Penile Metastases From Prostate Adenocarcinoma: A Rare Presentation
Srikanth Soma1, Poorna Chander Reddy2, Rahul Bhat3, Shivananda Prabhu4
1 Senior Resident, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, India.
2 Associate Professor, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, India.
3 Assistant Professor, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, India.
4 Professor, Department of General Surgery, Kasturba Medical College, Mangalore, Manipal University, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Srikanth Soma, B-404, Amsri Residency, Ameerpet, Hyderabad, Telangana-500016, India. E-mail : soma_986@yahoo.co.in
Penile metastases are rare in occurrence and are usually secondary to other genitourinary primary tumours. It is a debilitating near terminal condition at presentation with a dismal prognosis and poor survival rates. Supportive and palliative care is generally recommended to improve the quality of life of patients. We present a case of penile metastases in a 74-year-old male patient with prostatic adenocarcinoma in association with multiple skeletal metastases.
Metastatic prostate cancer, Palliative care, Penile lesions
Case Report
A 74-year-old male patient presented with acute urinary retention and sudden onset paraparesis, to the Emergency Department. Physical examination revealed multiple non tender nodules involving the glans and shaft of penis [Table/Fig-1]. There were no palpable inguinal lymph nodes. Digital rectal examination revealed hard enlarged prostate with multiple nodules. Examination of the spine appeared normal. There was gross motor weakness including mild sensory loss involving both the lower limbs. Suprapubic cystostomy was performed to achieve urinary drainage.
Photograph revealing multiple nodules involving the glans and shaft of penis

The patient had been previously diagnosed with locally advanced prostatic adenocarcinoma 4 years back at another institution and was started on hormonal manipulation. The patient had incomplete details about the previous histologic and radiologic findings. Considering the general status of the patient and the obvious clinical findings, was planned not to put the patient through multiple invasive procedures and focus was put on providing palliative care. On admission prostate specific antigen (PSA) was grossly elevated (227 ng/mL).
The CT scan revealed features of prostate adenocarcinoma with no other gross abnormalities. Bulky growth involving the prostate with extracapsular extension and involves the seminal vesicles. No lymph node enlargement noted. In view of paraparesis, bone scan and MRI of spine were done which revealed multiple metastatic lesions involving the vertebrae and pelvic bones.
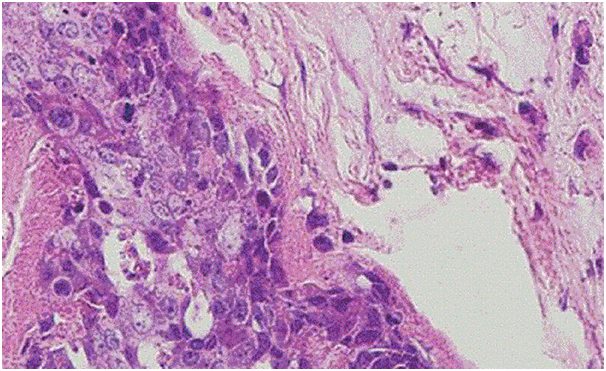
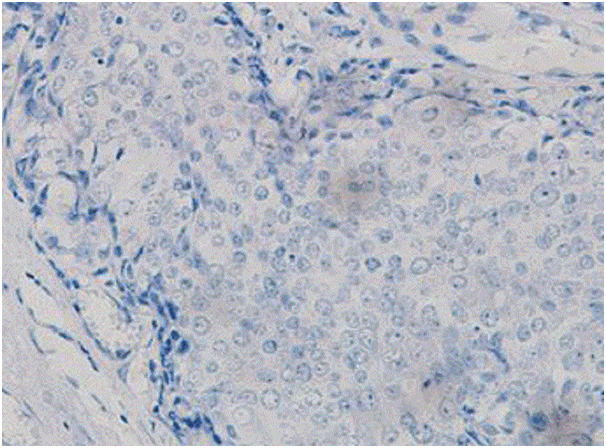
A core biopsy of penile lesion was obtained for histopathology, which showed features suggestive of poorly differentiated adenocarcinoma [Table/Fig-2]. Immunohistochemical staining for PSA was negative [Table/Fig-3]. Similar presentation of penile metastases with PSA negativity was published. Diagnosis of penile metastases was considered because the clinical and imaging findings most likely matched metastatic prostatic adenocarcinoma and being previously diagnosed with prostate cancer. In view of general condition of the patient and poor prognosis, he was put on palliative care to improve his quality of life. On follow up, the patient had succumbed to the disease within 4 months. Metastatic penile tumours are extremely rare.
Microscopic picture (H&E staining) showing features suggestive of poorly differentiated adenocarcinoma (200X magnification)
Immunohistochemistry showing PSA staining negative (200X magnification)
Discussion
A search through the literature, 219 cases of penile metastases was identified, among which genitourinary cancers were the most common primaries [1]. Metastatic penile cancer from prostate adenocarcinoma was reported in very few cases. The most common presentations were nodules over penis, followed by priapism, pain during erection and dysuria in few cases. The following mechanisms have been described as causes of metastases to penis from prostate adenocarcinoma by Abehouse - direct invasion, implantation, haematogenous dissemination and lymhatic dissemination [2]. The prognosis remains poor in this group of patients. In one of the studies conducted in Japan, 71% of patients died within 6 months of such a diagnosis [3]. There are a number of treatment options depending on the general status of the patient, location and extent of the primary tumour and symptomatology such as local excision, radiation therapy, bilateral orchiectomy, hormonal manipulation, systemic chemotherapy and partial/total amputation of the penis in severely symptomatic cases (intractable pain, uncontrollable bleeding). Like the presentation in our case, patients who present with obstruction to urinary outflow, procedures such as suprapubic cystostomy or suprapubic catheterisation can be of palliative value [4]. Penile metastases from prostate adenocarcinoma should never be ruled out based on PSA negativity on immunohistochemistry when the history, clinical and imaging findings suggest otherwise as was the presentation in this case and a similar case published previously [5].
Conclusion
Metastatic prostatic cancer presents with various signs and symptoms and one should keep in mind the possibility of penis as the site for metastasis. Management of such patients with penile metastases from adenocarcinoma of the prostate should be more on improving their quality of life with multitude of palliative options rather putting the patient through a morbid systemic/surgical therapy.
[1]. Ansari H, Prasant R, Franks A, Prostatic carcinoma metastasis to the penis – an uncommon siteLancet Oncol 2003 4:705-06. [Google Scholar]
[2]. Abehouse BS GA, Metastatic tumours of the penis; a review of literature and report of two casesJ Urol 1961 86:99 [Google Scholar]
[3]. Kotake Y, Gohji K, Suzuki T, Watsuji T, Kusaka M, Takahara K, Metastases to the penis from carcinoma of the prostateInt J Urol 2001 8:83-86. [Google Scholar]
[4]. Osther PJ, Lontoft E, Metastasis to the penis: case reports and review of the literatureInt Urol Nephrol 1991 23:161-67. [Google Scholar]
[5]. Dijkstra S, van der Heijden AG, Schaafsma HE, Synchronous penile metastasis from a high-grade adenocarcinoma of the prostateCase Rep Urol 2012 2012:193787 [Google Scholar]