapy was found to be unsuccessful by Edgerton et al., [21].
Conclusion
In any unexplained deep seated intramuscular swelling with pain in a young adult, intramuscular haemangioma has to be included in the differential diagnosis. It must be investigated with MRI which is the investigation of choice and can be cured with surgical excision which is the treatment of choice.
[1]. Ly JQ, Sanders TG, Mulloy JP, Osseous change adjacent to soft-tissue hemangiomas of the extremities: correlation with lesion size and proximity to boneAJR Am J Roentgenol 2003 180:1695-1700. [Google Scholar]
[2]. Nagira K, Yamamoto T, Marui T, Akisue T, Yoshiya S, Kurosaka M, Ossified intramuscular hemangioma: multimodality imaging findingsClin Imaging 2001 25:368-72. [Google Scholar]
[3]. Enzinger FM, Weiss SW, Benign tumors and tumor like lesions of blood vesselsIn: Soft Tissue Tumors 1995 St Louis, MOCV Mosby Co:579-626. [Google Scholar]
[4]. Shallow TA, Eger SA, Wagner FB, Primary hemangiomatous tumors of skeletal muscleAnn Surg 1944 119:700-04. [Google Scholar]
[5]. Terezhalmy GT, Riley CK, Moore WS, Intramuscular hemangiomasQuintessence Int 2000 31:142-43. [Google Scholar]
[6]. Narayanan C. D., Prakash P., Dhanasekaran C. K., “Intramuscular hemangioma of the masseter muscle: a case report,”Cases Journal 2009 vol. 2(no. 5)article 7459 [Google Scholar]
[7]. Moser RP, Barr MS, Musculoskeletal case of the day. Intramuscular hemangioma of the thighAJR Am J Roentgenol 1994 162:1465-66. [Google Scholar]
[8]. Jenkins HP, Delaney PA, Benign angiomatous tumors of skeletal musclesSurg Gynecol Obstet 1932 55:464-80. [Google Scholar]
[9]. Jiang TT, Cisa J, Desai P, Intramuscular ossified hemangiomaSkeletal Radiol 1995 24(7):538-40. [Google Scholar]
[10]. Allen PW, Enzinger FM, Hemangioma of skeletal muscle, an analysis of 89 casesCancer 1972 29:8-22. [Google Scholar]
[11]. Ferguson IL, Hemangiomata of skeletal muscleBr J Surg 1972 59(8):634-37. [Google Scholar]
[12]. Dong Hwee Kim, Miriam Hwang, Yoon Kyoo Kang, In Jong Kim, Yoon Kun Park, Intramuscular Hemangioma Mimicking Myofascial Pain Syndrome: A Case ReportJ Korean Med Sci 2007 22:580-2.ISSN 1011-8934 [Google Scholar]
[13]. Iftikhar W, Bhat MS, Basit S, Khursheed O, Jan M, Kawoosa AA, Intramuscular haemangioma of vastus lateralis presenting as stiffness of knee in an adolescent patientOA Orthopaedics 2014 18(2)(1):2 [Google Scholar]
[14]. Lakshmi Krithika Chandrasekar, Sankarapandiyan Sathasivasubramanian, Mohanarangam Venkata Sai Pulivadula, Intramuscular Haemangioma with Diagnostic Challenge: A Cause for Strange Pain in the Masseter Muscle Volume 2014 Article ID 285834 [Google Scholar]
[15]. Khodamorad Jamshidi, Dawood Jafari, Mehdi Ramezan Shirazi, Alireza Pahlevansabagh, Tina Shoushtaryzadeh, An Unusual Presentation of Ossified Intramuscular Hemangioma:A Case ReportActa Medica Iranica 2014 52(4):319-22. [Google Scholar]
[16]. Wook Jin, MD, Gou Young Kim, MD, Jae Hoon Lee, MD, Dal Mo Yang, MD, Hyun Cheol Kim, MD, Ji Seon Park, MD, Kyung Nam Ryu, MD, Intramuscular Hemangioma With Ossification Emphasis on Sonographic FindingsJ Ultrasound Med 2008 27:281-85. [Google Scholar]
[17]. Greenspan A, McGahan JP, Vogelsang P, Szabo RM, Imaging strategies in the evaluation of soft-tissue hemangiomas of the extremities: correlation of the findings of plain radiography, angiography, CT, MRI, and ultrasonography in 12 histologically proven casesSkeletal Radiol 1992 21:11-18. [Google Scholar]
[18]. Wani IH, Bhat MS, Basit S, Khursheed O, Jan M, Kawoosa AA, Intramuscular haemangioma of vastus lateralis presenting as stiffness of knee in an adolescent patientOA Orthopaedics 2014 8:2(1):2 [Google Scholar]
[19]. Brown R A, Crichton K, Malouf G M, Intramuscular haemangioma of the thigh in a basketball playerBr J Sports Med 2004 38:346-48.doi: 10.1136/bjsm.2003.004671 [Google Scholar]
[20]. Chawla Y, Dilawari J, Studies in sclerotherapy.1. Comparison of sodium tetradecyl sulphate with absolute alcohol as sclerosants in the treatment of esophageal varicesJ Clin Gastroenterol 1990 12:378-80. [Google Scholar]
[21]. Edgerton MT, The treatment of hemangiomas: with special reference to the role of steroid therapyAnn Surg 1976 183:517-32. [Google Scholar]