Comparative Evaluation of Bolus Administration of Dexmedetomidine and Fentanyl for Stress Attenuation During Laryngoscopy and Endotracheal Intubation
Sellamuthu Gunalan1, Rajagopalan Venkatraman2, Govindarajan Sivarajan3, Paneerselvam Sunder4
1 Postgraduate Student, Department of Anaesthesiology, SRM Medical College Hospital and Research Centre, Potheri, India.
2 Associate Professor, Department of Anaesthesiology, SRM Medical College Hospital and Research Centre, Potheri, India.
3 Professor and Head of the Department, Department of Anaesthesiology, SRM Medical College Hospital and Research Centre, Potheri, India.
4 Assistant Professor, Department of Anaesthesiology, SRM Medical College Hospital and Research Centre, Potheri, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajagopalan Venkatraman, B3, 3rd Block, Jains Ashraya Phase 3, 199, Arcot Road, Virugambakkam, Chennai – 600092, India. E-mail : drvenkat94@gmail.com
Background
Laryngoscopy and endotracheal intubation can cause hypertension and tachycardia which can result in myocardial ischemia or stroke in vulnerable people. The objective of our study was to compare the efficacy of bolus dose of dexmedetomidine and fentanyl in attenuating haemodynamic stress responses following laryngoscopy and intubation.
Materials and Methods
Sixty patients who were fixed to undergo elective surgeries under general anaesthesia were randomly divided into 2 groups. Group 1 received 1 mcg/kg of dexmedetomidine over 10 minutes and group 2 received fentanyl 2mcg/kg before induction. Anaesthesia was standardized in both the groups and vital parameters were recorded for up to 10 minutes after intubation.
Results
Dexmedetomidine in a dose of 1mcg/kg prevented an increase in heart rate following laryngoscopy when compared to fentanyl group. This effect lasted for 10 minutes after intubation is performed. Though dexmedetomidine prevented an increase in blood pressure, this effect was statistically significant only for 2 minutes after intubation when compared to fentanyl group.
Conclusion
Attenuation of rise in heart rate and blood pressure following laryngoscopy and endotracheal intubation was better with 1mcg/kg of dexmedetomidine when compared to fentanyl.
Dexmedetomidine, Intubation reflexes, Opioids, Stress response
Introduction
Laryngoscopy and endotracheal intubation increase the plasma concentration of catecholamines due to sympathetic stimulation which can result in tachycardia and hypertension in most of the individuals [1,2]. The longer the duration and greater the force of laryngoscopy, severe is going to be the haemodynamic stress response. The elevation in arterial pressure generally starts before five seconds of laryngoscopy, peaks in 1–2 min and returns to normal levels inside 5 min [3]. This may not bring on any unfriendly consequences for normal people but rather could be dangerous in patients with cerebrovascular diseases, hypertension or myocardial insufficiency [4]. The laryngoscopic response in these patients can increase myocardial oxygen demand and may lead to complications in susceptible individuals [5,6]. In spite of the availability of numerous drugs to blunt the haemodynamic response, the search for an ideal drug with minimal adverse effect continues.
Several strategies have been tried to obtund stress response following laryngoscopy and endotracheal Intubation like local anaesthetics, intravenous opioids, β blockers, α2 adrenergic agonists, vasodilators, magnesium or by increasing volatile anaesthetic concentrations [7]. No single agent has been established as the most appropriate for this purpose. The disadvantages of these drugs vary from inadequate control of haemodynamics to various adverse effects like severe hypotension, bradycardia, arrhythmias, chest wall rigidity and delayed recovery. Alpha 2 (α2) adrenergic agonists like clonidine decrease sympathetic tone and has been demonstrated to reduce the stress responses to laryngoscopy [8,9]. Dexmedetomidine is an extremely selective α2 receptor agonist having eight times higher affinity and α2 selectivity contrasted with clonidine. The different benefits of dexmedetomidine are anxiolytic, sedation, analgesia and better haemodynamic control without any respiratory depression [10]. Because of its shorter duration of action, it does not interfere much with recovery from anaesthesia. It also decreases intraoperative opioid and volatile anaesthetic requirements for maintenance of anaesthesia as it decreases minimum alveolar concentration (MAC) of volatile anaesthetics by up to 90% [11–13].
Fentanyl is a potent narcotic with rapid onset and short duration of action and is routinely used in the context of balanced anaesthesia. Fentanyl given in a dose of 2 mcg/kg 5 minutes before laryngoscopy attenuates the haemodynamic stress response following laryngoscopy and endotracheal intubation. Fentanyl is a synthetic opioid attenuating the cardiovascular response by its action on opioid receptors and also by decreasing sympathetic outflow [14].
A search through PubMed and Scopus indexed journals did not reveal any study comparing these two ideal agents for stress attenuation, dexmedetomidine and fentanyl and only very few studies are available in other non-indexed journals [15–18]. The objective of this study was to compare the efficacy of bolus administration of IV dexmedetomidine 1mcg/kg with IV fentanyl 2mcg/kg in attenuating the cardiovascular stress response accompanying laryngoscopy and endotracheal intubation and to look for any adverse effects of these drugs.
Materials and Methods
This prospective randomized, double blinded control study was done in a tertiary medical college hospital from August 2012 to August 2013 after getting institutional ethical committee approval. The patients were kept informed of the study and consent was obtained. Sixty patients undergoing elective surgical procedures under general anaesthesia with endotracheal intubation were selected for the study.
Inclusion Criteria: ASA Physical status I and II patients in the age group of 18 to 60, weighing between 50 to 100 kg and with airway of Modified Mallampati Grade I and II were included in the study.
Exclusion Criteria: The patients with hypertension, ischemic heart disease, pregnancy, full stomach and emergency surgery were excluded from the study. Patients with ASA Physical status III and above, suspected difficult airway and modified Mallampatti Grade III and IV were also excluded from the study. Patients who had Cormack Lahane score III and above and also those in which duration of laryngoscopy lasted more than 25 seconds were also removed from the study.
All the patients were assessed preoperatively and premedicated with Alprazolam 0.5mg orally on the night before and 2 hours before surgery. In preoperative room baseline parameters were observed and documented. A good intravenous access was secured and all patients were pre-hydrated with 500ml of Ringer’s lactate. Now patients were randomly divided by computer into two groups. Group A received 1 mcg/kg of Inj. Dexmedetomidine in 100 ml of normal saline over 10 minutes and 5ml of normal saline 3 minutes before induction. Group B received 100 ml of normal saline over 10 minutes and Inj. Fentanyl 2 mcg/kg diluted in 5 ml of normal saline 3 minutes before induction. These solutions of 100 ml and 5 ml were prepared by first anaesthesiologist and labeled them as group A and B accordingly. The second anaesthesiologist, who was not aware of the groups, administered the drug and monitored the patients recording vital parameters. The laryngoscopy and intubation were performed by the third anaesthesiologist who was also blinded to the drug given. If the patient develops any complications then it was planned to stop drug infusions immediately and treat complications accordingly. After preoxygenation patients were induced with Inj. Propofol in a dose of 2.5 mg/kg body weight over 30 seconds to all patients in both groups and followed by Inj. Vecuronium 0.1mg/kg body weight after confirming a lack of response to voice and a loss of the eyelid reflex. Patients were ventilated with 50% nitrous oxide and Sevoflurane 1% for 3 minutes. Endotracheal intubation was performed by an experienced anaesthesiologist with the appropriate size cuffed endotracheal tube. Anaesthesia was maintained with controlled ventilation with nitrous oxide 66% and oxygen 33% with Sevoflurane 1.6%. No surgical stimulation was allowed for 10 minutes after intubation.
Statistical Analysis
The heart rate, systolic blood pressure and diastolic blood pressure were monitored before induction, after study drug, during laryngoscopy and intubation and thereafter for succeeding ten minutes at an interval of one minute and any complications noted. Results were tabulated. The data obtained were analysed statistically. Statistical analysis was carried out using student’s t-test and chi-square test. Demographic Data was analysed using students t-test and chi-square test was applied whenever there was a statistically significant difference between two different sets of data for each variable. Power analysis was perf ormed using SPSS version 15 for windows and for effective sample size on the basis of haemodynamic differences. The information collected regarding all the cases were recorded in master chart. The Mean, Standard Deviation, X2, ‘P’ values were calculated. A p-value less than 0.05 was taken to denote significant relationship.
Results
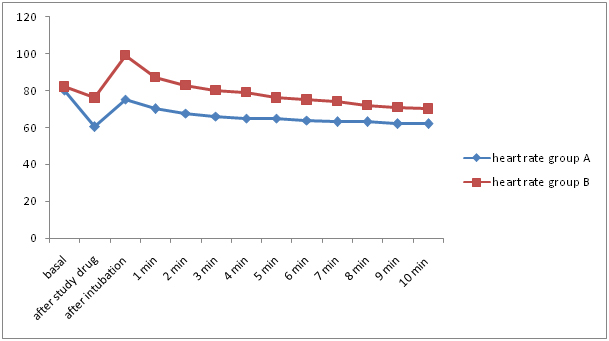
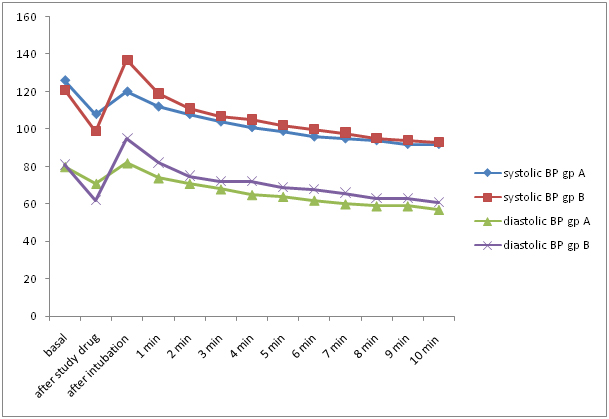
The demographic data were comparable in both the groups and are given in [Table/Fig-1]. There was no significant difference in basal heart rate and blood pressure and is given in [Table/Fig-2,3]. In dexmedetomidine group, the mean heart rate decreased after the administration of study drug and did not rise much beyond basal levels during or after intubation. In fentanyl group, the mean heart rate decreased after the administration of the study drug but it increased significantly beyond the basal values following intubation. The mean heart rate returned to basal levels only after 2 minutes but still it remained higher than the dexmedetomidine group. Only one patient developed bradycardia in the dexmedetomidine group which responded well to atropine. The variations in heart rate in both the groups are given in [Table/Fig-2,4]. The mean blood pressure decreased after dexmedetomidine infusion and after intubation, it did not increase beyond the basal levels. In fentanyl group though there was a slight reduction in blood pressure after drug administration blood pressure increased after intubation and returned to basal values after 1-2 minutes. The variations in blood pressure are given in [Table/Fig-2,3,5].
| Demographic characteristics | Group A | Group B |
|---|
| Age | 32.47 ± 10.39 | 31.27 ± 10.43 |
| Gender [M/F] | 18/ 12 | 15/ 15 |
| Weight | 58.63 ± 13.41 | 60.40 ± 12.95 |
Changes in heart rate and mean arterial pressure at various time intervals
| Time | Heart rate | Mean arterial pressure |
|---|
| Group A | Group B | p value | Group A | Group B | p value |
|---|
| Basal | 80.13 ± 11.6 | 81.97± 8.51 | 0.598NS | 97.1 ± 14.59 | 94.2 ± 8.93 | 0.352NS |
| After study drug | 60.3± 9.46 | 76.20± 17.37 | 0.001*** | 83.7 ± 12.12 | 73.6 ± 12.36 | 0.002** |
| After intubation | 75.10± 13.92 | 99.87± 19.78 | 0.001*** | 95.2 ± 16.92 | 109 ± 20.36 | 0.006** |
| 1 min | 70.03± 12.34 | 87.17± 17.67 | 0.001*** | 87.2 ± 13.19 | 94.7 ± 16.66 | 0.060NS |
| 2 min | 67.63± 11.52 | 83.50± 17.52 | 0.001*** | 83.3 ± 11.09 | 86.7 ± 15.58 | 0.325NS |
| 3 min | 66.60± 10.93 | 80.90± 18.09 | 0.001*** | 80.3 ± 10.62 | 83.9 ± 15.21 | 0.292NS |
| 4 min | 65.97± 10.16 | 79.47± 16.91 | 0.001*** | 77.7 ± 10.73 | 83.1 ± 14.12 | 0.099NS |
| 5 min | 65.23± 10.18 | 76.37± 16.49 | 0.003** | 75.8 ± 11.28 | 80.6 ± 13.17 | 0.135NS |
| 6 min | 64.60± 9.59 | 75.37± 16.21 | 0.003** | 73.9 ± 10.45 | 79.1 ± 12.49 | 0.082NS |
| 7 min | 63.83± 8.86 | 73.93± 16.02 | 0.004** | 73.0 ± 10.55 | 77.1 ± 11.24 | 0.147NS |
| 8 min | 63.50± 8.82 | 72.47± 15.44 | 0.008** | 71.4 ± 11.58 | 74.3 ± 10.04 | 0.316NS |
| 9 min | 62.87± 9.51 | 71.17± 15.53 | 0.015* | 70.4 ± 10..80 | 73.5 ± 9.90 | 0.251NS |
| 10 min | 62.40± 9.22 | 70.10± 15.51 | 0.023* | 69.4 ± 10.84 | 72.2 ± 9.53 | 0.292NS |
*Significant, ** Highly significant, *** Very highly significant
Changes in systolic and diastolic arterial pressure at various time intervals
| Time | Systolic blood pressure | Diastolic blood pressure |
|---|
| Group A | Group B | p value | Group A | Group B | p value |
|---|
| Basal | 126.53 ± 16.12 | 121.53 ± 10.02 | 0.147NS | 80.20 ± 11.64 | 81.27 ± 8.30 | 0.684NS |
| After study drug | 108.03 ± 12.19 | 99.30 ± 13.07 | 0.010* | 71.23 ± 12.03 | 62.57 ± 12.38 | 0.008** |
| After intubation | 120.77 ± 18.71 | 137.53 ± 24.26 | 0.004* | 82.30 ± 16.72 | 95.30 ± 18.58 | 0.006** |
| 1 min | 112.20 ± 14.28 | 119.50 ± 20.54 | 0.115 NS | 74.40 ± 13.37 | 82.07 ± 14.98 | 0.041* |
| 2 min | 108.50 ± 11.83 | 111.10 ± 18.02 | 0.512NS | 71.10 ± 11.55 | 75.70 ± 14.41 | 0.178NS |
| 3 min | 104.63 ± 11.24 | 107.40 ± 17.59 | 0.471NS | 68.17 ± 11.22 | 72.53 ± 14.76 | 0.202NS |
| 4 min | 101.83 ± 11.16 | 105.93 ± 15.87 | 0.252NS | 65.67 ± 11.15 | 72.63 ± 13.64 | 0.034* |
| 5 min | 99.43 ± 11.97 | 102.80 ± 14.45 | 0.330NS | 64.27 ± 11.55 | 69.60 ± 13.04 | 0.099NS |
| 6 min | 96.77 ± 11.20 | 100.37 ± 13.68 | 0.270NS | 62.33 ± 11.26 | 68.13 ± 13.53 | 0.076NS |
| 7 min | 95.63 ± 10.63 | 98.23 ± 12.51 | 0.389NS | 60.93 ± 11.63 | 66.10 ± 11.95 | 0.095NS |
| 8 min | 94.00 ± 11.29 | 95.90 ± 12.25 | 0.535NS | 59.87 ± 12.01 | 63.83 ± 10.50 | 0.179NS |
| 9 min | 92.77 ± 11.16 | 94.97 ± 11.17 | 0.449NS | 58.97 ± 12.01 | 63.83 ± 10.50 | 0.185NS |
| 10 min | 92.20 ± 11.27 | 93.73 ± 10.69 | 0.591NS | 57.83 ± 11.86 | 61.33 ± 10.26 | 0.227NS |
*Significant, ** Highly significant, *** Very highly significant
Changes in blood pressure
Discussion
The sympathomimetic stress response to laryngoscopy and intubation results in an increase in the myocardial oxygen demand and may lead to ischemia and acute heart failure in susceptible individuals. Hypertension and tachycardia during laryngoscopy can occur even in normotensive individuals and is rather surprising that complications have not been met very often probably because of its transient nature. Though numerous drugs have been tried to obtund haemodynamic response, none of them are totally satisfactory.
An advantage with dexmedetomidine is its ability to provide a dose dependent sedation allowing it to be useful for cooperative sedation in remote locations. Because of its pharmacological profile, dexmedetomidine can be used as an anaesthetic adjuvant and also for intensive care unit sedation [13]. Fentanyl acts on the opioid receptors, mainly μ receptors, for its analgesic action. Because of its ability to reduce sympathetic outflow, it brings about haemodynamic stability. Fentanyl is used routinely as part of general anaesthesia in a dose of 2 mcg/kg and this dose is effective for stress attenuation when given five minutes before laryngoscopy [14].
In the present study, heart rate was significantly decreased in the dexmedetomidine group when compared to fentanyl group immediately after study drug and there was statistically significant reduction in heart rate for up to 10 min after intubation in the dexmedetomidine group. In fentanyl group, heart rate increased following laryngoscopy and endotracheal intubation and returned back to normal only after 3 minutes. The attenuation in systolic, diastolic and mean arterial pressure was significantly better in the dexmedetomidine group than the fentanyl group. This finding was also observed by Laha et al., and Bloor et al., [7,19,20]. In dexmedetomidine group, systolic and diastolic blood pressure did not rise significantly following laryngoscopy and endotracheal intubation. With dexmedetomidine, mean systolic and diastolic blood pressure returned to baseline value within 1 minute after intubation, whereas in fentanyl group it was 2 minutes.
Laha et al., studied the effects of preinduction loading dose of dexmedetomidine 1 mcg/kg on attenuation of sympathoadrenal responses and requirements of anaesthetic agents [7]. They concluded that administration of dexmedetomidine not only attenuates the rise in mean heart rate, systolic blood pressure after intubation at 1, 2, 3 and 5 min but also significantly reduces the requirement of anaesthetic drugs. The dose of dexmedetomidine used and the results were similar to our study. Scheinin et al., performed a study on the effect of dexmedetomidine on tracheal intubation and dose of thiopentone and fentanyl needed for the surgery [12]. They observed that dexmedetomidine not only attenuates the haemodynamic responses to intubation but also reduces the doses of thiopentone and fentanyl. The plasma catecholamine concentration was measured in this study and it was found that the concentration of noradrenaline in mixed venous plasma was lesser in the dexmedetomidine group during all phases of induction. This study measured plasma catecholamine levels which was not possible in our study.
Sulaiman et al., studied the efficacy of dexmedetomidine on attenuation of stress response to endotracheal intubation in patients undergoing elective off pump coronary artery bypass grafting [13]. They concluded that administration of dexmedetomidine at a dose of 0.5mcg/kg over 10 min before induction of general anaesthesia decreases the heart rate and blood pressure following laryngoscopy and intubation for up to 5 minutes in patients undergoing myocardial revascularization. This study did not report any complications like hypotension or arrhythmias. Since this study was done on cardiac patients unlike normal patients in our study, they have used a lower dose than us.
Jaakola et al., did a study with dexmedetomidine in a dose of 0.6mcg/kg and observed that dexmedetomidine reduces the increase in heart rate and blood pressure during intubation [21]. The dosage used in these studies was less than the dose used by us. Lawrence et al., performed a study with a single dose of 2mcg/kg of dexmedetomidine before induction of anaesthesia and observed that it attenuated the haemodynamic response to both intubation and extubation [22]. Bradycardia was observed at the 1st and 5th min after administration and this might have been due to bolus administration of a large dose when compared to our study. Saraf et al., studied the effect of dexmedetomidine 0.6mcg/kg on stress response and found that bolus administration of 0.6mcg/kg administered 10 minutes before induction obtunds stress response in both adult and paediatric patients [23].
Gurulingappa et al., did a study comparing lignocaine and fentanyl for stress attenuation. They concluded that fentanyl at 4mcg/kg was more effective than lignocaine in attenuating the stress response [14]. Fentanyl was employed in a higher dose compared to our study. Since we felt fentanyl in a dose of 4mcg/kg could have an impact on postoperative recovery, we used the conventional dose of 2mcg/kg in our study. Gandhi et al., performed a study comparing dexmedetomidine in a dose of 0.6mcg/kg with fentanyl 2mcg/kg for stress attenuation. They observed that dexmedetomidine was effective in attenuating hear rate and blood pressure for up to 10 minutes after intubation [18]. In our study heart rate control was achieved for 10 minutes, but there was a statistically significant difference in blood pressure control for 1min only.
Several studies have highlighted that the use of dexmedetomidine in a dose of 0.5mcg/kg to 1mcg/kg is effective in obtunding haemodynamic stress response following laryngoscopy and intubation. The findings of all these studies were comparable to our study.
Limitations
One of the limitations of our study is that we did not measure plasma catecholamine levels, which was not feasible in our institute.
Conclusion
It is concluded that bolus injection of dexmedetomidine 1mcg/kg given intravenously over 10 minutes prior to intubation provided consistent and reliable protection against the pressor response during laryngoscopy and endotracheal intubation when compared to fentanyl group and is devoid of any major complications.
*Significant, ** Highly significant, *** Very highly significant
*Significant, ** Highly significant, *** Very highly significant
[1]. Shibman AJ, Smith G, Achola KJ, Cardiovascular and catecholamine responses to laryngoscopy with and without tracheal intubationBr J Anaesth 1987 59:295-99. [Google Scholar]
[2]. Longnecker DE, Alpine anaesthesia: Can pretreatment with clonidine decrease the peaks and valleys?Anaesthesiology 1987 67:1-2. [Google Scholar]
[3]. Rose DK, Cohen MM, The airway: Problems and predictions in 18500 patientsCan J Anaesth 1991 41:372-83. [Google Scholar]
[4]. Kovac AL, Controlling the haemodynamic response to laryngoscopy and endotracheal intubationJournal of Clinical Anaesthesia 1996 8:63-79. [Google Scholar]
[5]. Prys-Roberts C, Green LT, Meloche R, Studies of anaesthesia in relation to hypertension II - Haemodynamic consequences of induction and endotracheal intubationBr J Anaesth 1971 43:531-47. [Google Scholar]
[6]. Dalton B, Guiney T, Myocardial ischemia from tachycardia and hypertension in coronary heart disease – Patients undergoing anaesthesia 1972 BostonAnn Mtg American Society of Anaesthesiologists:201-2. [Google Scholar]
[7]. Laha A, Ghosh S, Sarkar S, Attenuation of sympathoadrenal responses and anaesthetic requirement by dexmedetomidineAnaesth Essays Res 2013 7:65-70. [Google Scholar]
[8]. Aantaa R, Scheinin M, α-2-adrenergic agents in anaesthesiologyActa Anaesthesiol Scand 1993 37:433-48. [Google Scholar]
[9]. Quintin L, Bonnet F, Macquin I, Aortic surgery: Effect of clonidine on intraoperative catecholaminergic and circulatory stabilityActa Anaesthesiol Scand 1990 34:132-37. [Google Scholar]
[10]. Keith A, Sergio D, Paula M, Marc A, Wisemandle W, Alex Y, Monitored anaesthesia care with dexmedetomidine: A prospective, randomized, double-blind, multicenter trialAnaesth Analg 2010 110:47-56. [Google Scholar]
[11]. Aho M, Lehtnen AM, Erkola O, The effect of intravenously administered dexmedetomidine on perioperative haemodynamics and isoflurane requirements in patients undergoing abdominal hysterectomyAnaesthesiology 1991 74:997-1002. [Google Scholar]
[12]. Scheinin B, Lindgren L, Randell T, Scheinin H, Scheinin M, Dexmedetomidine attenuates sympatoadrenal responses to tracheal intubation and reduces the need for thiopentone and peroperative fentanylBr J Anaesth 1992 68:126-31. [Google Scholar]
[13]. Sulaiman S, Karthekeyan RB, Vakamudi M, Sundar AS, Ravullapalli H, Gandham R, The effects of dexmedetomidine on attenuation of stress response to endotracheal intubation in patients undergoing elective off-pump coronary artery bypass graftingAnn Card Anaesth 2012 15:65-70. [Google Scholar]
[14]. Gurulingappa MAA, Aleem A, Awati MN, Adarsh S, Attenuation of Cardiovascular Responses to Direct Laryngoscopy and Intubation-A Comparative Study Between iv Bolus Fentanyl, Lignocaine and Placebo(NS)Journal of Clinical and Diagnostic Research 2012 6(10):1749-52. [Google Scholar]
[15]. Gogus N, Akan B, Serger N, Baydar M, The comparison of the effects of dexmedetomidine, fentanyl and esmolol on prevention of haemodynamic response to intubationBrazil Journal of Anaesthesiaology 2014 64(5):314-19. [Google Scholar]
[16]. Bhagat M, Kumar M, Khanna R, Suwalka U, A Comparison of Intravenous Dexmedetomidine V/S Inj. Fentanyl for Attenuation of Haemodynamic Responses during Laryngoscopy and Intubation after Propofol InductionNational Journal of Integrated Research in Medicine 2014 5(3):71-75. [Google Scholar]
[17]. Aksu R, Akın A, Bicer C, Esmaoglu A, Tosun Z, Boyacı A, Comparison of the Effects of Dexmedetomidine VersusFentanyl on Airway Reflexes and Haemodynamic Responses to Tracheal Extubation During Rhinoplasty: A Double-Blind, Randomized, Controlled StudyCurrent Therapeutic Research 2009 70(3):209-20. [Google Scholar]
[18]. Gandhi S, Goyal V, Radhakrishnan K, Balakrishnan M, Comparison of Dexmedetomidine with Fentanyl in Attenuation of Pressor Response during Laryngoscopy and IntubationIOSR Journal of Pharmacy 2014 4(2):28-38. [Google Scholar]
[19]. Bloor BC, Ward DS, Belleville JP, Maze M, Effects of intravenous dexmedetomidine in humans. II. Haemodynamic changesAnaesthesiology 1992 77:1134-42. [Google Scholar]
[20]. Bajwa SS, Kaur J, Singh A, Attenuation of pressor response and dose sparing of opioids and anaesthetics with preoperative dexmedetomidineIndian J Anaesth 2012 56:123-28. [Google Scholar]
[21]. Jaakola ML, Ali-Melkkilä T, Kanto J, Kallio A, Scheinin H, Scheinin M, Dexmedetomidine reduces intraocular pressure, intubation responses, and anaesthetic requirements in patients undergoing ophthalmic surgeryBr J Anaesth 1992 68:570-75. [Google Scholar]
[22]. Lawrence CJ, De Lange S, Effects of a single preoperative dexmedetomidine dose on isoflurane requirements and peri-operative haemodynamics stabilityAnaesthesia 1997 52:736-44. [Google Scholar]
[23]. Saraf R, Jha M, Kumar S, Damani K, Bokil S, Galante D, Dexmedetomidine, the ideal drug for attenuating the pressor responsePediatric Anaesthesia and Critical Care Journal 2013 1(1):78-86. [Google Scholar]