The phylogenic, ontogenic and racial variations of the scapula, make it as one of the most interesting bones for research [1]. Moreover, the meticulous dimensions of the scapula are of major importance in the patho-mechanics of rotator cuff disease, total shoulder arthroplasty, and recurrent shoulder dislocation [2].
The acromion is related to a variety of disorders and contributes to pathologic conditions in the shoulder [3]. Moreover, its morphology is an important tool in shoulder pathology diagnosis [4]. The predominant theory for the impingement syndrome of the rotator cuff muscles classifies the causative agents as anatomical and functional. The anatomical causes include the shape and inclination of the acromion process [5]. This theory was supported by other studies [6,7] that showed a high incidence of rotator cuff disease with type III acromia. Therefore, morphometry of the acromion is important as its anatomical variation may contribute to shoulder pathologies, [8]. However, few studies had been carried out to record various shapes and variants of the scapula [3].
Based on the presence of a notch on the anterior glenoid rim, the shapes of the glenoid cavity have been classified into: pear shaped, inverted-comma shaped or oval shaped [9]. Moreover, the inclination of the glenoid has been associated with full thickness rotator cuff tears [10]. Therefore, variations of shape and size of glenoid cavity of scapula is important for the understanding of shoulder dislocation, rotator cuff disease and to determine the meticulous size of the glenoid component in the shoulder arthroplasty and has a prognostic value on the primary gleno-humeral osteoarthritis [11].
The purpose of the current study was to record the morphometrical data for the acromion and the glenoid cavity of the scapula specifically and to study the various shapes of both the acromion process and the glenoid cavity in the Egyptian population and to compare the data obtained from the present study with those of other populations in order to establish possible morphofunctional correlations related to race, geographic region and literature data. Moreover, these data could have clinical role for better understanding and management of shoulder pathology; gleno-humeral instability, orthopaedic joint replacement and rotator cuff tears management in Egyptians.
Materials and Methods
A total of 160 completely ossified, dry, unbroken scapulae were collected from Department of Human Anatomy and Embryology, Faculty of Medicine, Suez Canal University, Ismailia, Egypt in the current study. The bones belonged to mature specimens, but the exact ages or genders were not known. Of the 160 scapulae, 80 belonged to the right side, and 80 belonged to the left one. Only bones with clear and intact features were used for the study while damaged scapulae were excluded.
Each scapula underwent a morphological evaluation and osteometric measurements for whole scapula, acromion and glenoid cavity.
The linear measurements were taken using a sliding vernier calliper (accurate to 0.1 mm) and recorded in millimetres. The measurement of the thickness of the acromion was made by a specially scaled 1 mm gauge, where this could not be achieved with a micrometer. The angular measurements were made with a goniometer.
Morphological Evaluation
– Morphological shapes of the tip of the acromion were recorded as: cobra-shaped, square tip and intermediate-shaped [5] [Table/Fig-1].
– Types of inferior surface of acromion process according to appearance: rough and smooth types.
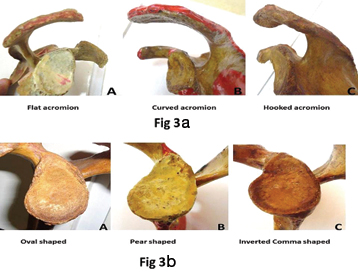
– Types of acromion process according to slope: The angle of slope is formed by the intersection of a line extending from the tip of the hook to the junction of the hook (A) and a line along the undersurface of the acromion (B) [12] [Table/Fig-2]. When angle ranged from 0° to 12°, acromion was considered type I or flat, from 13° to 27°, acromion was considered type II or curved. Angles above 27° classified acromion as type III or hooked [5] [Table/Fig-3a].
– Morphological shapes of the glenoid cavity: was recorded in the following way [13]. A piece of white sheet was placed on the glenoid cavity and held firmly in position to trace the shape of the glenoid cavity. The side of the point of a lead pencil was rubbed along the rim of the glenoid cavity to get a tracing of the shape of the glenoid cavity on the paper. It was scored as being: oval, pear shaped or inverted comma shaped [14] [Table/Fig-3b].
Morphological shapes of the tip of the acromion

Measure of acromion angle (arrow). A corresponds to a line extending from the tip of the hook to the junction of the hook and B corresponds to a line along the undersurface of the acromion

(a) Classification of the acromial morphology; (b) Morphological types of the glenoid cavity
Osteometric Evaluation
(A) The scapular parameters [15]
– Maximum length: is the maximum longitudinal diameter between the superomedial and inferior angles [Table/Fig-4a].
– Maximum width: is the maximum transverse diameter between the medial border of the scapula, where the spine meets the body of the scapula and the anterior lip of the glenoid [Table/Fig-4a].
(a) Scapular parameters: L represents maximum longitudinal diameter and W represents maximum width; (b) Acromion parameters."L" represents the maximum length. "B"representsthe maximum breadth and "T" represents the thickness; (c) Acromio-coracoid (A) and acromio-glenoid (B) distances
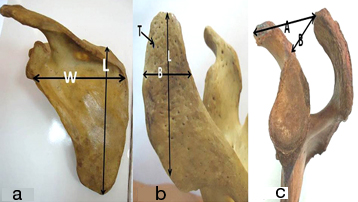
(B) The acromion parameters [5]
– Maximum length: is the distance between tip and midpoint of posterior border of acromion process [Table/Fig-4b].
– Maximum breadth: is the distance between the lateral and medial borders at the midpoint of the acromion process [Table/Fig-4b].
– Thickness: is 1 cm behind the anterior border and 1 cm medial to the lateral border [Table/Fig-4b].
– The acromio-coracoid distance: is the distance between both tips of acromion and coracoid processes [Table/Fig-4c].
– The acromio-glenoidal distance: is the distance between tip of acromion process and supraglenoid tubercle [Table/Fig-4c].
(C) The glenoid cavity parameters [13] [Table/Fig-5]
Diameters of the glenoid cavity. A: Superior-Inferior, B: Anterior-Posterior 1, C: Anterior-Posterior 2

– Superior-Inferior glenoid diameter: is the maximum distance between the inferior point of the glenoid border and the most prominent point of the supraglenoid tubercle [Table/Fig-5].
– Anterior-Posterior glenoid diameter 1: is the maximum breadth of the articular margin of the glenoid cavity perpendicular to the glenoid cavity height [Table/Fig-5].
– Anterior-Posterior glenoid diameter 2: Is the anterior-posterior diameter of the superior half of the glenoid cavity at its mid-point [Table/Fig-5].
Statistical Analysis
Each one of these measurements and observations were performed by only one investigator to reduce inter-observer error, three times separately and tabulating the mean value measurement. The mean ± SEM of the measurements were calculated. The data were analysed using the Statistical Package for the Social Sciences (SPSS) version 15.0. The morphometric values of the two sides were analysed using an unpaired t-test. Statistical significance was set p≤ 0.05. For comparison of the data obtained from the present study with earlier published reports, one sample t-test was employed.
Results
Regarding the morphological shape of the tip of the acromion, the intermediate shape presented with the highest incidence. The cobra shaped presented with the lowest distribution in both sides. The intermediate shape of the tip of the acromion was also presented with the medium frequency distribution among the total scapulae [Table/Fig-6&7a].
The incidence of the morphological parameters
| Parameter | Right side | Left side | Total mean |
|---|
| No | % | No | % | No | % |
|---|
| Morphological shapes of the tip of the acromion |
| Cobra shaped | 13 | 16.25 | 11 | 13.75 | 24.00 | 15.00 |
| Square tip | 24 | 30.00 | 27 | 33.75 | 51.00 | 31.88 |
| intermediate | 43 | 53.75 | 42 | 52.50 | 85.00 | 53.12 |
| Types of the inferior surface of the acromion process |
| Smooth | 69 | 86.25 | 70 | 87.50 | 139 | 86.88 |
| Rough | 11 | 13.75 | 10 | 12.50 | 21 | 13.12 |
| Types of the acromion process according to slope |
| Flat | 20 | 25.00 | 23 | 28.75 | 43 | 26.88 |
| Curved | 49 | 61.25 | 44 | 55.00 | 93 | 45.62 |
| Hooked | 11 | 13.75 | 13 | 16.25 | 24 | 15.00 |
| Shapes of the glenoid cavity |
| Oval shaped | 39 | 48.75 | 42 | 52.50 | 81 | 50.63 |
| Pear shaped | 28 | 35.00 | 22 | 27.50 | 50 | 31.25 |
| Inverted comma shaped | 13 | 16.25 | 16 | 20.00 | 29 | 18.12 |
(a) Percentage of the morphological shapes of the tip of the acromion; (b) Percentage of the types of the inferior surface of the acromion process; (c) Percentage of the types of the acromion process according to slope; (d) Percentage of the shapes of the glenoid cavity

Types of the acromion according to its slope were also examined. In both sides, type II curved presented the highest incidence, while type III hooked acromion presented the lowest incidence [Table/Fig-6&7b].
In both sides, the smooth inferior surface of the acromion was found to be more commonly distributed than the rough one; and predominantly linked to type III acromia [Table/Fig-6&7c].
The oval shaped glenoid cavity presented with the highest incidence among the total scapulae examined while the inverted coma shaped showed the lowest incidence [Table/Fig-7d]. The scapular, acromion and glenoid diameters are presented in [Table/Fig-8,9 and 10].
Mean values of the scapular parameters
| Parameter | Right side | Left side | Total mean |
|---|
| Mean ± SD | Mean ± SD | Mean ± SD |
|---|
| Maximum length(mm) | 151.05±8.42 | 151.20±9.47 | 151.16±10.32 |
| Maximum width (mm) | 107.43±8.07 | 107.01±9.00 | 107.22±9.74 |
| Width / length index (%) | 71.12 | 70.77 | 70.93 |
Mean values of the acromion parameters
| Parameter | Right side | Left side | Total mean |
|---|
| Mean ± SD | Mean ± SD | Mean ± SD |
|---|
| Maximum length | 52.33±4.19 | 53.28±4.11 | 52.81±4.08 |
| Maximum breadth | 32.09±3.21 | 32.01±3.69 | 32.05±3.88 |
| Thickness | 9.11±2.74 | 8.92±2.35 | 9.06±2.68 |
| The acromio-coracoid distance | 31.10±3.55 | 31.58±3.09 | 31.34±3.64 |
| The acromio-glenoidal distance | 27.11±3.08 | 27.67±3.00 | 27.39±3.01 |
Mean values of the glenoid parameters
| Parameter | Right side | Left side | Total mean |
|---|
| Mean ± SD | Mean ± SD | Mean ± SD |
|---|
| Superior-inferior glenoid diameter | 38.88±2.63 | 39.01±2.49 | 38.95±2.73 |
| Anterior-posterior glenoid diameter 1 | 21.33±2.49 | 21.69±2.06 | 21.51±2.69 |
| Anterior-posterior glenoid diameter 2 | 28.31±2.38 | 27.99±2.55 | 28.15±2.58 |
Discussion
In the current study, the mean value of scapular length is near to the value reported in Greeks [3]. On the other hand, the mean of the scapular height is higher than what has been reported in Indians (145.1 mm) [16] and in Turkish (98.8 mm) [8,15]. The mean value of scapular width here is nearer to what has been reported in Indians [16] but higher than reported in other populations [15]. Population, ethnic and genetic variation may play a role in these variations.
In the current study Type II acromion had the greatest incidence. Moreover, rough inferior surface of the acromion was noticed to be predominant in type III acromia. These data are in accordance to a great number of studies in other population samples which showed type II as the most frequent type [3,5,7,8,12,17–19]. However, few other studies have shown a higher frequency of the type III [20] or type I acromion [21].
We found type I as the second highest acromion type in our study, which is in accordance to several studies [3,18,20]. However, some other studies have shown that type III acromion was the second most frequent [5,8,12,17,19].
It has been explained that different acromial shapes is likely to develop due to both genetic and acquired causes; and only age is the acquired cause that has been positively correlated with progression from flat to curved or hooked acromia [6].
Moreover, these differences could be due to distinct ethnic origin in demographic samples that have their own anatomical variations [22]. Also, different methodological approaches or techniques among studies could lead to variations in classifications and analysis.
The occurrence of impingement syndrome, is more frequent with advanced age, especially having III acromion, because they are more subjected to degenerative changes [7,18]. The rotator cuff compression was seen mostly in hooked types, often seen in curved types and rarely seen in flat types of acromia [17]. In hooked acromia, the reduced dimensions of the subacromial space can lead to impingement of the rotator cuff tendon and subsequent tear production [3]. Additionally, the acromial shape has been shown to have correlation not only with the severity of symptoms in impingement syndrome but also with the outcome of the conservative therapy or the need for surgical interference [23].
Length of the acromion in the current study was found to be higher than other studies [24]. However, in Chilean population group the length of acromian has been reported higher in comparison with current study. [17] Also, in Nepalese population the acromian process length of right scapulae were more that left scapulae [25]. Ethnic differences could be the underlying reason for such morphometrical variations.
In our study, the mean breadth of the acromion process was higher than reported in other studies [17,25]. Moreover, the right acromion process was found to be wider than the left which was in match to what was reported in another study [25].
The current thickness of the acromion is different than those reported in Greeks and Indians [3,16]. These different values could be due to population variation.
The values regarding the acromio-coracoid distance in Indians and Nepalese [16,25] are higher than the current ones while the mean values of the acromio-glenoid distance are rather near to the current findings. However, our current values regarding both acromio-coracoid and acromio-glenoid distances are higher than those reported by Sitha et al., [15]. The acromio-coracoid and acromio-glenoid distances between both sides in this present study showed no significance difference, which are in match with other findings [16,25].
The distance between its tip and the upper edge of the glenoid cavity is an important factor to measure as it could influence the acromial length; which is an important factor in the diagnosis of the impingement syndrome [24].
The current values of the superior-inferior diameter of glenoid are higher than those reported by others [8,11,13,26]. They also mentioned that the right glenoid value was slightly higher than the left which is contradictory to what is found in the current study [11,13].
The mean anterior-posterior diameter 2 of the glenoid in the current study is higher than other studies [11,13,15,27]. On the other hand, the AP-2 diameter recorded in the current study was near to [26]. The Anterior-Posterior diameter 1 in the current study was near to values reported for East Anabolia [27] but lower than reported for other populations [11,13].
The current findings indicate the most frequently glenoid type is the oval shaped one while the least one is the inverted coma shaped. These results are in match with others [8,9]. However, the current results are contradictory to other reports [9,11,13].
Racial and sexual differences can interfere in the development of bone projections, providing alterations such as size and morphology. These alterations can occur in scapulae and may affect the glenohumeral stability. When the glenoid notch is distinct, the glenoid labrum is often not attached to the rim of the glenoid at the site of the notch and can be a predisposing factor in anterior dislocation of the shoulder joint [9].
Conclusion
Variations in the size and shape of the acromion process and glenoid cavity which were observed in the current study will be of great help for orthopaedic surgeons to understand the shoulder pathology better and to decide the proper size of the glenoid component for the shoulder arthroplasty in Egyptians.