Pulmonary Infection by Blastoschizomyces capitatus in An old Tuberculosis Patient
Sapna Chauhan1, Swati Tiwari2, Paramjit Singh3, Roma Goyal4
1 Assistant Professor, Department of Microbiology, Muzaffarnagar Medical College, Uttar Pradesh, India.
2 Junior Resident 2nd Year, Department of Microbiology, Muzaffarnagar Medical College, Uttar Pradesh, India.
3 Professor and Head of Department, Department of Microbiology, Muzaffarnagar Medical College, Uttar Pradesh, India.
4 Demonstrator, Department of Microbiology, Muzaffarnagar Medical College, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sapna Chauhan, C-46, Faculty Residences, Muzaffarnagar Medical College, Opp. Begrarajpur Industrial Area, Muzaffarnagar, Uttar Pradesh, India.
E-mail: drsapna_chauhan@yahoo.com
Blastoschizomyces capitatus is an arthrospore filamentous fungus. Lung infection by Blastoschizomyces can develop as an opportunistic infection in patients with underlying conditions especially when there is immunosuppression including neutropenia. However, it can occur in non-neutropenic patients with solid organ transplant and patients whose local pulmonary defenses are altered by chronic underlying lung pathology. We report here a case of pulmonary infection by B. capitatus in an old tuberculosis patient.
Fluconazole, Immunocompetence, Sputum
Case Report
A 75-year-old male presented to the Emergency Department of Muzaffarnagar Medical College, Muzaffarnagar, Uttar Pradesh on with fever, breathlessness, epitaxis and malaise. On chest auscultation, bilateral rhonchi and crepitation in intrascapular region were found.
Lab investigations showed Hb 16 gm%, TLC 9900/mm3 with DLC P76L21M02E01B00 and Platelets 2.53lakhs/μl ESR was 35mm in 1st hour FBS=146mg/dl. HIV and HBsAg were both non reactive. Liver and renal function tests were within normal limits. X-ray chest showed patchy consolidation in middle and lower zones. ECG revealed AV block. Sputum sample was send to the Microbiology Department for gram stain, acid fast staining, KOH mount and culture.
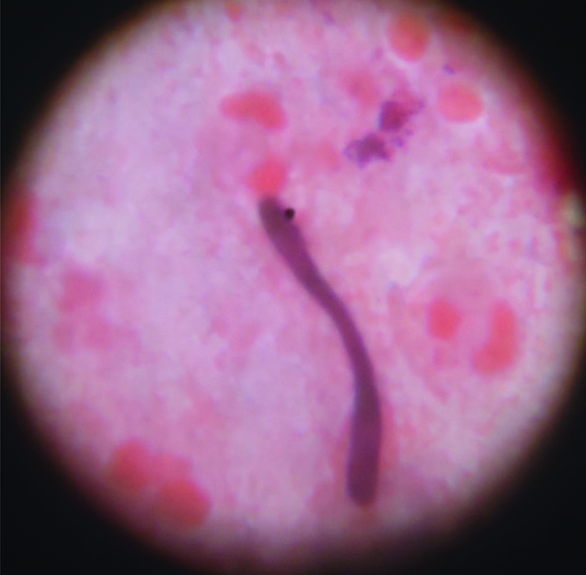
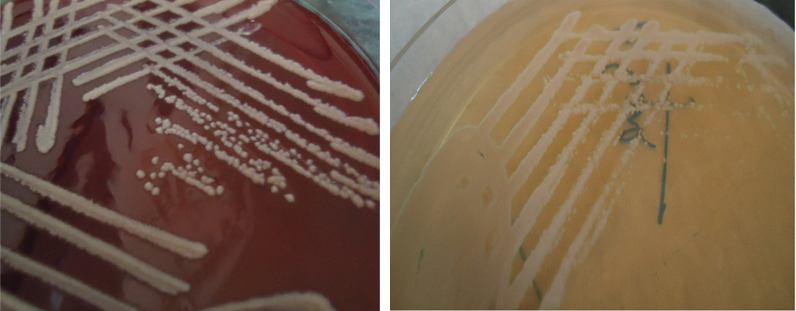
Numerous fungal hyphae with arthrospores were seen on gram staining of the sputum sample [Table/Fig-1]. Direct KOH examination also showed fungal hyphae. No acid fast structures were seen. Culture on blood agar and SDA agar showed pure growth of white to cream colored, yeast like, smooth to wrinkled colonies [Table/Fig-2]. His three repeat samples were examined which also revealed similar findings.
Gram stain of the sputum sample showing fungal hyphae
Blood Agar and Sabouraud’s Dextrose Agar showing cream coloured yeast like colonies of Blastoschizomyces capitatus
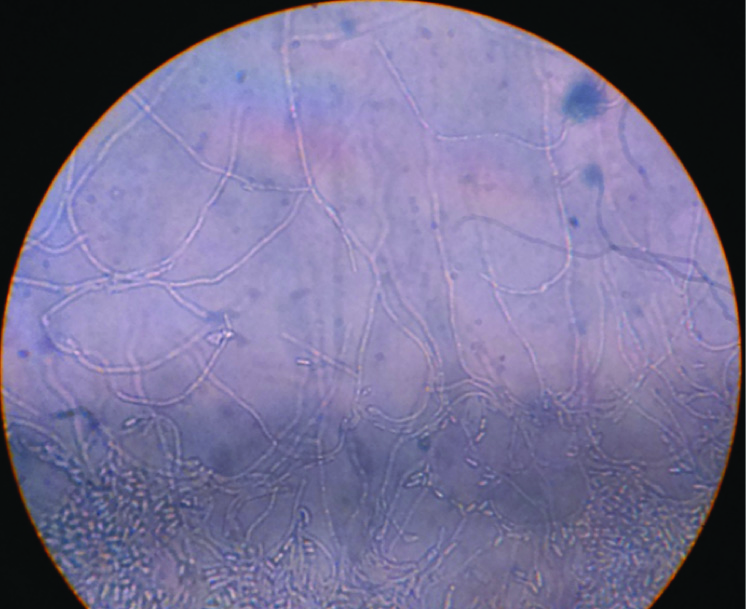
On lactophenol cotton blue preparation and gram staining, true hyphae, pseudohyphae and annelloconidia resembling arthroconidia were seen microscopically [Table/Fig-3]. On further Dalmau plating on Cornmeal Tween 80 agar clusters of annelloconidia at the tips of the annelids were seen [Table/Fig-4]. Further on subculture, growth was obtained at 45°C. The isolated fungus was unable to utilize urea. Glucose and galactose were assimilated. On the basis of direct examination, culture and various biochemical tests, fungus was finally identified as Blastoschizomyces capitatus. A further confirmation of the same was done by the VITEK-2 (bioMèrieux VITEK) system. Antifungal susceptibility was also done by VITEK-2 system, the fungus was found to be sensitive to most antifungal agents.
Lactophenol cotton blue mount showing annelloconidia and pseudohyphae

Dalmau plating on Cornmeal Tween 80 agar showing clusters of annelloconidia
Patient was started on oral fluconazole 150 mg, however, we were not able to follow up the patient as the patient left the hospital against medical advice (LAMA).
Discussion
Invasive fungal infections are increasingly important as causes of morbidity and mortality especially in immunocompromised patients. B. capitatus is an infrequent cause of invasive systemic infection in such patients [1]. Lesions have occurred in the lung, kidney, liver, spleen, brain and other organs; it has also caused endocarditis. The organism is distributed in nature and may be found as normal flora of the skin, respiratory tract and gastrointestinal tract [2]. The organism was previously known with different names as Geotrichium capitatum, Trichosporon capitatum and Saprochaete capitatai [3,4]. Fungus forms yeast like, smooth to wrinkled, white to cream colored colonies on blood agar and Sabouraud agar. On Corn-meal agar, round to oval budding yeast cells with pseudohyphae and many annelloconidia are seen. However, similar picture is also seen with Trichosporon spp. or Candida krusei which may lead to misidentification. Biochemical tests like urease and growth on cycloheximide helps it distinguishing from the above two [5]. Several cases have been reported about Blastoschizomyces infection in immunocompromised patients. Acute leukemias resulting in neutropenia has been the dominant predisposing factor in >90% of patients [6]. Not much data is however available on pulmonary infection by B. capitatus in an immunocompetent individual. Pulmonary mycosis in non-neutropenic patient affects two main populations: the solid organ transplanted patients and patients whose local defences are altered by chronic underlying lung pathology. An internet search revealed only four cases of Pulmonary mycosis [7–9]. It is evident from the studies [Table/Fig-5] that all the patients were elderly but otherwise immunocompetent males except in study by Gill [8] where the patient was a female. All of them were put on azole group of drugs to which they responded very well and recovered. Patient in study by El-Hassani et al., [10] also had tuberculosis as underlying lung pathology just as our study.
Comparative analysis of various studies on Pulmonary mycosis
| Author | Year | Age & Sex of patients | Treatment offered | Treatment outcome |
|---|
| Wills TS et al., [7] | 2004 | 40-year-Male | Oral Fluconazole + Inj. Amphotericin B | Recovered completely |
| Gill P and Gill J [8] | 2011 | 70-year-Female | Oral Fluconazole | Recovered completely |
| Dhevahi E et al., [9] | 2014 | 52-year-male68-year-male | Oral ItraconazoleOral Itraconazole | Recovered completely |
| Our study | 2015 | 75-year-Male | Oral Fluconazole | Recovered completely |
Conclusion
Infections due to less pathogenic and non-pathogenic fungi are on a rise. B. capitatus is an infrequent cause of invasive systemic infection in immunocompromised hosts. However it can cause pulmonary infection in patients without immunosuppression but with underlying lung pathology. Hence, the use of definitive diagnostic procedures and the rational application of antifungals can only curb the situation.
[1]. Girmenia C, Pagano L, Marino B, D’Antonio D, Fanci R, Spechia G, Invasive infections caused by Trichosporon species and Geotrichium capitatum in patients with haematological malignancies: a retrospective multicenter study from Italy and review of the literatureJ Clin Microbiol 2005 43:1818-28. [Google Scholar]
[2]. Naficy AB, Murray HW, Isolated meningitis caused by Blastoschizomyces capitatusJ infect Dis 1990 161:1041-42. [Google Scholar]
[3]. De Hoog GS, Smith MT, Ribosomal gene phylogeny and species delimination in Geotrichium and its telemorphsStudies in Mycology 2004 50:489-515. [Google Scholar]
[4]. Salkin I, Gorden M, Samsonoff W, Reider C, Blastoscizomyces capitatus, a new combinationMycotaxon 1985 22:375-80. [Google Scholar]
[5]. Larone DH, Medically important fungiA guide to identification (2nd ed) 1993 Washington DCAmerican Society for Microbiology:25 [Google Scholar]
[6]. Birrenbach T, Bertschy S, Aebersold F, Mueller NJ, Achermann Y, Muehlethaler K, Emergence of Blastoschizomyces capitatus Yeast Infections, Central EuropeEmerg Infect Dis 2012 18:98-101. [Google Scholar]
[7]. Wills TS, Degryse A, Lavina J, Sinnott JT, Blastoschizomyces capitatus pneumonia in an immunocompetent maleJ of Southern Medical Association 2004 97(7):702-04. [Google Scholar]
[8]. Gill P, Gill J, Blastoschizomyces capitatus pneumonia in an immunocompetent FemaleIndian J Tuberc 2011 58:88-89. [Google Scholar]
[9]. Dhevahi E, Sumathi S, Shree B, Sambantham S, Blastoschizomyces capitatus: An rare opportunistic infection alerts the clinical correlation from a tertiary care hospital at ChennaiIOSR Journal of Dental and Medical Sciences 2014 13(6):59-62. [Google Scholar]
[10]. El-Hassani I, Deham H, Touaoussa A, Er-Rami M, Pulmonary infection by Geotrichum capitatum about a case and review of the literatureJ Mycol Med 2014 24(4):341-44. [Google Scholar]