Anaesthetic Efficacy of Topical Benzocaine Gel Combined with Hyaluronidase for Supplemental Intrapulpal Injection in Teeth with Irreversible Pulpitis- A Double Blinded Clinical Trial
Sujatha Gopal Sooraparaju1, M. Abarajithan2, Emmanuel Solomon Sathish3, Nujella Bhaskara Padma Suryakumari4, Kranti Kiran Reddy Ealla5, Winner Gade6
1 Professor & Head, Department of Conservative Dentistry and Endodontics, MNR Dental College, Telangana, India.
2 Director, Smile Bright Root Canal Academy, Madurai, India.
3 Professor & Head, Department of Conservative Dentistry and Endodontics, Ultra’s Best Dental College, Madurai, Telangana, India.
4 Reader, Department of Conservative Dentistry And Endodontics, MNR Dental College, Telangana, India.
5 Reader, Department of Oral And Maxillofacial Pathology, MNR Dental College, Telangana, India.
6 Post Graduate, Department of Conservative Dentistry and Endodontics, MNR Dental College, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kranthi Kiran Reddy Ealla, Associate Professor, MNR Dental College & Hospital, Sangareddy, Medhak District, Telangana, India. E-mail : drekkr@yahoo.co.in
Objective
Intrapulpal injection technique is one of the most commonly employed method to achieve profound pulpal anaesthesia during an endodontic procedure. To determine if the topical application of benzocaine gel along with hyaluronidase to the pulp chamber could reduce the pain felt with the intrapulpal injection technique.
Materials and Methods
Two hundred patients with chronic irreversible pulpitis undergoing endodontic treatment for mandibular first molars in which the primary anaesthetic technique failed were selected and randomly divided into 2 groups. In the control group intrapulpal injection was administered with backpressure. In the experimental group topical application of 20% benzocaine gel mixed with hyaluronidase was done over the exposed pulp following which intrapulpal injection was administered with backpressure. Pain assessment was done on a visual analogue scale.
Results
There was statistically significant difference (p<0.001) between the two groups. The mean value in the control group corresponded to the pain perception "strong”, whereas that of the experimental group corresponded to the pain perception "weak”.
Conclusion
Topical application of 20% benzocaine gel mixed with hyaluronidase to the exposed pulp reduces the pain encountered with the intrapulpal injection.
Hot pulp, IAN block, Pulpal anaesthesia
Introduction
A painless endodontic therapy is made possible with the help of local anaesthesia. Local anaesthetics are more successful in exodontia but achieving profound pulpal anaesthesia is a frequent problem in endodontics especially in mandibular teeth with symptomatic pulpitis. The inferior alveolar nerve (IAN) block with 2% lidocaine is the frequently employed injection technique for achieving local anaesthesia for mandibular teeth in endodontics. Clinical studies in endodontics have found failure with the IAN block occurring 44%to 81 % of the time [1]. Wali et al., found that after administering IAN block, anaesthetic failure occurred in 17% first molar, 11% first premolar and 32% lateral incisors [2]. Also, onset of pulpal anaesthesia is longer after IANB, in 19 to 27% it took 16 minutes and in 8% cases it took even 30 minutes [3]. Studies have shown that even with the use of different local anaesthetic agents like articaine, bupivacaine, prilocaine [4] and various anaesthetic techniques like Gow-gates, Akinozi [5,6], there was not much difference in the success rates with achieving pulpal anaesthesia in mandibular teeth.
Thus clinically this problem is overcome with the help of one of the supplemental anaesthetic techniques like intrapulpal, intraosseous and intra-ligamentary injections [7]. The intrapulpal injection technique is commonly preferred in situations where patients encounter pain or discomfort during pulp extirpation. The most important factor in the success of intrapulpal technique is that the administration must be done underpressure. Birchfield and Rosenburg [8] suggested that the anaesthetic effect of the intrapulpal technique is due to the back-pressure of the solution and is not dependent on the type of solution injected. A number of methods such as obliterating a large pulpal opening with gutta-percha or a cotton pellet have been suggested to aid in the build-up of pressure [9]. According to Malamed SF the main drawback with this technique is that the intrapulpal injection by itself can be highly painful [10]. Hyaluronidase is an enzyme which is a spreading factor that acts by Hydrolysis of hyaluronic acid, a normal component of connective tissue and hence enhances the diffusivity of drugs injected along with it [11]. In the field of ophthalmology the combination of local anaesthesia with hyaluronidase for field blocks is a routinely used procedure as it has been proved to improve the speed of onset and quality of anaesthesia [12,13]. This combination was also tried in dentistry for IAN block, but did not gain popularity because it did not improve the efficacy of the block and the chances for postoperative pain and trismus was high as it was injected into a space [14]. However, Sathish et al., had found that hyaluronidase increased the duration of inferior alveolar nerve block [15].
Giving topical anaesthesia is a common practice. In this study we have tried applying a topical anaesthetic and hyaluronidase combination into the pulp chamber which could reduce the pain of the intrapulpal injection. This has never been tried before. Hence, the aim of our study was to evaluate if the topical application of 20% benzocaine gel mixed with hyaluronidase to the pulp chamber before administration of intrapulpal injection can reduce the pain encountered with the injection technique itself.
Materials and Methods
This prospective study was carried out in the year 2013-2014 in our Institution (Meenakshi Ammal Dental College and MNR Dental College). Two hundred patients treated endodontically during the 2 year period of this study who fell into the inclusion criteria were selected among the 796 patients treated during this period.
The subjects who were included are patients undergoing treatment for mandibular molars diagnosed as irreversible pulpitis based on history and subjective symptoms like spontaneous, nocturnal pain and lingering response to cold testing. Only healthy adults with no medical problems (by oral questioning) in the age group 20 to 35 years were selected. From these selected patients, teeth in which profound pulpal anaesthesia could not be achieved with primary inferior alveolar nerve block were selected for the study. The excluded patients are those who were diagnosed as irreversible pulpitis but who took analgesics in the past 5 days.
These patients were randomly divided into two groups. A blinded researcher randomly alloted the patient for a particular group who will not take part in assessing the efficacy of anaesthesia. The approval from the Ethical committee was obtained.
Anaesthetic success: Lack of profound pulpal anaesthesia was determined to be the situation if the patient experienced pain during chamber access when they had been comfortable with the treatment up to that point. The success of inferior alveolar nerve block was checked with an electric pulp tester and was considered successful if the tooth to be treated and adjacent tooth showed two consecutive 80 readings. If the block was found to be a success but still the inflamed pulp was not anaesthetized, to supplement the block anaesthesia initially administered, the intrapulpal injection was given into pulp chamber or during pulp extirpation. A patient who experienced pain while still in dentin was not included in the study. Patient consent to participate in the study was procured before giving the intrapulpal injection. Patients were selected in a random manner to receive one or the other of the two techniques. There were 100 patients in each group.
Group 1 (Control Group): Intrapulpal injection of 2% lignocaine (1: 200000 adrenaline) (Xylocaine 2%; AstraZeneca Pharma India Ltd) a saline soaked cotton pellet was placed in the pulp chamber for 2 minutes as placebo, followed by intrapulpal injection with backpressure. In teeth were backpressure could not be achieved a cotton pellet was used to achieve backpressure. A standard anaesthetic syringe with 27-gauge needle was used to inject 0.5 ml of the solution within 5 seconds.
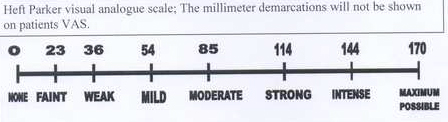
Group 2 (Experimental Group): Topical application of 20% benzocaine gel (Mucopain, ICPA Health products India Ltd.) mixed with hyaluronidase (Hynidase Shreya life sciences Pvt. Ltd) (1g with 300IU/ml sterile water) followed by intrapulpal injection of 2% lignocaine (1:200000 adrenaline). Hyaluronidase pellet in the vial was dissoluted with 5ml of distilled water provided by the manufacturer. Now 1ml from this solution was taken in a micropipette and dispensed into a dappen dish with 50 mg benzocaine gel measured with a custom made plastic scoop. An applicator tip was used to mix them. With the help of applicator tip 20% benzocaine gel mixed with hyaluronidase was placed over the exposed pulp for 2 minutes. Following this, intrapulpal injection of 2% lignocaine (1:200000 adrenaline) was administered with backpressure as in group 1. This study was double blinded in that neither the patient nor the person who did the pain assessment was aware of which technique was used. Each patient rated his or her pain sensation during the injection procedure on a Heft parker visual analogue scale 1. The visual analogue scale was divided into four categories. No pain corresponded to 0 mm, mild pain was defined as >0mm and ≤54mm. Mild pain included the descriptions of faint, weak and mild pain. Moderate pain was defined as ≥54mm and ≤ 114mm. Severe pain was defined as >114 mm and included the descriptions of strong, intense and maximum possible. The mean pain value calculated from the 100 raw data for each group in mm and standard deviation were computed and analysed by student-t-test at a significance level of 0.05 [Table/Fig-1].
Heft Parker visual analogue scale
Results
There was statistically significant difference between the two groups (p<0.001). The mean value in the control group was 121.56±21.37 which corresponded to the Pain category “strong”, whereas that of the experimental group was 36.35±9.23 which corresponded to the pain category "weak" [Table/Fig-2].
Mean and standard deviation of pain values calculated from the raw data
| GROUPS | MEAN PAIN VALUE (IN mm) ± STANDARD DEVIATION |
|---|
| Control group | 121.56±21.37 |
| Experimental group | 36.35±9.23 |
Discussion
The intrapulpal injection is an often used supplemental injection technique for achieving pulpal anaesthesia in teeth in which the primary anaesthetic technique fails to achieve profound pulpal anaesthesia. The intrapulpal injection technique has many advantages that it is technically simple, does not require removal of rubber dam and the systemic effects are negligible [7]. Moreover, anaesthesia can be achieved with any solution injected with back pressure. But the major draw back of this technique is that the intrapulpal injection itself is painful [7]. The topical application of the combination was done for two minutes because this is sufficient for the onset of action of topical anaesthetics [16]. We chose benzocaine gel because it has been proved that they reach higher concentrations at the sensory nerve endings [17]. Hyaluronidase increases the permeability of connective tissue and thus enhances the spread of local anaesthetics used in combination with them [12]. Thus we propose that the increase in the depth of anaesthesia with the topical application of 20% benzocaine gel mixed with hyaluronidase to the pulp prior to intrapulpal injection can eliminate or reduce the pain encountered with the injection technique itself. Hyaluronidase has been safely used in the field of ophthalmology and hence can be considered harmless in the oral cavity. In our present study there was statistically significant difference (p<0.00l) in pain perception between the two groups. The pain perception was "weak" in the group in which the topical application lignocaine gel mixed with hyaluronidase to the pulp preceded the intrapulpal injection. The better diffusivity of this topical anaesthetic with the aid of hyaluronidase is the suggested mechanism for rendering the intrapulpal injectionless painful.
Limitation of This Study
The limitation of this study is that it has been tried only in mandibular first molars. More extensive studies with increased sample size and different teeth are required to further recommend this technique for clinical endodontics.
Conclusion
Thus the topical application of benzocaine gel mixed with hyaluronidase to the exposed pulp prior to the administration of intrapulpal injection can make the intrapulpal injectionless painful.
[1]. Bigby J, Reader A, Nusstein J, Beck M, Weaver J, Anaesthetic efficacy ofarticaine for inferior alveolar nerve blocks in patients with irreversible pulpitisJ Endod 2004 30:568-71. [Google Scholar]
[2]. Wali M, Reader A, Beck M, Anaesthetic efficacy of lidocaine and epinephrine in human alveolar nerve blocksJ Endod 1988 14(4):193-96. [Google Scholar]
[3]. Simon F, Reader A, Meyer W, Evaluation of a peripheral nerve stimulator in human mandibular anaesthesiaJ Dent Res 1990 69(3):304-07. [Google Scholar]
[4]. Claffey E, Reader A, Nusstein J, Anaesthetic efficacy of articaine forinferior alveolar nerve blocks in patientswith irreversible pulpitisJ Endod 2004 30(8):568-71. [Google Scholar]
[5]. Gow-Gates GA, Mandibular conduction anaesthesia: a new technique using extraoral landmarksOral Surg Oral Med Oral Pathol 1973 36(3):321-28. [Google Scholar]
[6]. Sisk A, Evaluation of the Akinosimandibular block technique in oralsurgeryJ Oral Maxillofac Surg 1986 44(2):113-15. [Google Scholar]
[7]. Meechan JG, Supplementary routes to local anaesthesiaEndod J 2002 35:885-96. [Google Scholar]
[8]. Birchfield J, Rosenburg PA, Role of anaesthetic solution in intrapulpal anaesthesiaJ Endod 1975 1:26-27. [Google Scholar]
[9]. Van Gheluwe J, Walton R, Intrapulpal injection: factors related to effectivenessOral Surg Oral Med Oral Pathol Oral Radiol Endod 1997 83:38-40. [Google Scholar]
[10]. Malamed SF, The management of pain and anxiety.In: Cohen S Bums RC, EdsPathways of the pulp 1998 7th ednSt.LouisMosby:665-666. [Google Scholar]
[11]. Eckenhoff JE, Kirby CK, The use of hyaluronidase in regional nerve blocksAnaesthesiology 1951 12:27-32. [Google Scholar]
[12]. Bowman RJ, Newman DK, Richardson EC, Callear AB, Flanagan DW, Is hyaluronidase helpful for peribulbar anaesthesia?Eye 1997 11(Pt 3):385-88. [Google Scholar]
[13]. Dempsey GA, Barrett PJ, Kirby IJ, Hyaluronidase and peribulbar blockBr J Anaesth 1997 78:671-74. [Google Scholar]
[14]. Ridenour S, Reader A, Beck M, Weaver J, Anaesthetic efficacy of a combination of hyaluronidase and lidocaine with epinephrine in inferior alveolar nerve blocksAnaesth Prog 2001 48:9 [Google Scholar]
[15]. Satish SV, Shetty KP, Kilaru K, Bhargavi P, Reddy ES, Bellutgi A, Comparative evaluation of the efficacy of 2% lidocaine containing 1:200,000 epinephrine with and without hyaluronidase (75 IU) in patients with irreversible pulpitisJ Endod 2013 39(9):1116-18. [Google Scholar]
[16]. Friskopp J, Nilsson M, Isacsson G, The anaesthetic onset and duration of a newlidocaine/prilocaine gel intra-pocket anaesthetic (Oraqix) for periodontal scaling/rootplaningJ ClinPeriodontol 2001 28(5):453-58. [Google Scholar]
[17]. DeNunzio M, Topical anaesthesia as an adjunct to local anaesthesia during pulpectomiesJ Endod 1998 24:202-03. [Google Scholar]