Group-A rotaviruses are responsible for 30 to 60% of all cases of severe watery diarrhea in young children [1]. In India, one out of every 250 children or about 100-150,000 children die of rotavirus diarrhoea each year [2]. Timely diagnosis of rotavirus infection in patients with acute gastroenteritis helps to determine the appropriate treatment, prevents unnecessary use of antibiotics and minimizes the spread of the disease [3]. Several methods available for detecting the rotavirus in stool specimen include Latex agglutination (LA), Enzyme-linked immunosorbent assays (ELISA), Polyacrylamide gel electrophoresis (PAGE) and Reverse transcriptase- polymerase chain reaction (RT-PCR) [4]. The latex technology has been extensively used for rapid test purpose. However, it is less sensitive than ELISA, needs more skill for results interpretation and cannot be archived. Recently, ICG has become available. This test is reliable, economical, fastest and easiest to perform [5]. Hence the present study was undertaken to compare new ICG with standard ELISA test for the diagnosis of rotavirus infection in children below five years. We also determined the incidence, clinical and socio-epidemiological profile and the possible risk factors associated with the rotavirus infection.
Materials and Methods
A prospective study was undertaken between February 2013 to April 2014 in the Microbiology and Paediatrics Department, Government Medical College, Amritsar, Punjab, India. Written & Informed consent with history was taken from the parents of children below five years. Approval of ethical committee was taken.
Hundred stool samples from children below five years diagnosed with acute gastroenteritis were taken from Paediatric ward of Bebe Nanki Mother and Child Care Centre, Guru Nanak Dev Hospital, Amritsar and tested by both ICG and standard ELISA. Socio-economic status of the family was assessed according to Kuppuswamy’s socio-economic scale 2012 and malnutrition status according to Indian academy of Paediatrics classification (IAP).
Freshly passed stool samples were collected in wide mouth sterilized container from hospitalized children with acute gastroenteritis by the help of their parents or caretaker and transported to the Microbiology department for laboratory testing. Samples were kept at 4°C and tested within 24 hours of collection. Rotavirus antigen detection was carried out by SD Bioline rotavirus one step test kit (Immunochromatographic test) and DRG rotavirus ELISA kit according to manufacturer’s instruction [6,7].
Statistical Analysis
Statistical analysis was performed by the SPSS program for Windows, version 17.0. Continuous variables are presented as mean ± SD, and categorical variables are presented as absolute numbers and percentage. Data were checked for normality before statistical analysis. Normally distributed continuous variables were compared using the unpaired t-test, whereas the Mann-Whitney U-test was used for those variables that were not normally distributed. By using either chi square test or Fisher’s exact test categorical variables were analysed. A p-value less than 0.05 were taken to indicate a significant difference for all statistical tests.
Results
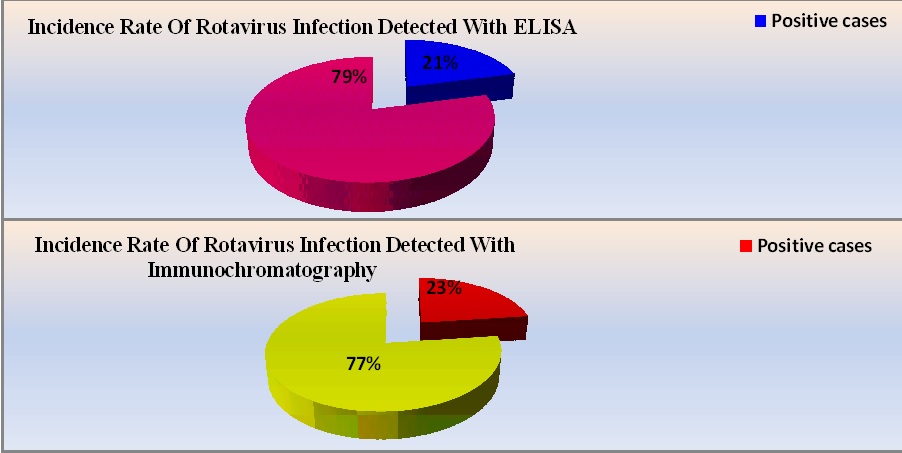
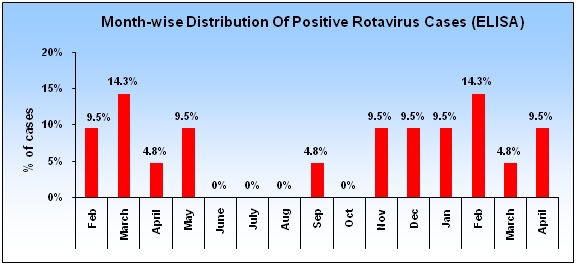
When ICG was compared to standard ELISA it showed a sensitivity of 95.24% and specificity of 97.47% [Table/Fig-1,2]. Rotavirus was found to be a common cause of acute gastroenteritis in children less than 5 years in and around Amritsar city with an incidence of 21% using ELISA and 23% using ICG [Table/Fig-3]. The infection was maximum during the months of November to April [Table/Fig-4]. Clinical, socio-economical profile and possible risk factors were also determined by standard test ELISA. It was highest in age group 6 months to 24 months (83.3%) followed by children of age group less than 6 months [Table/Fig-5]. Male children (90.47%) were affected more than female (9.52%) [Table/Fig-5]. There was no statistically significant difference in the frequency of rotavirus infection among patients from urban and rural areas and in different Kuppuswamy’s classes [Table/Fig-5]. Maximum number (76.2%) of rotavirus positive cases by ELISA presented with a triad of diarrhea, vomiting and fever followed by vomiting preceding diarrhea (19.0%) and diarrhea alone (4.8%) [Table/Fig-6]. Association of respiratory symptoms (38.09%) and severe dehydration (76.19%) with rotavirus infection was statistically significant [Table/Fig-6]. Majority (90.47%) of rotavirus positive cases by ELISA had watery diarrhea followed by mucoid diarrhea (9.52%) [Table/Fig-6]. Maximum cases (52.38%) of rotavirus diarrhea were on bottle feeding followed by breast feeding (28.57%) and mixed feeding (19.04%) [Table/Fig-7]. 47.61% of rotavirus diarrhea was malnourished [Table/Fig-7]. Out of these, 33.33% had grade-I malnutrition, 9.52% grade- III malnutrition and 4.76% grade IV malnutrition [Table/Fig-7]. Among possible risk factors, associations of rotavirus infection with children using toys and submersible water pump as a source of drinking water were found to be statistically significant [Table/Fig-8].
Total number of positive and negative cases observed with immunochromatography test as compared to ELISA
| Negative | Positive | Total |
|---|
| ELISA | 79 | 21 | 100 |
| ICG | 77 | 23 | 100 |
Diagnostic efficacy of immunochromatography test when compared with ELISA
| Immunochromatography | ELISA |
| Negative | Positive | Total |
|---|
| Negative | 77 | 01 | 78 |
| Positive | 02 | 20 | 22 |
| Total | 79 | 21 | 100 |
| (chi-square chart) |
| Diagnostic Efficacy Of Immunochromatography Test When Compared With ELISA |
| True Positive | 20 |
| False Positive | 2 |
| True Negative | 77 |
| False Negative | 1 |
| Sensitivity (%) | 95.24 |
| Specificity (%) | 97.47 |
| Positive Predictive Value (%) | 90.91 |
| Negative Predictive Value (%) | 98.72 |
| Accuracy (%) | 97 |
Incidence rate of rotavirus infection detected with immunochromatography and ELISA
Monthly distribution of rotavirus positive cases by ELISA
Distribution of patients with acute watery diarrhea according to their age, sex, residence and socioeconomic status
| Age (Months) | ELISA Negative | ELISA Positive | p-value |
|---|
| Number | % | Number | % |
|---|
| <=5 months | 4 | 5.1% | 3 | 14.3% | 0.049 |
| 6 - 12 months | 34 | 43.0% | 8 | 38.1% |
| 13- 24 months | 19 | 24.1% | 8 | 38.1% |
| 25 - 36 months | 10 | 12.7% | 2 | 9.5% |
| 37 - 48 months | 3 | 3.8% | 0 | 0.0% |
| 49 - 60 months | 9 | 11.4% | 0 | 0.0% |
| Total | 79 | 100% | 21 | 100% |
| Gender |
| Male | 50 | 63.3% | 19 | 90.5% | 0.017 |
| Female | 29 | 36.7% | 2 | 9.5% |
| Total | 79 | 100% | 21 | 100% |
| Location |
| Urban | 50 | 63.3% | 16 | 76.2% | 0.267 |
| Rural | 29 | 36.7% | 5 | 23.8% |
| Total | 79 | 100% | 21 | 100% |
| Socio Economic Class |
| Upper Middle Class | 10 | 12.7% | 7 | 33.3% | 0.078 |
| Upper Lower class | 52 | 65.8% | 10 | 47.6% |
| Lower Middle Class | 17 | 21.5% | 4 | 19.0% |
| Total | 79 | 100% | 21 | 100% |
Clinical profile of rotavirus – antigen positive cases
| Clinical Features | ELISA Negative (n=79) | ELISA Positive (n=21) |
|---|
| Number | % | Number | % |
|---|
| Diarrhea only | 5 | 6.3% | 1 | 4.8% |
| Diarrhea, Vomitting, Fever | 38 | 48.1% | 16 | 76.2% |
| Vomiting Preceding Diarrhea | 26 | 32.9% | 4 | 19.0% |
| Diarrhea And Fever | 10 | 13% | 0 | 0% |
| Associated Complaints | ELISA Negative | ELISA Positive | p-value |
|---|
| Number | % | Number | % |
|---|
| None | 76 | 96.2% | 13 | 61.9% | <0.001 |
| Seizures | 1 | 1.3% | 0 | 0.0% |
| URTI | 1 | 1.3% | 8 | 38.1% |
| Jaundice | 1 | 1.3% | 0 | 0.0% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Appearance of stool | ELISA Negative | ELISA Positive |
|---|
| Number | % | Number | % |
|---|
| Watery | 64 | 81.0% | 19 | 90.5% |
| Mucoid | 4 | 5.1% | 2 | 9.5% |
| Bloody | 11 | 13.9% | 0 | 0.0% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Grades of Dehydration | ELISA Negative | ELISA Positive | p-value |
|---|
| Number | % | Number | % |
|---|
| NO | 13 | 16.5% | 0 | 0.0% | <0.001 |
| Some | 53 | 67.1% | 5 | 23.8% |
| Severe | 13 | 16.5% | 16 | 76.2% |
| Total | 79 | 100% | 21 | 100% |
Distribution of rotavirus positive cases according to type of feeding and nutritional status
| Type of feeding | ELISA Negative | ELISA Positive | p-value |
|---|
| Number | % | Number | % |
|---|
| Breast Feeding | 57 | 72.2% | 6 | 28.6% | <0.001 |
| Bottle Feeding | 11 | 13.9% | 11 | 52.4% |
| Mixed Feeding | 11 | 13.9% | 4 | 19.0% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Grades of Malnutrition (IAP) |
| NO | 60 | 75.9% | 11 | 52.4% | 0.002 |
| Grade I | 13 | 16.5% | 7 | 33.3% |
| Grade II | 6 | 7.6% | 0 | 0.0% |
| Grade III | 0 | 0.0% | 2 | 9.5% |
| Grade IV | 0 | 0.0% | 1 | 4.8% |
| Grade II | 79 | 100% | 21 | 100% |
Possible risk factors associated with rotavirus infection
| Type of feeding | ELISA Negative | ELISA Positive | p-value |
|---|
| Number | % | Number | % |
|---|
| Tap Water | 59 | 74.7% | 8 | 38.1% | <0.001 |
| Hand Pump | 7 | 8.9% | 0 | 0.0% |
| Submersible | 13 | 16.5% | 13 | 61.9% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Type of Toilet Used |
| In Bushes | 3 | 3.8% | 0 | 0.0% | 0.657 |
| Flush Type | 68 | 86.1% | 19 | 90.5% |
| Sewage System | 8 | 10.1% | 2 | 9.5% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Location Of Toilet In Relation To Water Source |
| Outside house | 7 | 8.9% | 2 | 9.5% | 1.000 |
| Within house | 72 | 91.1% | 19 | 90.5% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Playing With Toys |
| No | 20 | 25.3% | 11 | 52.4% | 0.017 |
| Yes | 59 | 74.7% | 10 | 47.6% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Wash Child’s Hand After Every Visit To Toilet |
| No | 54 | 68.4% | 17 | 81.0% | 0.295 |
| Yes | 25 | 31.6% | 4 | 19.0% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Wash Child’s Hand Before Every Meal |
| No | 53 | 67.1% | 18 | 85.7% | 0.112 |
| Yes | 26 | 32.9% | 3 | 14.3% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Attends Day Care School |
| No | 73 | 92.4% | 21 | 100.0% | 0.338 |
| Yes | 6 | 7.6% | 0 | 0.0% |
| Total | 79 | 100.0% | 21 | 100.0% |
| Consumption Of Food That Need No Cooking |
| No | 55 | 69.6% | 17 | 81.0% | |
| Yes | 24 | 30.4% | 4 | 19.0% | 0.415 |
| Total | 79 | 100.0% | 21 | 100.0% | |
| Often Play With Children |
| No | 33 | 41.8% | 12 | 57.1% | 0.208 |
| Yes | 46 | 58.2% | 9 | 42.9% |
| Total | 79 | 100.0% | 21 | 100.0% |
Discussion
ELISA is the standard test for detection of rotaviruses but because of limited availability and rather high cost we compared ICG to ELISA. In our study sensitivity (95.24%) and specificity (97.47%) of ICG was comparable to ELISA and made the diagnosis simple, rapid, cost-effective and convenient. A study conducted by Momenzadeh A et al., Rougemont DA et al., and Kim J et al., also showed similar results [8–10].
Rotavirus accounting 20-50% of hospitalization for gastroenteritis in children worldwide and is the most important cause of severe, life threatening gastroenteritis in children [11]. The present study showed an incidence of 21% of rotavirus diarrhea with ELISA in children less than five years of age. The results of this study supported by the studies from other cities of India like Chandigarh (16-19%), Kolkata (5-22%) and Chennai (20.8%) [12].
Most of the infected children in our study were between 6 to 24 months of age (85.71%). It appeared that infants below 4 months of age were initially protected to some extent against rotavirus diarrhea due to presence of maternal antibodies to rotavirus infection and seemed to have acquired active immunity by 24 months of age [13]. This result is similar to other studies done in Eastern Nepal and other countries [14,15].
Males had significantly higher rates of rotavirus infection than females which may be due to the tendency of parents to take male children more than female to hospital for treatment. This may also be attributed to more resistance to infection in females due to XX chromosome. Respiratory symptoms are frequently seen with rotavirus gastroenteritis and 38.09% of our cases had such symptoms. There was a higher incidence during November to April. This winter peak could be due to additional droplet infection via respiratory tract in addition to feco-oral transmission [16].
In our study 90.47% of cases had watery diarrhea and majority (76.19%) presented with severe dehydration. This is due to elaboration of a potent enterotoxin which causes profuse watery diarrhoea and then destroys the intestinal epithelial surface leading to blunted villi, extensive damage, and shedding of massive quantities of virus in stools [11].
Various studies showed that exclusive breastfeeding provide only temporarily protection against severe rotavirus diarrhea [17]. In our study, we found statistically significant association between feeding and rotavirus positivity, with children on exclusive breast feeds having a reduced incidence of rotavirus diarrhea. Bottle feeding was independently associated with rotavirus diarrhea. This is because human milk contains human rotavirus specific antibodies and these antibodies are capable of neutralizing rotavirus antigens [17]. In our study maximum number (47.61%) of rotavirus positive cases were malnourished. This may be due to defects in their cellular and humoral immunity [18].
Another possible risk factor associated with rotavirus infection in our study was children using toys (p < 0.05). These toys can be easily contaminated by older children who may be asymptomatic carriers of the virus in their finger nails, hands etc. Children are seem to put objects into their mouths while playing or scratching their gums when they are about to start teething, such contaminated objects then serve as source of infection [19]. Submersible pump as a water source was also associated with higher incidence of rotavirus infection in our study. According to an official of Water and Sewage Department of Municipal Corporation Amritsar, submersible pump obtained water at a depth 150-250 feet is not fit for drinking as per their own testing laboratory.
Conclusion
Rotavirus is a common cause of acute gastroenteritis in children aged less than 5 years in and around Amritsar city. It is not routinely diagnosed in most of the hospitals probably due to the cost of its diagnosis and its clinical spectrum of signs and symptoms which are similar to other types of gastroenteritis. Few laboratories in India use ELISA as the method of diagnosis of rotavirus infection because of limited availability and rather higher cost. ICG when compared to standard test- ELISA showed a sensitivity of 95.24% and specificity of 97.47%. Hence ICG test shows good agreement with ELISA and has the advantage of being a quicker, cost-effective, useful for testing single specimen, convenient, not requiring additional equipment, readily available, simple to perform and easy-to-read results. Rotavirus was significantly associated with 6-24 months of age, male children, with respiratory tract infection, severe dehydration, bottle feeding, malnutrition, children playing with toys and submersible water pumps as a source of drinking water.