The SMARTPHONE is becoming an ever more common tool among oral and maxillofacial surgeons. Its role in patient care continues to evolve as the technology improves [1]. Smartphone (or Smart Phone) is a mobile telecommunication with an operating system. With a smartphone providing voice, text, multimedia message, GPS navigation unit, camera and e-mail options; members of a surgical team can communicate with each other [1].
Smartphones have inhabitant software known as an application (“app”). Of the current popular smartphone operating systems, each has a respective online “app store” to browse and download applications (i.e., BlackBerry App World, Android Market, Play Store, iPhone App Store/iTunes etc) [1]. Once downloaded, these images can be easily copied, viewed, archived, or electronically mailed (e-mailed) [2]. Because of these conveniences and the speed of response with smartphones, oral and maxillofacial surgeons frequently provide medical and dental opinion away from the bedside (such as in the case of outside referrals, emergency room and inpatient consults, transfer requests, or assistance) to residents, fellows, or the dental surgeons.
The aim of this paper was to review the literature on “Smartphone in Oral and Maxillofacial Surgery” online Pubmed database and elucidate its uses and capabilities with the following cases in the field of oral and maxillofacial surgery. Smartphones should be intended for use when time and location restrict the facility of maxillofacial surgeons to physically meet and engage in maxillofacial patient care. Consequently, a cost-effective immediate assessment of maxillofacial patients with the aid of smartphones can be undertaken.
Materials and Methods
A systemic search of the literature was carried out to identify the eligible articles at Bharati Vidyapeeth Dental College and Hospital, Pune from January 2015 to April 2015. The existing literature through the term “Smartphone in Oral and Maxillofacial Surgery” relevant to oral and maxillofacial surgery in online data-base of the United States National Library of Medicine: Pubmed (http://www.ncbi.nlm.nih.gov/pubmed/) was searched. The inclusion criteria was to review the published reports, abstracts and studies with clinical and evidence based reviews on “Uses of Smartphone in Oral and Maxillofacial Surgery”. The exclusion criteria were problems related with health, personality, ethical consent and shortcoming of the devices.
Since all the users registered with their phone numbers, the software synchronizes all the WhatsApp users in one’s contact and makes it easy to communicate with photographs and other files with the concerned persons. Consequently, electronic transmission of clinical and radiographic images for remote consultation was demonstrated using this technology with the following case series.
Case: 1
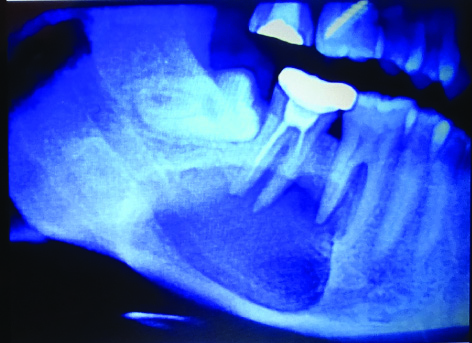
A 24-year-old female patient came to a dental surgeon with complain of pain in relation with lower right posterior tooth since 15 days. After proper history and clinical examination, patient underwent radiographic evaluation i.e. OPG (Orthopantomograph). OPG was then sent to the maxillofacial surgeon for further review and it showed the radiolucent lesion in relation with the lower first and second molar. In addition, there was an incomplete root canal treatment in relation to the mandibular second molar [Table/Fig-1].
Radiolucent lesion is associated with mandibular first and second molar in OPG
Case: 2
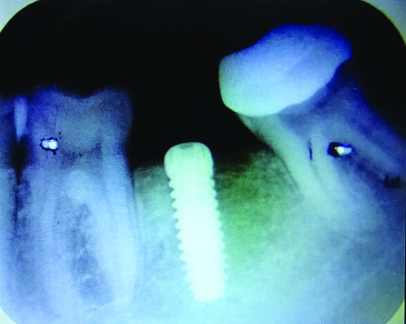
An implant was placed in lower mandibular second molar region after 2 years of postextraction. Post implant images were obtained after one day and e-mailed to the oral surgeon for review on his smartphone [Table/Fig-2].
Implant placement in mandibular second molar
Case: 3
A 45-year-old male patient presented to the dental surgeon with a difficulty in chewing and swelling in the upper right anterior jaw. The dental surgeon evaluated the case both clinically and radiographically [Table/Fig-3]. The image was then sent to the attending maxillofacial surgeon, who reviewed the case over a smartphone. A treatment plan was developed by surgeon for excisional biopsy of the lesion. Subsequently, a diagnosis of an epulis was obtained.
Epulis is associated in relation to upper lateral incisor and canine tooth

Case 4
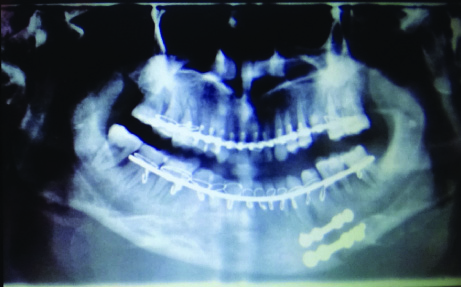
A 37-year-old male patient presented to the emergency room after an assault. After clinical and radiographic evaluations, correct diagnosis of a mandibular fracture done. After patient’s medical fitness patient underwent ORIF (Open Reduction and Internal Fixation) of mandibular body fracture. Postsurgical imaging (OPG) was obtained at the night of surgery and sent to the surgeon for review on his smartphone before morning rounds [Table/Fig-4].
OPG shows the mandibular body fracture reduction and stabilization with two miniplates
Results
Six articles were found with the search terms “Smartphone in Oral and Maxillofacial Surgery” in the online Pubmed database. Five out of six articles met the inclusion criteria for this study. The relevant data was extracted and tabulated [Table/Fig-5]. Conclusions were drawn and discussed based on inclusion criteria of the study.
Literature searched in the PubMed data-base for articles on Smartphones in Oral and Maxillofacial Surgery
| Serial No. | Author (s) | Years | Comments |
|---|
| 1 | Shahid R. Aziz [2] | 2009 | Efficient and effective way for remote specialist consultation. |
| 2 | Jordan M. Kaltman [3] | 2012 | Regardless of time and distance, cost effective service. |
| 3 | Seemann R [4] | 2010 | Teleconsultation and teleteaching become very easy although transmitted video have interruption. |
| 4 | Walker TW [5] | 2011 | Patients did not turn up for follow up |
| 5 | Schulz P [6] | 2013 | Successful implementation of e-learning during the clinical training in dental students. |
Discussion
In 1909, Gugliemo Marconi won the Nobel Prize for Physics for his work on wireless radio communications. Subsequently, the field of telecommunication took great leaps forward, leaving behind antiquated and outmoded forms of communication. Beginning with Marconi’s discovery, telecommunication has been defined as communication over a distance by cable, telegraph, telephone, or wireless broadcasting. The first practical medical use of telecommunication is believed to be in 1955 by Dr. Cecil Wittson who used closed-circuit television and radiotransmitted records for treatment of psychiatric patients [3,7].
Transfer of information from one point to another by means of electronic signals to provide a medical service is known as telemedicine [8]. WHO has described the telemedicine as: Use of information and communication technologies to transfer information the correct diagnosis, treatment, disease and injury prevention, continuing education of health professionals, individuals, or in any case affect the development of community health [9].
Increasingly, the Internet has become a part of our daily lives; the number of internet users in the world is nearly 3,035,749,340 of June 2014. Highest among Asians with 45.7% and least with Oceania and Australians is 0.9%. In India approximately 243,000,000 people use internet [10]. Over time and with development, as information and communication technologies are getting cheaper, telemedicine has steadily expanded the range of applications in the field of medicine and surgery. With the help of internet, rapid transfer of digital documents, images, radiographs, laboratory assays, or accessing desired information of the patients has become cheaper and quicker. Oral and maxillofacial surgeons are taking the advantage of this technology to remotely review both the clinical and radiographic presentation of the maxillofacial patients in preoperative, postoperative, or emergent care [2,11]. Shahid R Aziz introduced the most valuable and proficient method of remote consultation [2]. Jordan M Kaltman also described the technology as a lucrative service, breaking the barriers of time and distance [3].
Smartphones are the latest generation of wireless communication. The smartphone, used in this study, has a touchscreen and a camera of 16 megapixels with flash providing digital-camera quality images. The smartphones display provides a full-colour 1080 × 1920 pixel resolution, providing clear images. In addition, it has a battery capacity of 2500 mAh with internal memory storage of 16GB and a 2GB RAM [12].
Nowadays most of the smartphones have touchscreen interface, Wifi, Bluetooth, NFC and can run 3rd-party apps and are camera phones with super-quick phase detect autofocus facility, optical image stabilizer. In addition, these smartphones now have fourth-generation wireless network technology, with a download speed of 12 Mbits/sec [13]. Various applications can also be found either on commercial or on independent developer Web sites. Key words or titles are entered into search functions to spot the applications of interest. The cost of downloading such applications varies, however, many are free [1]. Various mobile atlas apps like anatomy of head and neck: with CT and MRI images in axial; coronal; and sagittal planes; 12 cranial nerves: origin; course; and their function, dictionary apps like dental dictionary; glossary of dentistry, drug apps like dental Rx; dental STAT; local anaesthesia, imaging apps like dental CT view; iPanoramic, journal apps like dental presss; IJOMS (International Journal of Oral and Maxillofacial Surgery), news apps like dental news; dental tribune, professional forum apps like AAOMS, ACE dental world, surgery apps like AO surgery reference, suturing techniques videos, study apps like NBDE (National Board Dental Examination) Q bank dental board exam, viva learning dental are available [14].
During the differential diagnosis, a common practical problem comes in solving patient’s complaint by dentists or doctors who are not specialists of oral and maxillofacial surgery. The accessibility of high quality consultation is essential; presence of oral and maxillofacial surgeons outside large centres is very limited. Design of the whole project of surgical-prosthetic reconstruction with dental implants, impacted third molar requires expert opinion. It has been renowned by a study that telemedical examination does not vary from clinical examination for the dentists of their specialty [15]. Telemedical consultation has been noted as a success for the evaluation of burn injuries, neurosurgical insult, and digit trauma [16,17].
On the other hand, the demerits of this technology include patient confidentiality and the cost of the device. No clear guidelines for patient confidentiality are available from both the Dental Council and Medical Council of India compared to the other developed countries. Conversely, in the near future clear guidelines will lend a hand in determining patient confidentiality. Cost of smartphones is also declining by the day and in the near future will most likely substitute the conventional phone [18].
Conclusion
Utilization of smartphones in oral and maxillofacial surgery facilitate in differential diagnosis, treatment, follow up, prevention of the disease further and improved the quality with care to the dental and maxillofacial patients regardless of difficulty in accessing the oral and maxillofacial care due to remoteness, inability to travel, or lack of health care facility.