Oral disease usually manifests as one of the following: (1) change in colour; (2) swelling; (3) ulcers; (4) ulceroproliferative; (5) vesiculo-bullous or (6) surface textural changes [1–3]. Critical understanding of these parameters is very essential in the diagnostic process. The word swelling denotes any enlargement or protuberance over the body surface [2]. The swellings of oral cavity may be classified as a sessile or pedunculated based on the type of junction of the lesion with underlying tissue. Based on the anatomical origin the swellings may also be classified as central and peripheral lesions. The exophytic lesions may present either as intra-osseous/central or extra-osseous/peripheral [4]. The term oral exophytic lesions represent any pathological growth that projects above the normal contours of the oral surface epithelium [5]. Exophytic lesions are often difficult to diagnose clinically, due to the varied pathogenesis of the diseases and there by yielding diagnostic challenge. Exophytic appearance often provides a greater chance of misdiagnosis as malignant lesions [6].
Methodology
Study eligibility criteria: We conducted a comprehensive literature search in the PubMed database using related MeSH keywords for the previously published papers between January 1980 and March 2015. We first conducted the search using “Oral exophytic lesions.” The resulting number of literature count was 138 articles. Further search with words “Oral cavity AND exophytic lesions” showed 82 published papers. Out of 220 published papers, only three studies have been found with an attempt of classification, and 63 full text papers were found. These yielded a total of 66 published papers, which were brought to our consideration, for devising a classification system on Oral exophytic lesions.
Studies were included if they meet the following criteria: (1) observational studies including cross-sectional studies and case reports in PubMed database; (2) full text availability of the papers in PubMed database and; (3) articles written in English language and published in PubMed database. Articles those did not meet our inclusion criteria are excluded.
Recommendation for the classification system: The previous classification systems were focusing on: (1) Soft tissue exophytic lesions; (2) Exophytic lesions in HIV disease and; (3) Exophytic metastatic lesions of the oral cavity [6–8]. Based on our literature search, it was noted that, classification of oral exophytic lesions of the oral cavity have not been organized as a separate group. Hence, present manuscript attempted to classify the oral exophytic lesions based on the: (1) Nature of the pathology; (2) Relation to the bone proximity and; (3) Histological basis.
Justifying the need for the study: Zain et al., report of National Epidemiological Survey of Oral Mucosal Lesions in Malaysia mentioned the frequency of the exophytic oral lesions as 25.8% [9]. It is also identified that isolated case reports of various exophytic lesions of the oral cavity have been published from time to time. Javad et al., suggested that histopathological diagnosis of exophytic lesions is influenced by clinical, radiographic diagnosis and surgeons’ observation during biopsy. The later mentioned study justifies the basis of clinico-pathological importance in diagnosis. Based on results from Javad et al., it was identified that 81.7% of clinical diagnosis was consistent with histopathological diagnosis and 18.3% cases were not consistent with clinical diagnosis. Their study focused on the consistency rate of diagnosis of various oral soft tissue exophytic lesions and also stated that clinical diagnostic agreement of verruca vulgaris, verrucous carcinoma, peripheral giant cell granuloma and squamous cell carcinoma was varied and further stated that above mentioned lesions carries a diagnostic challenge [10].
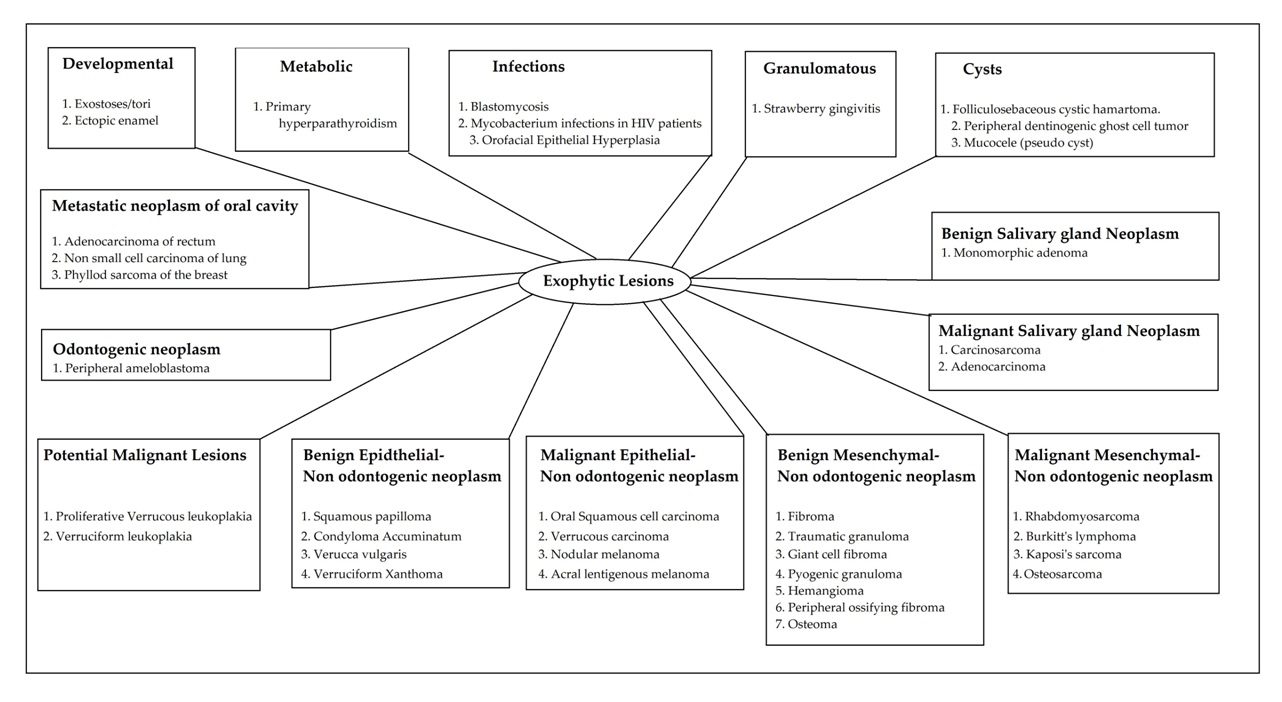
Approach to classification of oral exophytic lesion in the present paper is very straight forward due to the simple clinical/histological parameters, which will aid in easy clinico-pathological understanding. The parameters considered in the present classification system are designed to focus on clinico-pathological elements and that includes: (1) Origin/nature of pathology; (2) Location of the lesion (peripheral/central) and; (3) Type of histological structure (epithelium/mesenchyme). The origin/nature of the pathology includes developmental, metabolic, infectious, granulomatous, cystic (true and pseudo), potentially malignant disorders and neoplasias (benign, malignant and metastasis).
Criteria for clinicopathological understanding of Oral exophytic lesions: Our first approach in classifying oral exophytic lesions is based on the Origin/nature of the pathology [Table/Fig-1], the second approach was based on Location [Table/Fig-2] and third approach was based on the type of histological structure [Table/Fig-3] in the exophytic lesion. Additionally second classification system is proposed based on the aetiology of the lesion [Table/Fig-4]. Classification approaches based on origin/nature of pathology and location was given higher priority in discussion due to the better explainability of clinico-pathological descriptors specifically peripheral or central lesions.
Classification system 1 and Approach 1: Oral exophytic lesions based on Origin/nature of pathology
Classification system 1 and Approach 2: Oral exophytic lesions based on Location of pathology
| No. | Peripheral (Extraosseous) and Central (Intraosseous) case definition | Examples. |
|---|
| 1 | Extra-osseous/Peripheral lesions:- Due to the excessive proliferation of the epithelial or mesenchymal tissue. | Enamel pearls, Dens evaginatus, Blastomycosis, Mycobacterium infections in HIV, Focal epithelial hyperplasia, Wegner’s granulomatosis, Folliculosebaceous cystic hamartoma, Peripheral dentinogenic ghost cell tumour, Mucus retention pehnomenona, Proliferative verrucous leukoplakia, Verruciform leukoplakia, Squamous papilloma, Verruca vulgaris, Condyloma accuminatum, Oral squamous cell carcinoma, Verrucous carcinoma, Melanoma, Ductal papilloma, carcinoma Ex pleomorphic adenoma, Fibrous nodule, Traumatic granuloma, Giant cell fibroma, Pyogenic granuloma, Haemangioma, Rhabdomyosarcoma, Periosteal osteoma, peripheral ossifying fibroma, Paraosteal osteosarcoma, Peripheral ameloblastoma, Peripheral odontogenic fibroma. |
| 2 | Intra-osseous/central lesions:- Due to the cortical plate thickening and swelling, this results in surface elevation.- Osteolytic activity of the lesion may lead to protruding out of the surface. | Exostoses, Giant cell tumour, Burkitt’s lymphoma and Metastatic neoplasm. |
Classification system 1 and Approach 3: Oral exophytic lesions based on the Histological structure. (origin/nature of pathology and clinical character of the lesions are included for clinico-patholgical correlation)
| No. | Origin/Nature of the pathology | Lesions | Clinical character | Histological structure |
|---|
| 1 | Developmental | Exostoses/tori | Nodular and hard | Intraosseous |
| Ectopic Enamel | Nodular and hard | Peripheral(based on theectodermalorigin of theenamel) |
| Dens evaginatus | Nodular and hard | Peripheral(based on theectodermalorigin of theenamel) |
| 2 | Metabolic | Primaryhyperparathyroidism | Exophytic, sessile,firm to hard swelling,and reddish brown incolour | Intraosseous |
| 3 | Infectious | Blastomycosis | Exophytic appearance,irregular rolledborders andsometimes surfaceulcerations. | Peripheral |
| Rhinosporidiosis | Lobulated, fungatingand exophytic growth. | Peripheral |
| MycobacteriumInfections in HIV | Exophyticproliferativeulcerations. | Peripheral |
| FocalEpithelialHyperplasia | Broad based, exophytic, multiplelesions, familialhistory, early onset in life. | Peripheral |
| 4 | Granulomatous | Straw berryGingivitis | Numerous shortbulbous projections ofgingiva givingexophytic appearance | Peripheral |
| 5 | Cysts | True cyst | FolliculosebaceousCystic Hamartoma | Exophytic papule ofinvolved surface | Peripheral |
| Peripheraldentinogenic GhostCell Tumour | Nodular,sessile/peduncularmass over gingiva | Peripheral |
| Pseudo cyst | Mucocele | Pedunculated,exophytic swelling | Peripheral |
| 6 | Potentially malignant lesions | Proliferative VerrucousLeukoplakia | Exophytic and verrucous | Peripheral |
| VerruciformLeukoplakia | Exophytic, sharp andpointed surface lesion. | Peripheral |
| 7 | Neoplasia | Benignepithelialneoplasm(nonOdontogenic) | Squamous Papilloma | Pedunclated, exophytic | Peripheral |
| Condyloma Accuminatum | Broad based, exophytic, multiplelesions. Usually assocated with genitallesions | Peripheral |
| Verucca Vulgaris | Broad based, exophytic | Peripheral |
| Nevus | Palpable and sometimes raised | Peripheral |
| Verruciform Xanthoma | Broad based, exophytic. | Peripheral |
| Papillary Hyperplasia | Multiple projections, erythematous. | Peripheral |
| MalignantEpithelialneoplasm(Nonodontogenic) | Oral squamous Cell Carcinoma | Exophytic, indurated, white and red areas inswelling | Peripheral |
| Verrucous Carcinoma | Broad base exophyticswelling and presenceof thick white keratin. | Peripheral |
| Nodular Melanoma | Persistent, palpableraised lesion. |
| Acral LentigenousMelanoma |
| Benign Softtissueneoplasm(Nonodontogenic) | Fibroma | Nodular, fixed tosurface mucosa | Peripheral |
| Lipoma | Exophytic,Compressible,encapsulated, yellowin colour | Mesenchymalorigin(Fibrous tissue) |
| Traumatic Granuloma | Vascular, fixed to mucosa. | Peripheral(Mesenchymal origin) |
| Giant cell fibroma | Nodular, occurs ongingiva or attachedalveolar mucosa | Peripheral Mesenchymal– (Fibrous tissue) |
| Pyogenic granuloma | Exophytic, ulcerated,swelling and bleeds easily. | Peripheral |
| Haemangioma | Compressible,exophytic, pulsatile,red colour swelling. | Peripheral |
| Lymphangioma | Diffuse, exophytic,compressible swelling. | Peripheral |
| Rhabdomyosarcoma | Well circumscribed,exophytic, submucosalswelling and fixed tomuscle. | Peripheral,MesenchymalOrigin(Muscle tissue) |
| Burkitt’s lymphoma | Lobulated, exophyticgrowth. Palpable hardlymphnodes. | IntraosseousMesenchymalOrigin(Muscle tissue) |
| Kaposi’s sarcoma | Exophytic, lobulated,red coloured lesion. | Mesenchymal(Muscle tissue) |
| Benignosseousneoplasm | Peripheral OssifyingFibroma | Usually occurs overgingiva or attached tomucosa, exophytic, firm mass. | Peripheral |
| Osteoma | Exophytic, bony hard swelling. | Peripheral |
| MalignantOsseousneoplasm | Osteosarcoma | Exophytic, bony hardswelling associated with pain. | Peripheral (extraosseousvariant of central origin) |
| BenignOdontogenicNeoplasm | PeripheralAmeloblastoma | Sessile or pedunculatedexophytic growth often withoutulceration | Peripheral |
| Malignantneoplasm ofsalivaryglands | Carcinosarcoma | Exophytic mass,varied presentations | Peripheral (Glandular origin) |
| Adenocarcinoma | Exophytic growth,pain is usually absent. | Intraosseous |
| Metastaticneoplasms ofJaw bonss | Adenocarcinoma of rectum,Non small cell carcinoma of lung,Phyllod sarcoma of the breast | Exophytic with orwithout ulcerations. |
Classification System 2: Oral exophytic lesions based on Aetiology
| 1. Structural or Developmental disturbances: |
| a. Exostoses |
| b. Enamel pearls |
| 2. Smoking/Tobacco or other Deleterious habit related: |
| a. Proliferative verrucous leukoplakia |
| B. Verruciform leukoplakia |
| c. Oral squamous cell carcinoma |
| d. Verrucous carcinoma |
| 3. Trauma |
| a. Fibrous nodule |
| b. Traumatic granuloma |
| c. Giant cell fibroma |
| 4. Altered Sexual Practices: |
| a. Condyloma Accuminatum |
| 5. Infection: |
| a. Blastomycosis |
| b. Mycobacterium Infections in HIV |
| c. Focal epithelial hyperplasia |
| d. Squamous papilloma |
| e. Verruca vulgaris |
The peripheral lesions can be either surface epithelial lesions or mesenchymal tissues that are immediately subjacent to the epithelium and which excludes osseous and/or marrow derived tissue. The exophytic nature in the peripheral category is due to the excessive proliferation of the: (1) Epithelial tissue (examples: Squamous papilloma, Verruca vulgaris, Squamous cell carcinoma, etc.,) or; (2) From the mesenchymal tissue (examples: haemangioma, periosteal osteoma, paraosteal osteosarcoma).
Central lesion takes origin from either: (1) bone or marrow tissues (Examples: exostoses, giant cell tumour, burkitt’s lymphoma, metastatic bone tumours of jaw) or; (2) Any growth that are identified primarily in the bone (Examples: intraosseous squamous cell carcinoma, muco-epidermoid carcinoma). Although the central lesions are specifying to the intra-osseous nature (in the bone) it may have exophytic nature due to two reasons: (1) The thickening and swelling of the cortical plate may cause the elevation of the surface and resulting in the exophytic nature of the lesion, and; (2) the osteolytic activity leading lesional tissue to protrude out of the surface and resulting in the exophytic nature of the lesion [11,12].
Discussion of The Classified Lesions
First classification system
A large number of exophytic lesions may affect the oral cavity and based on the origin of the oral exophytic lesions it may be classified into developmental, metabolic, infectious, granulomatous, cystic, or neoplastic [Table/Fig-1]. The developmental origin of oral exophytic lesions include exostoses/tori, and enamel pearl/ectopic enamel. The metabolic origin of oral exophytic lesions includes primary hyperparathyroidism. The infectious origin of oral exophytic lesions are blastomycosis, mycobacterium infections in HIV patients, oro-facial epithelial hyperplasia and Rhinosporidiosis. Granulomatous origin of oral exophytic lesion is Wegener’s granulomatosis. The cystic lesions that display oral exophytic features are folliculosebaceous cystic hamartoma, mucus retention phenomenon and peripheral dentinogenic ghost cell tumour. Premalignant lesions that show the exophytic growth are proliferative verrucous leukoplakia and verruciform leukoplakia. Neoplastic lesions that demonstrate the exophytic growth could be sub categorized based on the tissue origin of tumours such as: (1) benign salivary gland tumours (monomorphic adenoma and ductal papillomas); (2) malignant salivary gland tumours (adenocarcinoma); (3) benign epithelial neoplasm of non odontogenic tissue origin (Squamous papilloma, condyloma accuminatum, verruca vulgaris and verruciform xanthoma); (4) Malignant epithelial neoplasm of non odontogenic tissue origin (oral Squamous cell carcinoma, verrucous carcinoma, nodular melanoma, and acral lentigenous melanoma); (5) Benign mesenchycmal neoplasm of non-odontogenic tissue origin (fibroma, traumatic granuloma, giant cell fibroma, pyogenic granuloma, Haemangioma, peripheral ossifying fibroma, and osteoma); (6) malignant mesenchymal neoplasm of non-odontogenic tissue origin (Rhabdomyosarcoma, Burkitt’s lymphoma, Kaposi’s sarcoma, and osteosarcoma); (7) Benign odontogenic neoplasm (peripheral ameloblastoma) and; (8) Metastatic neoplasm of jaw bone (adenocarcinoma of rectum, non small cell carcinoma of lung, phyllod sarcoma of the breast.
Second classification system: The aetiology based classification [Table/Fig-4] for oral exophytic lesions includes structural or developmental disturbances (exostoses and enamel pearls), smoking/tobacco related habits (proliferative verrucous leukoplakia, oral Squamous cell carcinoma and verrucous carcinoma), trauma-induced (fibroma, traumatic granuloma, giant cell fibroma), associated with altered sexual practices (condyloma accuminatum), and infections (Blastomycosis, mycobacterium infections in HIV, focal epithelial hyperplasia, and verruca vulgaris).
Peripheral exophytic growth
Enamel Pearls: Peripheral exophytic growth originated from developmental disturbance condition and characterized by ectopic presence of enamel at the furcation area of the multi-rooted tooth. The ectopic enamel gives an exophytic appearance and usually identified on maxillary and mandibular second molars [13,14]. The lesion may not be seen clinically due to its location at root furcation; and the lesion have a tendency to predispose to periodontal tissue breakdown [15,16].
Dens Evaginatus: Peripheral exophytic growth originated from developmental disturbance condition of dental structure and is characterized by the hard, cusp/tubercle projecting out of the tooth surface [17].
Blastomycosis: Peripheral exophytic growth caused due to the fungal infection. The exophytic appearance of the lesion is characterized by irregular rolled borders and sometimes surface ulcerations. The infection induces the reactionary proliferation of epithelial tissue, called as pseudoepitheliomatous hyperplasia and hence gives an exophytic appearance clinically. The exophytic appearance of the lesion often mimics Squamous cell carcinoma (SCC) clinically and histologically [14,16].
Mycobacterium Infections in HIV: Peripheral exophytic growth originated from mycobacterium in HIV infection. The oral lesions may be presented as exophytic proliferation, ulceration and granular leukoplakia areas [4,18,19].
Focal Epithelial Hyperplasia: Peripheral exophytic growth originated from Human papilloma virus (HPV 13 and 32) infection and characterized by proliferation of oral squamous epithelium. Clinically, it is often identified as multiple, soft, round papules from the surface epithelium, giving appearance of exophytic and commonly involving labial and buccal mucosa. Histologically due to the epithelial proliferation, the thickened portion of epithelium extends upwards and not downwards which gives the appearance of exophytic nature of the lesion. Exophytic appearance of the lesion often mimics papillomas or condylomas [20–22].
Wegener’s Granulomatosis: Peripheral exophytic growth of granulomatous origin and is usually seen on gingival surface. The gingival surface of patients with wegener’s granulomatosis often depict granular hyperplasia, often showing numerous short bulbous projections, giving an exophytic appearance to the lesion and haemorrhagic areas [6]. The clinical appearance of the above mentioned description is termed as strawberry gingivitis. Histologically due to the pseudoepithelomatous hyperplasia of the involved keratinized stratified squamous epithelium and lobular surface gives the appearance of exophytic nature of the lesion [23,24].
Folliculosebaceous Cystic Hamartoma: It is a rare cutaneous hamartoma and only one case has been identified in the literature search and 39 cases of the mucocutaneous folliculosebaceous cystic hamartomas has been reported. Based on the epithelial structure involvement in the exophytic growth, the lesion is considered to be peripheral category of exophytic lesion. Mohammed Nadimul et al., reported a case with upper lip and labial mucosal involvement. Histologically due to the hyperplasia of the follicular structures, sebaceous and accessory salivary glands the clinical appearance of exophytic nature of the lesion is noted [25].
Peripheral Dentinogenic Ghost Cell Tumour: Peripheral exophytic growth which usually manifests as a nodular, sessile or pedunculated mass over the gingival tissue. The nodular growth over the gingival gives the appearance of exophytic lesion. It is often misdiagnosed for epulis, fibromas and peripheral giant cell granulomas [26–28].
Mucus retention phenomenona: This condition is usually trauma induced and presented as a dome shaped and sessile swellings, rarely it may be presented as an exophytic and pedunculated swelling. Lesion is classified under peripheral category due to the salivary gland ductal epithelial involvement. The exophytic lesions are more common on ventral and anterior part of the tongue due to the involvement of Blandin-Nuhn salivary glands and often seen commonly in females and in second decade of the life [29]. Due to the uncommon clinical location, exophytic appearance, it may be not diagnosed as mucoceles [30].
Proliferative Verrucous Leukoplakia: Peripheral exophytic growth of pre-malignant disease type and characterized by the irregular surface of the epithelium [31,32]. Histologically due to the epithelial proliferation gives the appearance of the exophytic nature of the lesion.
Verruciform leukoplakia: Some of the leukoplakic lesions presents as a sharp, pointed, exophytic appearance and are termed either verruciform or verrucous leukoplakia. Lesion is classified under peripheral exophytic growth category due to the surface epithelial involvement and irregular growth. It is often difficult to differentiate with the early verrucous carcinomas [4,33,34]. Histologically due to the papillary growth of the surface epithelium gives an exophytic appearance to this lesion.
Squamous Papilloma: Viral induced peripheral growth commonly identified as exophytic, pedunculated, finger like surface projections of the epithelium. Histologically, epithelial proliferation in finger/papillary pattern is a reason for exophytic appearance [35,36].
Verruca Vulgaris: Viral induced peripheral exophytic growth clinically characterized by painless, rough, white, papillary, exophytic, pedunculated or sessile growth. Histologically, the lesion is identified as hyperplastic epithelium and arranged in a finger like projection and the epithelial rete- pegs tend to converge towards the center of the lesion [4,37,38]. The reason for the clinical and histological appearance of exophytic growth of the lesion is similar to Squamous papilloma. Clinically, verruca vulgaris have a broad base; this feature is helpful to distinguish from Squamous papilloma.
Condyloma Accuminatum: Peripheral growth usually identified as an exophytic appearance and often transmitted to oral cavity due to oral sexual practices [35,39,40]. The reason for the clinical and histological appearance of exophytic growth of the lesion is similar to Squamous papilloma.
Oral squamous Cell Carcinoma: The exophytic cases of the Oral squamous cell carcinoma are represented as a irregular surface, fungating and verruciform growth and often ulcerated with indurated borders and colour may vary from red to white areas [41,42]. The lesion is categorized as peripheral growth due to the epithelial origin.
Verrucous Carcinoma: Peripheral exophytic growth of neoplastic origin and it is clinically characterized by diffuse, exophytic, veruciform, and whitish appearing lesion. The exophytic appearance and of the lesion is due to the hyperplastic epithelium [43,44].
Melanoma: Peripheral exophytic and malignant growth are usually seen in acral lentigenous and nodular variants of melanoma. Clinically brown-black macules may extend to give exophytic appearance [45]. The macule may extend and gives the exophytic appearance. Kumar et al., in their clinicopathological series of four oral melanomas suggested that, nodular form of melanoma presented with exophytic and ulcerated lesion [46].
Ductal Papilloma: Clinical presentation of this benign neoplastic lesion is usually identified as an exophytic and/or papillary growth [47]. Brannon et al., mentioned that ductal papillomas are characterized by biphasic growth pattern of exophytic and endophytic components [48]. The lesion is categorized as peripheral growth due to the salivary gland ductal origin.
Carcinoma ex Pleomorphic adenoma: Clinical presentation of this malignant salivary gland neoplasm of peripheral orign is usually identified as exophytic and ulcerated mass [4,49]. Adenocarcinoma: Song et al., in reported a case of adenocarcinoma with exophytic mass over right mandibular ramus [50].
Fibrous Nodule: It is a peripheral exophytic growth characterized by firm consistency on palpation and usually associated with trauma. The exophytic nature of the lesion is due to the increased fibrous tissue in the stroma [51].
Traumatic Granuloma: It is a peripheral and reactive oral mucosal condition often clinically characterized as exophytic ulcerated mass. Histological section shows slight epithelial hyperplasia and ulcer bed shows increased granulation tissue [52].
Giant Cell Fibroma: Clinical details of the lesion includes sessile or pedunculated nodule and often appears papillary and exophytic. This lesion is often mistaken with Squamous papilloma. The exophytic nature of the lesion is due to the increased fibrous tissue in the stroma [53,54].
Pyogenic Granuloma: It is tumour like exophytic growth of the oral cavity characterized by a smooth, lobulated mass and is usually pedunculated. The peripheral exophytic nature of the lesion is due to the hyperplastic epithelium and is often associated with inflammatory origin [55].
Haemangioma: The superficial haemangiomas are hamartomatous lesion and appears as fiery red coloured and clinically presented as an exophytic mass. However, Kai et al., reported a first case of central Haemangioma with an exophytic growth in maxillae [56].
Rhabdomyosarcoma: It is a peripheral exophytic growth of malignant mesenchymal tissue origin. The embryonal variant of rhabdomyosarcomas shows a polypoid and exophytic and growth tend to get fixed to surrounding tissues at an early stage [57,58].
Periosteal Osteoma: It is a benign neoplasm of bone and is characterized by polypoid, exophytic or sessile mass. It is also termed as an exophytic or peripheral osteomas. Histologically the lesion is composed of mature bone and the exophytic appearance is due to the increased mass of the osseous tissue [59]. The lesion is categorized as peripheral growth due to the extraosseous pattern of the growth.
Peripheral Ossifying Fibroma: This tumour is clinically identified as well circumscribed, pedunculated, exophytic growth and relatively common in gingival surface. The clinical presentation of the lesion is similar as giant cell fibroma and peripheral Odontogenic fibroma. Histologically, the lesion is characterized by fibrous proliferation with formation of mineralized component [60,61]. The exophytic appearance is due to the fibrous proliferation of the lesion and considered as peripheral growth due to its occurrence in gingival region.
Paraosteal Osteosarcoma: The paraosteal osteosarcomas presents as a firm swelling, exophytic growth with pain [62]. Paraosteal osteosarcomas are considered as peripheral growth due to the extraosseous pattern of the growth.
Peripheral Ameloblastoma: It is an uncommon variant of ameloblastoma and is characterized by an exophytic growth of the soft tissue. Clinical presentation is usually sessile or pedunculated exophytic growth at gingival or alveolar mucosal areas of the jaw and often without ulceration. The exophytic growth is due to the increased fibrous stroma with islands of ameloblastic epithelium and considered as peripheral growth due to its occurrence in the gingival/tooth bearing areas of the jaw [63].
Peripheral Odontogenic Fibroma: This lesion is clinically identified as firm, exophytic growth with normal mucosal colour. It is often difficult to distinguish with peripheral ossifying fibroma. The exophytic appearance is due to the increased collagen fibres in the lesion and considered as peripheral growth due to its occurrence in gingival region [64].
Intraosseous Exophytic growth - Exostoses: Intraosseous exophytic growth originated from developmental disturbance condition and characterized by localized bony protuberance from the cortical plate in maxillae or mandibular jaw. The lesion is commonly called as tori and are one of the most common form of oral exophytic lesions [65]. The nodular and lobular forms of the tori give clinical appearance of exophytic growth. Their size may be lesser than 2cm in diameter [66,67].
Giant cell tumour: Intraosseous exophytic growth originated from metabolic disturbance (hyperparathyroidism) and characterized by abnormal bone metabolism and often it is more commonly seen at posterior area of jaw bone. The osteolytic activity of the underlying disease mechanism predisposes the exophytic appearance of the lesion [68]. Punnya et al., reported an exophytic brown tumour in posterior right mandibular region [69].
Burkitt’s lymphoma: The oral presentation of this lesion often varies, and the cases have been described by lobulated and exophytic appearance of the tumour mass. Roseanna et al., reported a case of burkitt’s lymphoma presenting as a exophytic mass involving maxillary bones [70]. The lesion is considered as intraosseous due to the involvement of jaw bone.
Metastatic neoplasm: Metastic tumours such as Adenocarcinoma of rectum, non small cell carcinoma of lung, phyllod sarcoma of the breast were reported with exophytic presentation in the involved jaw bone (intraosseous growth) [10,71,72].
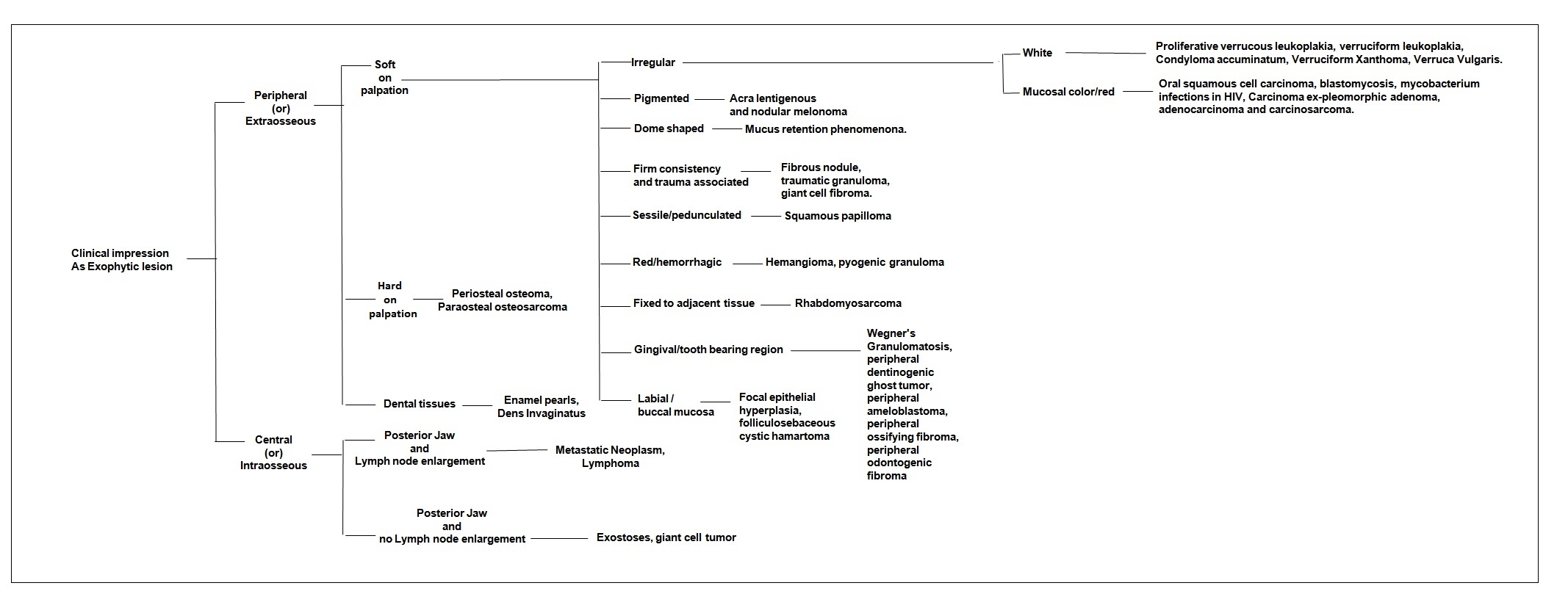
Decision Making Tree for Oral Exophytic Lesions
The information on clinical character and histological origin of the exophytic growth are two important parameters in decision making. The clinical characters such as consistency of the lesion (soft/hard), colour and pigmentation of the lesion, shape of the swelling, base of the exophytic growth, location of the lesion (anterior/posterior jaw; labial/buccal mucosa). Whereas, the histological origin of the growth such as bony, dental, gingival or epithelium. The obtained information should be analysed step by step for successful diagnosis of the lesion. Babu, Boyd, Kumaraswamy’s Decision making tree showed in the [Table/Fig-5] will be guiding the dental surgeons or diagnosticians to approach the oral exophytic lesions in step by step manner for obtaining clinical diagnosis. The present paper will be discussing various exophytic lesions under two categories, peripheral and central to accomplish easy understanding among readers. To achieve clinico-pathological understanding of documented oral exophytic lesions, clinical as well as histological details and its correlation to the exophytic nature of lesion is stated.
Babu, Boyd, Kumaraswamy’s Decision making tree for oral Exophytic lesions
Limitations of This Study
Classification systems are essential in medical and dental literature in order to provide a scientific understanding of disease of interest under aetiology, pathogenesis, clinical appearance, histological details or treatment of disease in an organized structure [73]. It is also imperative for a classification system to configure all those fore-mentioned areas in an integrated manner to provide a working and evidence based classification system to assist in diagnosis. The present classification system recognized those lesions that are available as research papers from PubMed data base. Further to this note, research papers assisted us in designing the evidence based classification but not satisfying a working based classification. This is because of the fact that some oral exophytic lesions were not included in the present classification system due to the limitation in the search criteria in the present study. The limitations of the present classification system may be due to the following reasons: (1) Lesions those are not published in the PubMed database; (2) Lesions that are published in PubMed database but do not have full text access; (3) Lesions that are published in PubMed database but not written in English language; and (4) Lesions that are documented in textbook resource, but not available in PubMed database. Any oral exophytic lesions from above four justified reasons are not included in the present classification and positioned us in a challenge of developing of fully integrated unified classification system. Future research papers or scientific committees are required to reframe or review the classification system and formulate a working and evidence based classification system in diagnosis of oral exophytic lesions.
Conclusion
The classification system for oral exophytic lesions was proposed to increase the clinico-pathological knowledge among dental surgeons or oral diagnosticians. Step by step approach of gathering information while clinical examination is important in the clinical diagnosis and the same is reinforced through decision making tree. Although decision making tree for oral exophytic lesions will be helpful in formulating working or provisional diagnosis, the final diagnosis should be made on the radiological and/or histological investigations. The present paper and classification model once again supports the importance of clinical and pathological evidences in formulating diagnosis.