Obturator artery (OA), one of the branches of the anterior division of the internal iliac artery, courses downwards and forwards on the lateral pelvic wall to reach the upper part of the obturator foramen, and leaves the pelvic cavity by the obturator canal [1]. Within the pelvis it gives off iliac, vesical and pubic branches. It divides into anterior and posterior branches to supply the medial compartment of the thigh. Posterior branch gives off the acetabular branch, which enters the hip joint [1].
The study of vascular pattern of the pelvis gains importance due to concentration of organs within the limited spacial confines of the pelvic cavity [2]. To successfully perform endoscopic total extraperitoneal inguinal hernioplasty (TEP) [3], or laparoscopic herniorrhaphy [4], a sound knowledge of retropubic vascular anatomy is pivotal. Major surgical interventions in the pelvis like extended organ resection following tumours, or sepsis due to perforation of pelvic organs, need ligation and transection of the supplying arteries and veins [5]. Aberrant obturator artery and vein may cross the superior pubic ramus and are therefore susceptible to injuries during dissection of the preperitoneal space of Bogros and stapling of the mesh [3]. Surgeons dealing with direct or indirect inguinal, femoral or obturator hernia need to know the variations of the OA and their close proximity to the femoral ring [6]. Sometimes, inadvertent injuries of involved or adjacent vessels require expertise in handling. To minimise blood loss or prevent subsequent acute or delayed ischaemia or venostasis, surgeons operating on the pelvic area should be familiar with the normal and pathological pelvic blood supply [5]. .
Materials and Methods
Fifty formalin-fixed hemipelvises (44 male and 6 female), were dissected in situ to study the variations in the origin of the OA. The OA was identified and traced from its origin to its exit at the obturator foramen. The course of the artery and its relations were noted and photographs were taken to document the variations. The study was done on hemipelvises available in the Department of Anatomy. Those pelvises where the OA was broken or where the origin or course could not be inferred were excluded from the study. The study was carried out over a period of 8 months.
Results
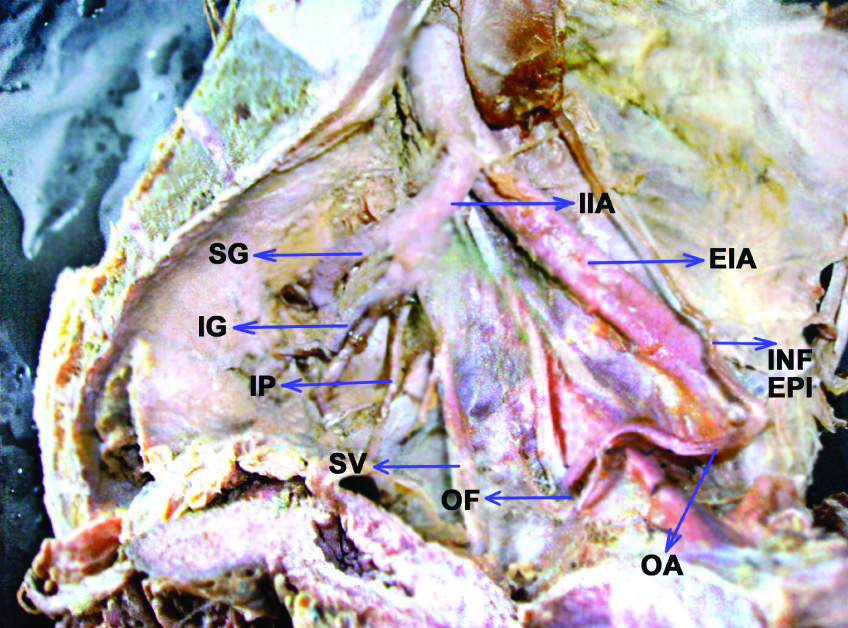
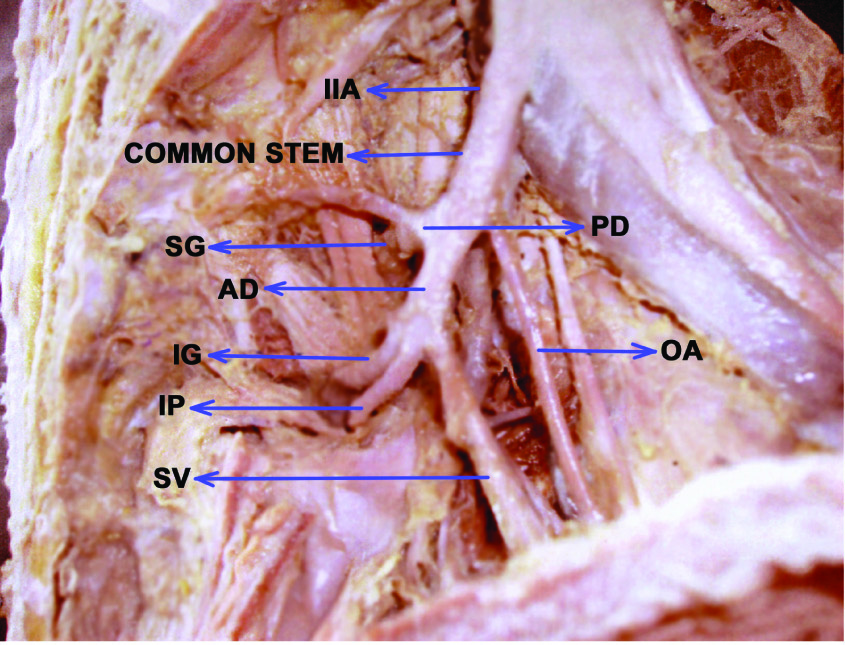
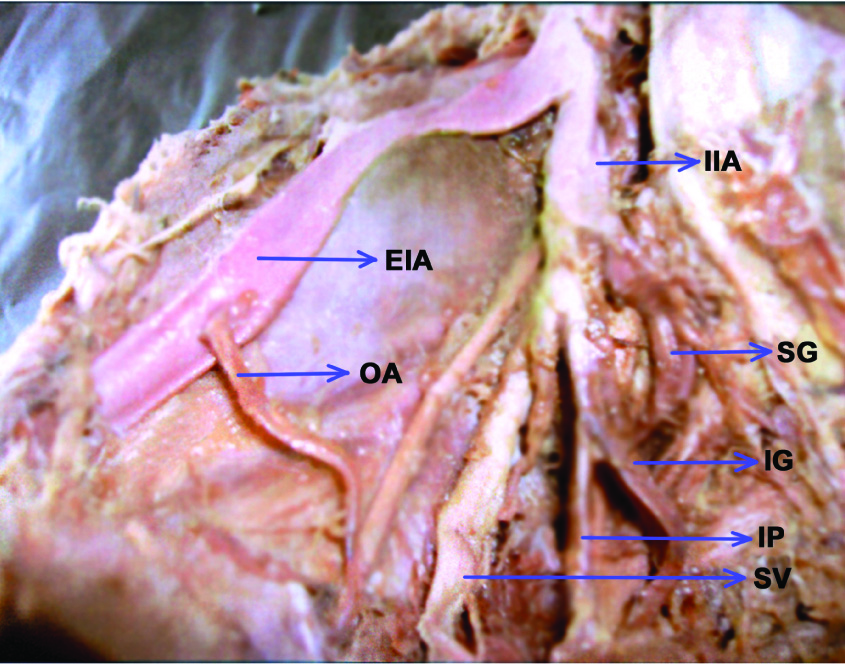
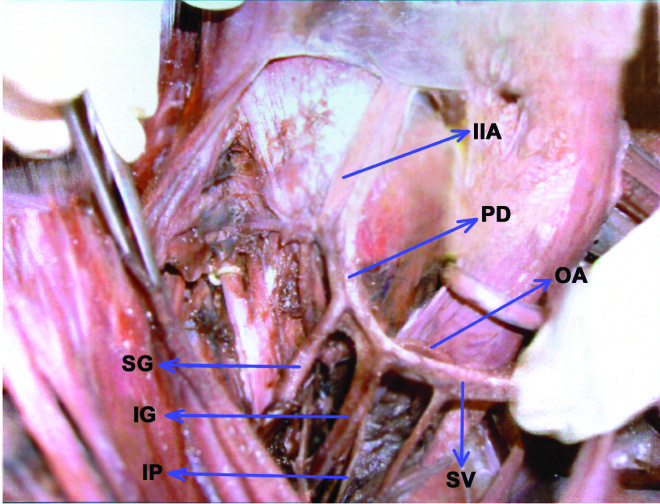
Out of 50 unilateral pelvises studied, 23 pelvic halves (46%) showed variations. In 11 (22%) cases, the origin of the OA was from the inferior epigastric artery. In 2 (4%) cases each, the origin of the obturator was from either the common stem of interal iliac artery or the external iliac artery. In 5 specimens (10%), the OA had its origin from the posterior trunk of the internal iliac artery. In another 3 specimens, the OA was seen arising from superior gluteal, inferior gluteal, and internal pudendal arteries. The present study was conducted on 50 random hemipelvises available in the Department of Anatomy. Therefore bilateral symmetry could not be assessed and the laterality of the pelvises was not considered. The observations are depicted in [Table/Fig-1,2,3,4,5,6,7 and 8].
Showing the origin of obturator artery from the inferior epigastric artery
Showing origin of obtutator artery from the common stem of internal iliac artery
Showing the origin of obturator artery from the external iliac artery
Showing origin of obturator artery from the posterior division
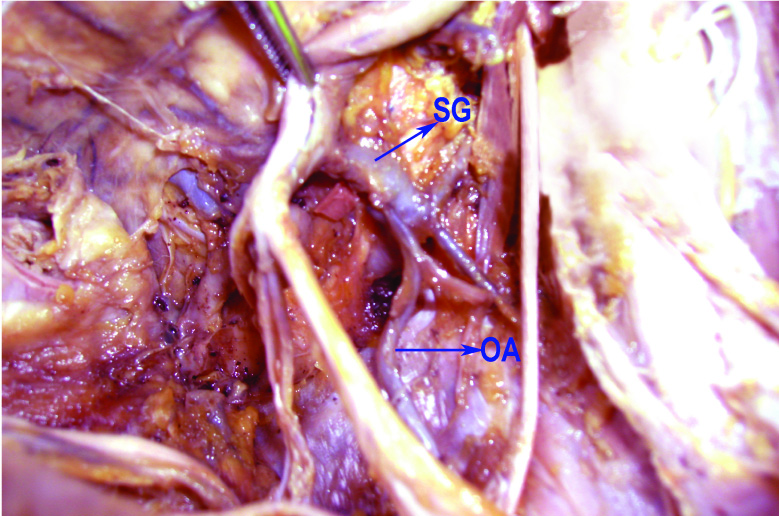
Showing the origin of obturator artery from superior gluteal
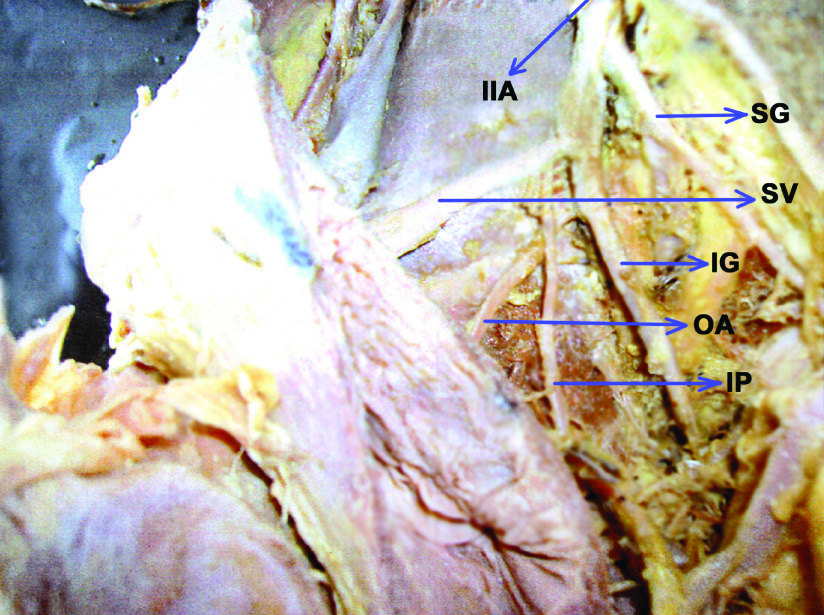
Showing the origin of obturator artery from the inferior gluteal
Showing the origin of obturator artery from the internal pudendal artery

Shows origin of obturator artery as observed in the present study
| Origin of obturator artery | Left | Right | Total | Percentage |
|---|
| Common trunk of the internal iliac artery | 2 | 0 | 2 | 4 |
| External iliac artery | 1 | 1 | 2 | 4 |
| Inferior epigastric artery | 8 | 3 | 11 | 22 |
| Posterior division of internal iliac artery | 3 | 2 | 5 | 10 |
| Superior gluteal | 1 | 0 | 1 | 2 |
| Anterior division of internal iliac artery (normal) | 10 | 17 | 27 | 54 |
| Inferior gluteal | 0 | 1 | 1 | 2 |
| Internal pudendal | 1 | 0 | 1 | 2 |
| Total | 26 | 24 | 50 | 100 |
Discussion
The internal iliac arteries provide nutrition to the pelvic wall, pelvic viscera, external genitalia, the perineum, buttocks and the medial part of the thigh. Distal collateral circulation may develop through connections between the deep femoral artery and the branches of the internal iliac arteries [5]. Hence a detailed knowledge of the vascular anatomy of pelvis is important for surgical interventions in this region.
Interesting variations in the origin of OA have long since attracted the attention of anatomists and surgeons. Bergman et al., in a compendium of human anatomic variations document that the most common source of origin of the OA, i.e., 41.4% of cases, is the common iliac or anterior division of internal iliac, in 25% the inferior epigastric, in 10% the superior gluteal, in 10% the interior gluteal/internal pudendal trunk, in 4.7% the inferior gluteal, in 3.8% the internal pudendal and in 1.1% the external iliac artery respectively [7].
Among 50 specimens observed in this study, in 54% cases, the obturator artery arose from the anterior division. Braithwaite [8]. had dissected 167 specimens and noticed that in 41% (highest) it originated from the anterior division of internal iliac artery. However, he could not find even a single OA originating from the posterior division. Kumar and Rath [9] dissected 316 pelvises and reported a case in which the left OA was found to arise from the posterior division of the internal iliac artery. In the present study, in 5 specimens, the obturator artery was seen arising from the posterior trunk. The parietal branches of the OA are important collaterals in aorto-iliac and femoral arterial occlusive diseases. In cases of ischaemic necrosis of head of femur following decreased blood flow through OA, a possible bypass graft may be considered to connect the posterior division to the distal end of the obstruction [9]. The longer OA, due to its origin from the posterior division of the internal iliac, may present an additional advantage while grafting [10].
In this study, among the variations observed, in the maximum number of cases (22%), the origin of the OA was from the inferior epigastric artery. This is in agreement with the study done by Pick et al., [10]. Pick et al., had dissected 640 cadavers and found that in 27% cases, the OA arose from the inferior epigastric artery, and 3% from the posterior division of the internal iliac artery. Four percent of cases in our study showed the origin of obturator artery from external iliac artery. Though the incidence is very low compared to the other variations, it has been reported by other workers as well; 21% by Pai et al., [7], 1.3% by Jakuhowicz and Czerniawska-Grzesinska [11], etc. If the anterior division of internal iliac artery is obstructed due to any cause, the OA and its branches will be spared, especially the branch to the head of femur, when the OA arises from the external iliac artery [9].
The ‘corona mortis’ located behind the superior pubic ramus is an anatomical variant where there is an anastomosis between the obturator and the external iliac or inferior epigastric arteries or veins [12]. ‘Corona mortis’ meaning crown of death, is so named due to its immense importance for its potential in causing considerable haemorrhage when cut and the difficulty in achieving subsequent haemostasis [12]. Darmanis et al., could find a vascular anastomosis in 83% of the cases in their cadaveric dissection study [12]. A study on 204 northeastern Thai cadavers by Namking et al., [13], reported the presence of arteria corona mortis in 22.5%, venous corona mortis in 70.6% and both structures in 17.2%. In the present study, in 26% of the cases there was a vascular connection between OA and inferior epigastric (22%) and between OA and external iliac (4%) arteries. The corona mortis or (CMOR) has widespread clinical implications being closely related to the superior pubic ramus, the acetabulum and the femoral ring and thus the femoral hernial sac that might enter the ring [14]. CMOR is at risk in groin or pelvic surgeries [15], could be avulsed in the fractures of superior pubic ramus leading to significant haemorrhage [16], could be injured in laproscopic hernia repair while dissecting the preperitoneal space of Bogros and the hernial sac [17] could prove to be a be a hazard for orthopaedic surgeons planning an anterior approach to the acetabulum such as ilioinguinal or intrapelvic [12].
Other variations that were noted in this series included one in which the OA was seen arising from the stem of the internal iliac artery (2 cases), and one each from inferior gluteal, superior gluteal and internal pudendal arteries. Biswas et al., in a study on 56 pelvic halves noted the origin of OA from the inferior epigastric in 23.3% of the cases [18], similar to our study, but could not find OA taking origin from inferior gluteal, internal pudendal, their common stem, or from iliolumbar artery. Variability in the origin of OA as reported by various authors and the findings of the present study are summarised in [Table/Fig-9] which is modified from Tiropathirao et al., [19].
Showing frequency in the origin of obturator artery reported by various authors and the findings of the present study
| Origin of Obturator Artery | Frequencies Reported by Different Workers In % |
|---|
| Persons and keith 1897 | Pick Ashely & Anson 1942 | Braithwaite 1952 | Tirupathirao et al., 2013 | Present Study 2015 |
|---|
| Direct from anterior division | 39.3 | 42.6 | 41.4 | 35.55 | 54 |
| Inferior gluteal and internal pudendal trunk | 8.2 | 10.1 | 10 | 13.33 | - |
| Inferior gluteal | 3.2 | 5.5 | 4.7 | 4.44 | 2 |
| Internal pudendal | 3.2 | 3.7 | 3.8 | 4.44 | 2 |
| Superior gluteal | 8 | 6.4 | 10 | 4.44 | 2 |
| Iliolumbar | 4.9 | 1.8 | 3.5 | 2.22 | - |
| Inferior epigastric | 25 | 21.3 | 19.5 | 26.66 | 22 |
| Direct form external iliac | 1.6 | 0.9 | 1.1 | 8.88 | 4 |
| By double origin | - | - | 6.5 | - | - |
The embryological explanations for the anomalies in the arterial patterns of the limbs are based on an unusual selection of channels from a primary capillary plexus, wherein the most appropriate channels enlarge, while others retract and disappear, thereby establishing the final arterial pattern [20,21]. The OA arises comparatively late in development as a supply to plexus, which in turn is joined by the axial artery of the lower limb that accompanies the sciatic nerve [22]. The origin of OA from the posterior division of the internal iliac artery is due to the persistence of vascular channels in relation to the posterior division that might have given rise to the OA, while the vascular channels related to the anterior division of the internal iliac artery destined to be the obturator artery have disappeared [9]. Before the OA appears as an independent blood vessel from the rete pelvicum, the blood flow destined for this territory makes an unusual choice of source channels. Instead of arising from the internal iliac artery as usual, it arises from the inferior epigastric artery, or directly from the external iliac artery.
Conclusion
The present study revealed that the origin of the obturator artery is highly variable, 23 out of 50 pelvic halves having variable origin of OA. Surgeons operating on the pelvic region should have a thorough knowledge of the pelvic vasculature, particularly pertaining to the OA, due to its wide distribution and highly variable origin, as such aberrant origins may be a significant source of bleeding during surgical interventions in the region. Awareness of variations in the vascular anatomy of abdomen and pelvis is also essential due to rapid development of surgical and investigatory techniques in obstetric maneouvres and urogenital interventions.
Abbreviations
OA- Obturator artery
SG- Superior gluteal
IG- Inferior gluteal
IP- Internal pudendal
SV- Superior vesical
INF EPI- Inferior epigastric
E IA- External iliac
AD- Anterior division
PD- Posterior division
OF- Obturator foramen
IIA- Internal illiac artery