Fracture of a structurally compromised tooth is commonly seen in individuals, who fail to undergo restoration of the same with a core and crown. Restoration with a core provides adequate resistance form for the tooth structure. Functionally a core should withstand all occlusal loads applied and distribute equally to the remaining portion of the tooth. Property of the core material to withstand the masticatory forces and resistance to dislodgement plays an important role in success of the restoration. Failure of the core material can result in crown failure.
Core materials used in dentistry include amalgam, resin composites, titanium reinforced resin composite, lanthanide reinforced composite, glass–ionomer and heat pressed ceramic and cast-gold [1]. Resin composite continues to be one of the most used core restoration materials in dentistry. Resin composites offer various advantages including high strength, fluoride release, ease of manipulation and also enhance the ability to reproduce the shade and translucency of natural teeth. However, the dentin may suffer from micro leakage and the ability of composites to absorb moisture makes their dimensional stability unsatisfactory [2,3]. The developments in reinforced glass-ionomer cements have created new choices in the selection of materials. The use of glass-ionomer as core materials has some characteristics including a weak bond to enamel and dentin, fluoride release and a low coefficient of thermal expansion. The disadvantages of glass-ionomer as core materials include their lack of compressive and tensile strength and their brittle characteristics [4].
Fracture resistance has been established as an appropriate method of investigating tooth strength and also to compare the strength of different core buildup materials. Fatigue test is one of the trustworthy investigations to evaluate core material as they simulate the clinical situation by imitating the physiological cyclic loading.
Various studies have been done to evaluate the fracture resistance of core materials like composite resin, lanthanide reinforced flowable resin composite, Ti reinforced composite, silver reinforced glass ionomer, amalgam and ceramic inlay with tooth preparation [5–7]. Those studies have been conducted to assess the strength of the core materials directly rather, after restoration with a crown [5].
Therefore the clinician is often puzzled with the variety of materials and decision making is often difficult to render the best possible treatment. In reality the core materials which restore the broken tooth structure are covered by a full crown restoration. If there is no significant difference in the fracture of the various core materials, the clinician could choose a core material based on other properties like ease of manipulation and adhesion to tooth structure. Thus the purpose of the study is to compare the strength of different core materials on a compromised tooth structure under metallic artificial crown. The working hypothesis was that there may not be significant differences in the fracture resistance of the various core materials chosen for the study when they are restored with a crown under simulated load conditions.
Materials and Methods
This study was conducted in the Department of Prosthodontics and Implantology, Rajah Muthaiah Dental College and Hospital in collaboration with the Department of Instrumental Engineering, Annamalai University, Chidambaram, India.
Seventy extracted, human maxillary premolars of average size and morphology, without caries, abrasion, fillings, injury from forceps or fractures were collected. The teeth were cleaned with ultrasonic scalers and stored in distilled water at room temperature. The teeth were embedded in autopolymerising resin (D.P.I -cold cure, Dental Product of India, Mumbai, India) at a position 2mm below the cemento-enamel junction [Table/Fig-1]. The teeth were randomly divided in-to four groups, designated as A, B, C and D. Each group contained 20 teeth, except Group A which contained 10 teeth. All the teeth were subjected to free hand preparation by a single operator with 1mm chamfer.
Teeth mounted in acrylic resin blocks

Extensive class-I cavities (approximately 2mm of tooth structure remaining in the periphery) were prepared, to simulate extensive tooth loss in all the teeth belonging to groups B, C, and D. Group A served as control group. Class I cavity was prepared using diamond burs in a contra-angle high speed airotor handpiece with water coolant such that the height of the remaining buccal wall was 4mm and the lingual wall was 3mm. Depth of the cavity was measured with a periodontal probe. The prepared teeth were then restored according to the manufacturer’s instructions, with the three core build up materials as follows:
Group B – Cavities were treated with dentine conditioner (D- Tech, Pune, India) for 20 sec, rinsed, dried gently and restored with Silver reinforced glass ionomer (SHOFU Hi Dense XP, Kyoto, Japan). Excess material was removed and restoration contoured.
Group C – Cavities were treated with ecthant for 15 sec, rinsed and dried gently. A layer of light cure bonding agent (sci pharma) was applied and cured for 30 sec, following which packable composite resin (3M EPSE Filtek P60, St. Paul, Minnesota, USA), was incrementally added and light cured.
Group D – The dentine was conditioned, rinsed and dried as above. Then the cavity was restored with Resin reinforced glass ionomer (GC Gold Label light cure GIC, GC coporation Tokyo, Japan). After removal of the excess, the material was light cured.
Wax patterns of 0.75mm thickness were made for 10 teeth in each group and cast in a base metal alloy (Nickel Chromium- Dura alloy, Scottdale, Pennsylvania, USA) using conventional casting technique [8]. All the Crowns were cemented to the teeth with type I glass ionomer cement (Fuji Plus, GC corporation, Leuven, Belgium, Europe). Cement was applied on the internal surface of the crowns with the help of spatula and was placed in position with a firm finger pressure [9]. The randomly selected remaining ten teeth in group B, C, D did not receive the crowns and served as subgroups B1, C1, D1. All the specimens were stored in distilled water at room temperature until (approximately 3 weeks) subjected to testing.
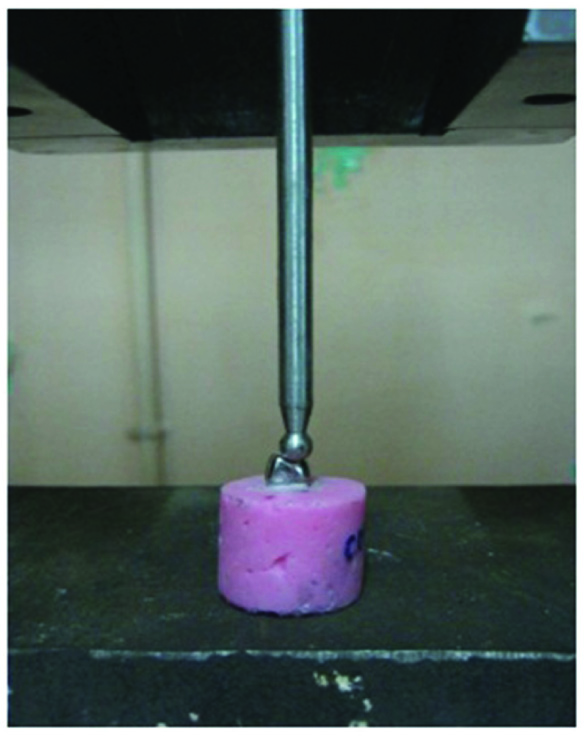
All the specimens in each group were exposed to 1.2 million cycles of fatigue loading in computer controlled chewing simulator [Table/Fig-2]. This protocol simulated 5 years of clinical service [5,6]. A cyclic static load of 500N was applied at the occlusal surface of the restoration by means of a steel ball with 6mm diameter placed mesially making contact with the cuspal inclines and perpendicular to the long axis of the tooth [7]. The number of specimens still intact after the fatigue loading was recorded and considered as survival in present.
Cyclic loading in artificial chewing simulator
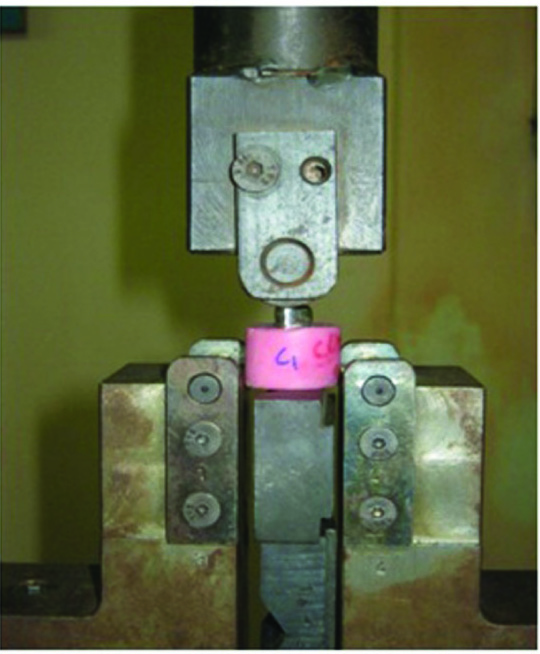
All the specimen that did not fracture during cyclic loading was loaded until fracture in a universal testing machine with a cross speed of 5mm/min [Table/Fig-3]. The force at which the fracture occurred was recorded in the computer software. Mode of failure was recorded.
Static loading in universal testing machine
The means and standard deviations of fracture strength value of all groups were used for statistical analysis. Statistical inferences among the groups were made using one-way ANOVA and multiple pair wise comparisons between the groups, subgroups and within them were done using Duncan Multiple Range and Student-t Test (p-value of <0.05 was considered as significant).
Results
All the samples survived 1.2 million cycles of static loading in the chewing simulator. The mean failure load of the specimens in group A, B, C, D with artificial crown were 2160 N, 1996 N,1931 N, 1886 N respectively and the mean failure load of the specimens in group B1, C1, D1 without artificial crowns were 1864 N, 1031 N, 896 N respectively [Table/Fig-4].
Descriptive statistical table for fracture strength of different core materials
| Group | n | Mean ± SD |
|---|
| A | 10 | 2160 ± 54.36 |
| B | 10 | 1996 ± 10.75 |
| B1 | 10 | 1864 ± 44.91 |
| C | 10 | 1931 ± 28.09 |
| C1 | 10 | 1031 ± 21.33 |
| D | 10 | 1886 ± 33.4 |
| D1 | 10 | 896 ± 18.16 |
All the specimens in group A, B, C, D demonstrated one mode of failure, with a fracture at the junction of crown margin and tooth, while the specimens in group B1, C1, D1, had fracture of both the core and the tooth.
Since the one-way ANOVA analysis of the fracture was significant (p =<0.001), the core materials were ranked with the Duncan multiple range test [Table/Fig-5]. According to Duncan’s test results for specimens in Group A, B, C, D; Control group was superior to group containing core materials. Among core materials Miracle mix was significantly superior followed by Composite and Reinforced Light Cure Glass Ionomer. However, the Duncan’s test results for specimens in Group B1, C1, D1; demonstrated that Miracle Mix was significantly superior followed by Composite and Reinforced Light Cure Glass Ionomer.
Group Comparison of fracture strength using One-Way ANOVA
| Group | N | Mean | SD | F- Value | p-value* |
|---|
| A | 10 | 2160 | 54.36 | | < 0.001 |
| B | 10 | 1996 | 10.75 | |
| C | 10 | 1931 | 28.09 | 115.56 |
| D | 10 | 1886 | 33.4 | |
| Total | 40 | | | |
* = p<0.001=SS= statistically significant
Statistical analysis using Student’s independent t-test was done to find significant difference between the Groups B, C, D and B1, C1, D1 [Table/Fig-6]. The t-test results showed there was significant difference of fracture load between the Group B and B1/ C and C1 / D and D1 (i.e. samples with artificial crown had more fracture strength than samples without crown).
Student’s independent t-Test
| Group | n | Mean ± SD (N) | p-value ¶ |
|---|
| B | 10 | 1996 ± 10.74 | < 0.001 |
| B1 | 10 | 1904 ± 44.91 |
| C | 10 | 1931 ± 28.09 | < 0.001 |
| C1 | 10 | 1031 ± 21.33 |
| D | 10 | 1886 ± 33.39 | < 0.001 |
| D1 | 10 | 896 ± 18.16 |
¶= p<0.001=VHS= very highly significant
Discussion
A variety of core materials are available to the dental practitioner to rebuild the structurally compromised tooth. In previous studies the choice of core materials have been tested using restored endodontically treated teeth without crowns [2,10,11]. Limited studies were observed to test the behaviour of such teeth when restored with a crown and subjected to mechanical stresses Therefore in this study, a scenario was selected which simulates the clinical experience. This study assessed the fracture strength of three core materials (miracle mix, composite resin and reinforced glass ionomer) with and without artificial crowns.
In the present study, extracted human maxillary premolars were used as abutments [1,3,12]. The advantage is that natural teeth possess a similar modulus of elasticity, hardness and strength as teeth in the oral environment. Yet a drawback of great variation in age, size, shape and quality, have made it difficult to standardize the samples. To overcome these problems abutments with comparable sizes were selected. Teeth which were too small or too big, as well as teeth with caries and other morphological variations were excluded.
The teeth were rooted in resin without simulated periodontal ligaments. Tooth mobility in the sockets in the presence of periodontal ligament may not affect the study result as the magnitude of load applied for the test load is quite high [1,2,10,13]. Teeth were set perpendicular in the artificial chewing simulator in order to simulate the occlusal force [14]. A force of 500N was applied during the dynamic loading. This simulates mean values of chewing forces in the premolars [7].
Cohen et al., reported that the glass ionomer demonstrated a lower fatigue resistance than composite and silver amalgam which is similar to the results of our study [15]. Bonilla et al., compared five core materials and concluded that titanium-reinforced composite resin, had greater resistance followed by amalgam and gic but according to our study the Miracle Mix had more resistance followed by Composite and reinforced GIC [16]. Coltak et al., determined the fracture resistance of three core materials supported by post and reported that composite resin supported by post had greater resistance followed by amalgam and GIC which is slightly different from our study were miracle mix had more resistance followed by composite and reinforced GIC [17]. Preetam Shah et al., evaluated the fracture resistance of endodontically treated teeth reinforced with different core materials and reported that GIC had the highest fracture resistance followed by Silver Amalagam and IRM [18]. Steven et al., reported that the fracture strength of resin composite core was significantly higher than metal reinforced glass ionomer core material [12].
Compressive strength is a vital predictor for success of the restoration, as its high value endures occlusal and parafunctional forces. Therefore our study considered both cyclic and static compressive load to evaluate the fracture strength of the core materials. The result of our study addressed that none of the restored teeth with or without artificial crown fractured during exposure in the artificial chewing simulator. Differences were noted between test specimens when subjected to static load (p < 0.001). Shofu Hi Dense XP had a higher fracture toughness (B 1996 N, B1 1864 N) when compared to Filtek P60 composite (C 1931 N, C11031 N) and GC light cure GIC (D 1886 N, D1 896 N), when the teeth were subjected to load with and without crown. Fracture strength of Filtek P60 composite (C 1931 N, C11031 N) was greater than GC light cure GIC (D 1886 N, D1 896 N).
On the basis of strength alone Composite resin and resin modified GIC are used as core material as an alternative to miracle mix cement. However, the light-cured materials have some disadvantages like incomplete curing due to insufficient light intensity or curing time is used or too great a thickness is applied. Although excellent adhesion to tooth structure can be achieved with dentinal bonding agents, the long-term stability of such bonds is unknown [19].
Strength is the principle factor for selecting a core material, because this property improves the clinical success rate of the core material by resisting deformation and offering even stress distribution. Although the perfect core material does not yet exist, the results of our study and other prior studies indicate that both miracle mix and resin composites may be indicated for use as core materials in specific clinical situations.
The findings in this study do suggest that all the specimens survived the cyclic fatigue loading of 1.2 million cycles which is convincing with the clinical survival rate. This may indicate the significance of the crown component in determining the strength by stabilizing the restoration in a clinical situation.
Despite, the samples were subjected to static load to determine the ultimate strength of each core material. Though the results obtained from the static load elicits significant difference between the core materials, usage of these values for selecting the core material for a clinical situation requires further longitudinal clinical investigation. Such results would help the clinician to select the core material based on the other properties like ease of manipulation and adhesion to tooth structure.
Limitation of This Study
This was confined only to the premolars of both arches and should be elaborated for different tooth.
This study may not accurately reflect the situation invivo as the fracture resistance was determined by applying heavy load to a single point.
Thermocyclicing was not performed for cyclic loading which would have simulated the natural phenomena.
Gum resin to simulate the cushioning effect of periodontal fibers was not included in this study.
Conclusion
It was concluded that the survival rate between the different core materials are the same with or without crown. The choice of core materials definitely influences the overall strength of the restoration with or without crowns in this in vitro study. Miracle mix had a greater fracture resistance than other core materials viz: composite resin, resin modified Glass Ionomer Cement.
* = p<0.001=SS= statistically significant
¶= p<0.001=VHS= very highly significant