Dry socket is the most common complication following a tooth extraction having peak incidence in the 40-45-year-old age group [1–3]. Most studies state that the incidence of dry socket is 1-4% for all routine dental extractions [4–7] and 5-30% for impacted mandibular third molar. Onset of Alveolar osteitis (AO) is 1–3 days after tooth extraction and duration usually ranges from 5 to 10 days [8]. During the last century, attempts have been made to find proper way for preventing AO and large number of clinical studies has been carried out of this clinically important topic [9–13]. Tranexamic acid, an antifibrinolytic agent impedes the proteolytic degradation of fibrin by preventing the attachment of plasminogen and plasmin [14]. A 4.8% solution has been proven to be very effective in reducing bleeding complications with negligible systemic absorption [15]. The antifibrinolytic agent tranexamic acid had been reputed to prevent AO when applied topically in the extraction socket following exodontias [16].
Despite the appealing attributes of this system and the fact that it has been used for local haemostasis enhancement after dental extractions for over decades, it has failed to gain widespread acceptance in the prevention of AO.
Considering all these therapeutic uses of this antifibrinolytic agent Tranexamic acid, a “Double blind study on the efficacy of tranexamic acid in the reduction of incidence of dry socket” is been undertaken.
Materials and Methods
The study is an institutional study conducted in Bangalore Institute of Dental Sciences, Bangalore extending for a period of 14 days postoperative the extraction phase. It is divided into 60 patients represented in [Table/Fig-1]. These patients underwent routine dental extractions of mandibular molar teeth. The inclusion criteria was young patients in the 2nd and 3rd decade of life; male and female patients (no sex differentiation); [Table/Fig-2], the dental extraction site and neighboring teeth should be free of infection and inflammation, be medically fit with no history of medications like antibiotics or any analgesics, with no history of any hypersensitivity reactions to the proposed medications including anaesthetics used in the study. The armamentarium is presented in [Table/Fig-3].
Age distribution of patients
| Age in years | Control | Treatment | Combined |
|---|
| No | % | No | % | No | % |
|---|
| 19-20 | 2 | 6.7 | 0 | 0.0 | 2 | 3.3 |
| 21-25 | 9 | 30.0 | 9 | 30.0 | 18 | 30.0 |
| 26-30 | 15 | 50.0 | 15 | 50.0 | 30 | 50.0 |
| 31-35 | 4 | 13.3 | 6 | 20.0 | 10 | 16.7 |
| Total | 30 | 100.0 | 30 | 100.0 | 60 | 100.0 |
| Mean ± SD | 26.43±3.86 | 27.70±3.44 | 27.07±3.67 |
Samples are age matched with p=0.184
Comparison of gender distribution between two groups
| Gender | Control | Treatment | Combined |
|---|
| No | % | No | % | No | % |
|---|
| Male | 22 | 73.3 | 11 | 36.7 | 33 | 55.0 |
| Female | 8 | 26.7 | 19 | 63.3 | 27 | 45.0 |
| Total | 30 | 100.0 | 30 | 100.0 | 60 | 100.0 |
p=0.004

In all the patients, medical history was obtained at the first visit and a standardized form was completed for each patient to record the relevant clinical data. Data recorded included patient age, gender, oral hygiene, tobacco smoking and use of oral contraceptives. Hygiene was scored with the simplified Oral Hygiene Index (OHI-S) as follows: good, 0 to 1.2; regular 1.3 to 3; and poor 3.1 to 6. Smoking was in turn coded as 1) non smoker 2) up to 10 cigarettes per day 3) 11 to 20 cigarettes per day and 4) more than 20 cigarettes per day. Oral contraceptives use was evaluated as either 1) yes 2) no. Each patient was signed informed consent as required by the institutional ethical clearance for this study. Bases on their occupation patients were grouped into lower, middle and high income groups.
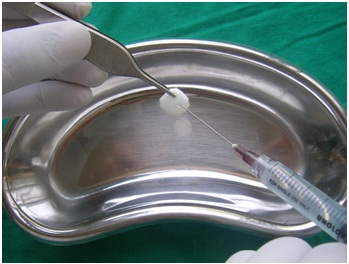
Collection of data: A double blind study was done in which Group A–30 out of 60 patients requiring routine dental extractions of mandibular teeth was randomly selected and was administered a dose of tranexamic acid orally (Pause 500mg) one hour prior to extraction of teeth. Gelfoam soaked in tranexamic acid (160mg) was placed into the extraction socket postoperatively as in [Table/Fig-4].
Gelfoam soaked with tranxenamic acid

A figure of eight silk suture was placed over the socket to secure the gelfoam. In the rest of the Group B – 30 patients, a placebo (crocin) was given orally one hour prior to the extraction and gelfoam soaked in saline was placed into the extraction socket postoperatively as in [Table/Fig-5]. A figure of eight silk suture was placed over the socket to secure the gelfoam. In all cases the inferior alveolar, lingual, and buccal nerves were anesthetized with 2ml cartridges containing 2% lignocaine with 1:200,000 adrenaline.
Gelfoam soaked with saline
Technique
One hour prior to extraction, orally either one of Group–A or Group–B, medication was given. Then, the mucoperiosteum was reflected to expose the bone and teeth were extracted using appropriate dental extraction forceps. Following extraction 1cc of either solution A (soaking gel foam with tranexamic acid) and solution B (soaking gelfoam with normal saline) were deposited on gelfoam and placed into the extraction socket and secured with a figure of eight silk suture. The sutures were removed during the patient 7th postoperative follow up.
Postoperative care: Patients were instructed to avoid rinsing for next 24 hours. Oral hygiene, maintenance was of vital importance. Patients were prescribed mild analgesics as required and asked to inform in case of bleeding, pain or discomfort. Patients were instructed to return on 3rd, 7th, 14th day to determine for dry socket by any increased severity of pain and loss of the blood clot with or without halitosis in the days following extraction.
Follow Up
For the purpose of this investigation, the diagnosis of dry socket was based on clinical symptoms rather than the appearance of dry socket. Pain was rated individually by each patient at 3rd, 7th, 14th day after extraction as in [Table/Fig-6,7 and 8]. As per study, any patient who reported severe pain and if the pain was not of a throbbing nature but was not relieved by ibuprofen, it was considered to be AO [17].
Efficacy of tranexamic acid on 3rd day postoperative
| Parameters | Control(n=30) | Treatment(n=30) | p-value |
|---|
| Pain | 18(60.0%) | 6(20.0%) | 0.002** |
| Dist.clot | 3(10.0%) | 3(10.0%) | 1.000 |
| Halitosis | 3(10.0%) | 2(6.7%) | 1.000 |
** Highly significant
Efficacy of tranexamic acid on 7th day postoperative
| Parameters | Control(n=30) | Treatment(n=30) | p-value |
|---|
| Pain | 12(40.0%) | 5(16.7%) | 0.045* |
| Dist.clot | 3(10.0%) | 2(6.7%) | 1.000 |
| Halitosis | 3(10.0%) | 1(3.3%) | 0.612 |
* significant
Efficacy of tranexamic acid on 14th day postoperative
| Parameters | Control(n=30) | Treatment(n=30) | p-value |
|---|
| Pain | 9(30.0%) | 2(6.7%) | 0.020* |
| Dist.clot | 2(6.7%) | 0 | 0.492 |
| Halitosis | 2(6.7%) | 0 | 0.492 |
* significant
Results
The overall result is interpreted in [Table/Fig-9]. In the study, out of 30 patients; 11 patients had complaint of one or other parameters seen as diagnostic criteria of dry socket i.e., 6 of the patient whose record showed time of onset of their complaint of pain had it by day 3 and 3 patients with disintegration of clot and 2 patients with halitosis. However, in the control group out of 30 patient 24 patients had complaints i.e., pain was seen in 18 of the patient, 3 patients with disintegration of clot and again 3 patients with halitosis in 3rd postoperative day, this seems to be comparatively on the higher side. Rest of the patient’s postoperative recovery was uneventful.
Overall comparison of control and treatment group.
| Parameters | Post-op day | Control(n=30) | Treatment(n=30) | p-value | Absolute riskreduction# | Risk Ratio |
|---|
| Pain | 3rd day | 18(60.0%) | 6(20.0%) | 0.002** | 0.40 | 0.33 |
| 7th day | 12(40.0%) | 5(16.7%) | 0.045* | 0.23 | 0.42 |
| 14th day | 9(30.0%) | 2(6.7%) | 0.020* | 0.23 | 0.22 |
| Dist. of clot$ | 3rd day | 3(10.0%) | 3(10.0%) | 1.000 | - | 1.00 |
| 7th day | 3(10.0%) | 2(6.7%) | 1.000 | 0.03 | 0.67 |
| 14th day | 2(6.7%) | 0 | 0.492 | - | - |
| Halitosis | 3rd day | 3(10.0%) | 2(6.7%) | 1.000 | 0.03 | 0.67 |
| 7th day | 3(10.0%) | 1(3.3%) | 0.612 | 0.07 | 0.33 |
| 14th day | 2(6.7%) | 0 | 0.492 | - | - |
# Percentage of absolute risk reduction of treatment when compared to control
$Disintegration of clot
Risk ratio <1: Less likely of risk in treatment
Risk Ratio>1: More likely of risk in treatment
Risk ratio=1 Equally likely between two groups
*significant
**Highly significant
At our routine seventh postoperative day recall appointment, we recorded for the same parameters on those same patients who had complaints on 3rd postoperative and found a marginal reduction i.e. 5 patients had complaint of pain, 2 patient with disintegration of clot, and 1 patient with halitosis in the treatment group in comparison to the control group which also showed improvement in relation to pain which was seen on 12 patients on seventh postoperative day follow up and there was no significant improvement with their socket condition in relation with disintegration of clot and halitosis.
Finally on our 14th day follow up we observed significant improvement on those same patients in the treatment group has only pain was seen in 2 patients with no other complaints like disintegration of clot and halitosis where as in control group 9 of the patients still complained of pain, 2 patient with disintegration of clot, 2 with halitosis. All these patients in the control group, treated with thorough irrigation using warm normal saline on alternate days until the socket granulates adequately. Pre operative antibiotics were not used and only analgesics were prescribed. As per study, Pain was rated individually by each patient at 3rd, 7th, and 14th day postoperatively in this study. The incidence of dry socket was found to be 6.66% among the patients administered tranexamic acid both orally and systematically and 30% among those who received no such treatment. Comparative analysis showed former to have comparatively less associated problems like disintegration of clot and halitosis, although the overall differences between the groups were not of much statistically significant. This study reveals favourable effect of tranexamic acid, given orally and applied topically.
Discussion
The full aetiology of AO is most particularly related to a complex interaction between excessive localized trauma, bacterial invasion and their association to plasmin and subsequently, the fibrinolytic system [18]. Prevention of AO entails reducing the number of possible risk factors, meticulous attention to procedural details and surgical skills. There are numerous compelling reasons not to fall into the trap of trying to compensate for a lack of surgical experience and unavoidable patient controlled factors by trying to place something in an alveolus to reduce the occurrence of a relatively minor complication. That approach had numerous potential disadvantages like-
The carrier material can potentially become a nidus for infection or foreign body reaction.
The carrier material can retard/delay healing or cause side effects [19].
The initiation of the fibrinolytic process appears to be related to an interfacing of multiple, interdependent factors, therefore, controlling any single factor attacks only part of the problem. When widely varying date are reported, using a wide array of different anitibiotics, antifibrinolytic agents and even plain rinses or basic oral hygiene, before, during and after surgery and all note improvement. It becomes apparent that many different factors are contributing to the problem [20].
Given that premise, there will be no universal solution found that addresses all of the factors. The key to management then becomes patient education, with a concurrent objective of reducing the incidence as much as possible through attention to procedural details and surgical skills. With the modern technology and knowledge available today, AO can be predictably confined to a small group of patients and those patients with identified risk factors can be easily forewarned to anticipate the minor complication [15]. Our purpose in this study was to overcome this minor complication by using this simple, inexpensive tranexamic acid both topically and systemically. Antifibrinolytic agents, when placed topically into the extraction site, have been shown to decrease the incidence of AO. As per study, the incidence of localized osteitis was 8% in the immediately packed sockets and 26% in the sockets that were not immediately packet [12]. Various results also showed that tranexamic acid impedes the proteolytic degradation of fibrin by preventing the attachment of plasminogen and plasmin and the solution has been proven to be very effective in reducing bleeding secondary to fibrinolysis of the wound clot [21].
At the end of this study the dispenser of the medicaments have revealed that the Control group contains (Tab. Crocin (placebo) orally 1 h prior + gelfoam soaked in saline placed at extracted socket and secured with figure of “8” suture and the Treatment group contains (tranexamic acid 500 mg orally 1h prior + gelfoam soaked in tranexamic acid placed at extracted socket and secured with figure of “8” suture). In this study comparison between the control group and treatment group was done clinically to determine the efficacy of tranexamic acid in the reduction of incidence of dry socket. The general health status of the patient may influence wound healing including extraction wounds and dry sockets. Thus patients with a medical condition or those on medications that are to know to affect healing were excluded in from the study.
The extractions were performed on routine basis and sites were free of infection. The variability may be due to differences in diagnostic criteria, intraoperative and postoperative treatment, patient age, medical status, surgical technique and skill, use of oral contraceptives, tobacco and alcohol consumption, feminine gender, among other factors. Similar to previous reports, a female preponderance was found in this study [21,22]. A statistically significant relationship was, however, not established genders in all patients who had extractions and those with dry sockets. The present age ranges in this study was between 19-35 years. However, this is in favour to claims that dry socket seldom or never occurs before the 18th or after the 50th year of life. The extractions and placement of medicaments were carried out by the same post graduate student during the study period. More patients with dry socket were in low and middle income groups [Table/Fig-10].

Expectedly, pain was the complain in all the patients. This was either associated with disintegration of clot and halitosis or presented individually. On the other hand, our patients had no problems associated with the use of intra-alveolar medicament placements, although cases of local sensitization, foreign body reactions, delayed healing, and neurosensory alterations have been described after the placement of different intra-alveolar preparations.
Pain was rated individually by each patient at 3rd, 7th, and 14th day postoperatively in this study [23]. Hence we clinically feel that this tranexamic acid produces a promoting action in preventing dry socket coinciding with the study by JM Sanchis and M Penarrocha based on criteria for dry sockets [5].
Thus it has been studied and reported that Tranexamic acid, an antifibrinolytic agent impedes the proteolytic degradation of fibrin by preventing the attachment of plasminogen and plasmin. Thereby, it promotes wound healing and prevents AO by reinforcing biological glue [24].
Though this study has been standardized to the maximum possible extent, it is humbly suggested that more studies with large samples are warranted, to evaluate the efficacy of this tranexamic acid to prevent AO when administered systemically and applied topically in the extraction socket following exodontia on a better scientific basis.
Conclusion
On the basis of this study, the continued use of tranexamic acid for the prevention of AO can be endorsed. The investigational material, tranexamic acid, not only did decrease the incidence of the condition but also appeared to contribute to the wound healing. The technique is safe and cost effective. However, the results of this study supports the conclusion that the use of tranexamic acid both locally and systemically following the removal of the teeth reduces the incidence of AO associated with the extraction of mandibular molars. Over all, tranexamic acid has several advantages also when used for simple dental extractions, namely: low cost and ready availability and therefore we recommend this treatment modality.
Samples are age matched with p=0.184
p=0.004
# Percentage of absolute risk reduction of treatment when compared to control
$Disintegration of clot
Risk ratio <1: Less likely of risk in treatment
Risk Ratio>1: More likely of risk in treatment
Risk ratio=1 Equally likely between two groups
*significant
**Highly significant