An Unusual Transorbital Penetrating Injury by House-key (lock): A Case Report with a Small Review of Literature
Santanu Sarkar1, Sandeep Modi2, Arup Kumar Seth3, Soumyajyoti Panja4
1 Clinical Tutor, Department of General Surgery, Burdwan Medical College & Hospital, West Bengal, India.
2 PG Resident, Department of General Surgery, Burdwan Medical College & Hospital, West Bengal, India.
3 PG Resident, Department of General Surgery, Burdwan Medical College & Hospital, West Bengal, India.
4 PG Resident, Department of General Surgery, Burdwan Medical College & Hospital, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Santanu Sarkar, 1/3/1 C Ramlal agarwala Lane; Sinthee; Kolkata- 700050, India. E-mail : drsantanu.surg@gmail.com
Penetrating injuries of the brain are quite uncommon, comprising approximately 0.4% of all head injuries. In our case, a four-year-old boy who fell forward on a house-key (lock) accidentally while playing with some other children sustained a left sided penetrating transorbital brain injury. After hospital admission, the patient had a Glasgow Coma Scale (GCS) score of 15/15, no visual loss but restriction of upward gaze (left eye) and profuse bleeding from the wound site. Firstly, the metallic key was removed in emergency operation theatre and haemostasis secured. Next day we did a combined surgical approach with neurosurgeons, Eye-surgeons and general surgeons after having CT scan report. We report this case because penetrating head injury is rare and transorbital penetrating head injury is even rarer and a predicament in emergency surgical practice with controversial management.
Cranio-cerebral injury, CT scan, GCS score, Orbital roof fracture
Case Report
A four-year-old boy fell from the bed on his face while playing in home resulting in a penetrating transorbital injury by house key which was kept on the floor inadvertently. While taking admission in casualty ward at midnight, the patient was conscious and completely responsive with GCS score of 15 points. Physical examination revealed a left supraorbital (superolateral aspect) wound [Table/Fig-1a]; but no bony defects were palpated over the superior orbital rim. The eyeball was intact with normal visual acuity but restriction of movement of his left eye was noticed especially in upward gaze. There was no history of vomiting or loss of consciousness.
(a) House-key impacted into the superolateral aspect of left orbit (b) Antero-posterior x-ray of face and cranium showing metallic key in left orbit
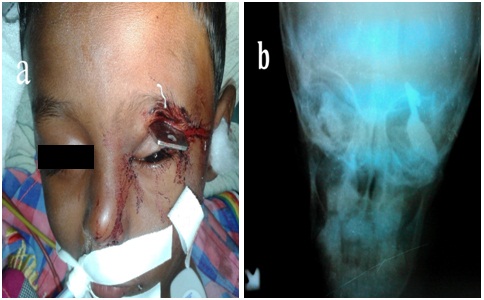
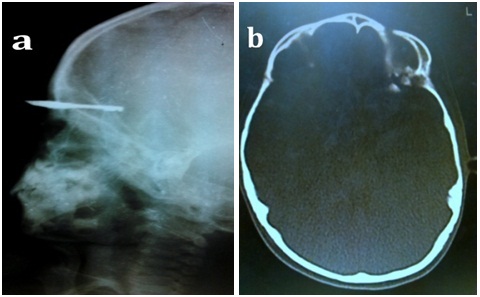
X-ray of skull was done immediately (both antero-posterior and lateral view), which revealed a metallic house key impacted into the left orbit [Table/Fig-1b,2a]. The child was immediately shifted into the operation theatre as there was profuse bleeding from wound site. Wound site was explored to remove the key under general anaesthesia. Next day morning CT scan of brain and orbit was done which revealed a fracture of the supero-lateral orbital roof (left) with displacement of the fracture fragments into the anterior cranial fossa [Table/Fig-2b] but surprisingly there was no further clinical deterioration. Considering the consequences of impacted foreign bodies in brain, the patient was shifted to nearest neurosurgical centre where with the help of multidisciplinary team approach including general surgeons, neurosurgeons and eye surgeons an extradural frontal craniotomy was done to explore the bony defect of left orbital roof and to remove bone fragments. Pericranium was then placed over the bony defect for stabilization of the orbital roof and the tear of the left superior rectus muscle was repaired by ophthalmologist. There was a small dural tear which was also repaired. Postoperative period was uneventful where the patient was treated with intravenous 3rd generation cephalosporin, dexamethasone and regular dressing. The patient was discharged home on 10th Postoperative day on prophylaxis for seizure for one month and tapering dose of oral steroids. He is under follow-up for last two months without any neurological or ocular complications.
(a) lateral x-ray of face and skull showing intracranial extension of foreign body; (b) Axial CT scan brain showing left orbital roof fracture fragments
Discussion
Penetrating brain injuries (PBI) are usually caused by relatively high-velocity metal objects i.e. missile, stab knife etc. and also can occur in explosions (splinters), motor vehicle collisions (metallic rod), occupational (screw drivers, nails, pins etc) or household accidents by scissors, glass, sharp-nails etc. Although less prevalent, PBI carries a worse prognosis than closed head trauma [1]. There are different routes for penetrating intracranial injury through the orbit among which the commonest route of entry is through superior orbital roof. The orbital roof is made up of the orbital plate of the frontal bone and the lesser wing of the sphenoid bone. It is very thin than other parts of the cranium and is therefore at particular risk of injury specially in children, because of the lack of a pneumatized frontal sinus [2]. There are certain other areas within the orbit that may provide direct access to the cranial cavity, such as the superior orbital fissure, inferior orbital fissure and the optic canal. Turbin et al., reported the pattern of transorbital intracranial injury and divided the orbital surface into four different zones [3]. The complications of transorbital penetrating cranio-cerebral injury include consequences of extra-ocular muscle injury, Intra-parenchymal brain lesions like cerebral oedema, cerebral contusions, intra-cerebral haematoma, subdural and epidural haematoma, subarachnoid haemorrhage, pneumocephalus, cerebrospinal (CSF) fluid fistulas, etc. Infective complications including brain abscess, encephalitis, meningitis, osteomyelitis and scalp wound sepsis & vascular complications like pseudo-aneurysm, post-traumatic carotico-cavernous fistula rarely also can occur [4]. The risk of postoperative seizure is as high as 30 to 50%, of which 10% appear within first week of trauma [5]. Initially there may be no apparent neurological deficit on examination and therefore a lack of neurological signs does not exclude an associated brain injury [6]. Chibbaro et al., reported 18 cases of orbito-cranial injuries caused by penetrating non-missile foreign bodies where GCS of 14-15 was noticed in 50% of subjects without obvious evidence of intracranial injury [7]. Therefore, even in the presence of a trivial orbital wound, a thorough ophthalmological examination and neurological evaluation is recommended supplemented by imaging studies (CT Scan) whenever necessary. Non-displaced or minimally displaced orbital roof fractures are usually managed by observation [8]. Early surgical exploration is recommended to reduce the morbidity in cases of retained foreign body and displaced fracture. A search of English medical databases, using key words transorbital penetrating injury and brain injury, revealed some interesting case reports, which were compiled in [Table/Fig-3] [9–17].
Published case reports of unusual transorbital penetrating brain injury
| Author | Journal | Year ofPublication | ±Age & Sex | Penetrating objects | Outcome |
|---|
| O’Neill OR et al., [9] | Surg Neurol | 1994 | — | Hunting arrow | Uneventful recovery |
| Paucic-Kirincic E et al., [10] | Pediatr Rehabil | 1997 | 9(M) | Toy-arrow | Enucleation of lt. eye ball, Latent rt. Sided haemiparesis & Cognitive disturbances |
| Cackett P et al., [11] | Emerg Med J | 2005 | 20(M) | Short bladed knife | Uneventful recovery |
| Lin HL et al., [12] | J Chin Med Assoc | 2007 | 83(F) | Iron bar | Blindness in the rt.eye; lt. haemiparesis |
| Satyarthee GD et al., [13] | Neurol India | 2009 | 28(M) | Ceramic stone | Enucleation of the eyeball |
| Paiva et al., [14] | International Journal of Emergency Medicine | 2010 | 10(M) | Bamboo stick | Uneventful recovery |
| Huiszoon et al., [15] | Case Reports in Ophthalmological Medicine (Hindawi) | 2012 | 45(F) | Bicycle hand brake | Death |
| Abdulbaki A et al., [16] | The Indian Journal of Neurotrauma | 2012 | 5(F) | Pen | Brain abscess |
| Ramdurg SRet al., [1] | The Indian Journal of Neurotrauma | 2014 | 20(M) | Branch of a tree | Seizure |
| Gupta OP et al., [17] | The Indian Journal of Neurotrauma | 2014 | 47(F) | Valve of pressure cooker | Uneventful recovery |
| Present case | J clin & diag research (jcdr) | 2015 | 4(M) | House-key | Uneventful recovery |
±Age in years; Sex: M=male, F= female; rt=right, lt=left
The principles of treatment for transorbital penetrating injury are removal of bone fragments and foreign body, control of persistent bleeding and intracranial hypertension, prevention of infection through debridement of all contaminated and necrotic tissues and at the same time preservation of as much nervous tissue as possible, and restoration of anatomic structures through accurate closure of the dura and lastly reconstruction of orbital roof. Jin Woo Kim et al., reported successful use of titanium micromesh and micro-screw system for large displaced fracture. These meshes do not interfere with postoperative imaging [18].
Conclusion
In a case of transorbital penetrating injury, high index of suspension for underlying brain injury even in absence of any neurological symptoms is mandatory and appropriate radiological imaging should be considered. Outcome depends upon the type of object, site of entry into the eye globe, its trajectory, involvement of paranasal sinuses, extent of brain parenchymal injury and the septic complications. Furthermore, we also emphasize the importance of a combined team approach involving general surgeons, neurosurgeons and ophthalmologists for surgical intervention in such cases.
±Age in years; Sex: M=male, F= female; rt=right, lt=left
[1]. Ramdurg SR, An Unusual Case of Trans-orbital Penetrating Brain Injury due to Fall on Branch of a TreeThe Indian Journal of Neurotrauma 2014 http://dx.doi.org/10.1016/j.ijnt.2014.12.007 [Google Scholar]
[2]. Fulcher TP, Sullivan TJ, Orbital roof fractures: management of ophthalmic complicationsOphthal Plast Reconstr Surg 2003 19:359-63. [Google Scholar]
[3]. Turbin RE, Maxwell DN, Langer PD, Patterns of transorbital intracranial injury: a review and comparison of occult and non-occult casesSurvey of Ophthalmology 2006 51(5):449-60. [Google Scholar]
[4]. Bard LA, Jarrett WH, Intracranial complications of penetrating orbital injuriesArchives of Ophthalmology 1964 71:332-43. [Google Scholar]
[5]. Salazar AM, Jabbari B, Vance SC, Grafman J, Amin D, Dillon JD, Epilepsy after penetrating head injury, I. Clinical correlates: a report of the Vietnam Head Injury StudyNeurology 1985 35:1406-14. [Google Scholar]
[6]. Solomon KD, Pearson PA, Tetz MR, Cranial injury from unsuspected penetrating orbital trauma: a review of five casesJ Trauma 1993 34:285-89. [Google Scholar]
[7]. Chibbaro S, Tacconi L, Orbito-cranial injuries caused by penetrating non-missile foreign bodies. Experience with eighteen patientsActa Neurochir(Wien) 2006 148:937-42. [Google Scholar]
[8]. Bolling J.P, Wesley R.E, Conservative treatment of orbital roof blow-in fractureAnn Ophthalmol 1987 19:75-76. [Google Scholar]
[9]. O’Neill OR, Gilliland G, Delashaw JB, Purtzer TJ, Transorbital penetrating head injury with a hunting arrow: case reportSurg Neurol 1994 42:494-97. [Google Scholar]
[10]. Paucic-Kirincic E, Prpic I, Gazdik M, Kriz M, Vojnikovic B, Golubovic V, Transorbital penetrating brain injury caused by a toy arrow: a case reportPediatr Rehabil 1997 1(3):191-93. [Google Scholar]
[11]. Cackett P, Stebbing J, Transorbital brain injuriesEmerg Med J 2005 22:299doi: 10.1136/emj.2003.007427 [Google Scholar]
[12]. Lin HL, Lee HC, Cho DY, Management of transorbital brain injuryJ Chin Med Assoc 2007 70(1):36-38. [Google Scholar]
[13]. Satyarthee GD, Borkar S, Tripathi A, Sharma BS, Transorbital penetrating cerebral injury with a ceramic stone: report of an interesting caseNeurol India 2009 57:331 [Google Scholar]
[14]. Paiva WS, Monaco B, Prudente M, Soares MS, De Amorim RLO, De Andrade AF, Teixeira MJ, Surgical treatment of a transorbital penetrating brain injuryClinical Ophthalmology 2010 4:1103-05. [Google Scholar]
[15]. Huiszoon WB, Noe PN, Manten A, Fatal transorbital penetrating intracranial injury caused by a bicycle hand brakeInternational Journal of Emergency Medicine 2012 5:34 [Google Scholar]
[16]. Abdulbaki A, Otaibi FA, Almalki A, Alohaly N, Baeesa S, Transorbital Craniocerebral Occult Penetrating Injury with Cerebral Abscess ComplicationCase Reports in Ophthalmological Medicine 2012 2012:742186:6pages, 2012. doi:10.1155/2012/742186 [Google Scholar]
[17]. Gupta OP, Roy K, Ghosh S, Tripathy P, An unusual penetrating transorbital craniocerebral InjuryThe Indian journal of neurotrauma 2014 11:53-56. [Google Scholar]
[18]. Kim JW, Bae TH, Kim WS, Kim HK, Early Reconstruction of Orbital Roof Fractures: Clinical Features and Treatment OutcomesArchives of Plastic Surgery 2012 39(1):31-35. [Google Scholar]