Pattern of Cancers Treated with Radiotherapy in Uduth Sokoto: A New Center Experience
Usman M. Aliyu1, Abdulgafar O. Jimoh2, Abdulmajeed Yunusa3, Moh’d Umar4
1 Head of Department/Consultant Clinical, Departments of Radiotherapy and Oncology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria.
2 Lecturer/Faculty Examinations Officer, Department of Pharmacology and Therapeutics, College of Health Sciences, Usmanu Danfodiyo University, Sokoto, Nigeria.
3 Lecturer, Department of Pharmacology and Therapeutics, College of Health Sciences, Usmanu Danfodiyo University, Sokoto, Nigeria.
4 Lecturer/Consultant Histopathologist, Department of Morbid Anatomy & Forensic Medicine, College of Health Sciences, Usmanu Danfodiyo University, Sokoto, Nigeria.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abdulgafar O. Jimoh, Lecturer/Faculty Examinations Officer, Department of Pharmacology and Therapeutics, College of Health Sciences, Usmanu Danfodiyo University, Sokoto, Nigeria.
E-mail: layidotcom@yahoo.com
Background
Cancer is a leading public health problem worldwide. In many developing countries, cancer tends to present in predominantly advanced stages, to a certain extent due to lack of comprehensive screening and poor access to efficient management. This study was carried out to describe the pattern of cancers managed in the Department of Radiotherapy and Oncology in Usmanu Danfodiyo University Teaching Hospital Sokoto, North-western Nigeria.
Materials and Methods
This was a cross-sectional descriptive study involving patients with malignancies that attended the new Oncology Department of the Usman Danfodiyo University Teaching Hospital Sokoto, North-West Nigeria for the period of one year (June 2013 – May 2014). The data was analyzed using SPSS (versions 20).
Result
A total of 210 patients with complete records met the criteria for the study. Majority 162 (77.1%) were females with a mean age of 45.68±12.4 years. The male patients were 48 (22.9%) with mean age 46.27±16.5. The spectrum of malignant lesions observed were cancer of the cervix 77 (36.67%), breast cancer 74 (35.24%), nasopharyngeal cancer 20 (9.52%), cancer of the larynx 18 (8.57%) and rectal cancer 14 (6.67%). Late presentation was most common with 6 (3%), 101 (49.8%) and 58 (28.6%) patients presenting at stage I, III and IV, respectively.
Conclusion
The study demonstrates that Cancer of the cervix is the leading malignancy in the study population.
Late presentation, Oncology, Sokoto nigeria
Introduction
Cancer is a major public health problem worldwide [1]. In 2005, cancer comprised 13% of all deaths worldwide [2]. According to the projection by [3], 15.4 million new cancer cases will be diagnosed and 9.8 million of them will die of the disease. In many developing countries, cancer tends to present in predominantly advanced stages, partly because of lack of comprehensive screening and poor access to effective treatment [4]. The age-adjusted survival for breast cancer and cervical cancer is estimated overall to be 57% and 41% in developing countries respectively, compared with 73% and 61% in developed countries [3]. By 2020, 61% of all incident cancer cases are projected to be in developing countries [5]. Radiotherapy refers to the use of ionising radiation in the treatment of malignant and some benign conditions. It’s now the most important non-surgical cancer therapy used in more than 50% of all patient with cancer weather curative or palliative [6]. Previous Studies conducted in Nigeria showed high prevalence of breast, cervical and prostate cancers [7–10]. In Uganda, cervical cancer followed by breast cancer in females, and penis followed by prostate cancers in males is the pattern [11]. In the globe, the most common malignancies in females in descending order are breast, lung, colorectal, endometrial and thyroid cancer respectively. In males, prostate, lung and colorectal cancer in decreasing order is the case [1]. Cancers that were initially thought to be rare in the country are becoming more frequent. Knowing the cancer type and pattern of presentation helps in planning and implementing appropriate measures in terms of prevention, early diagnosis and treatment and limitation of disability to reduce morbidity and mortality associated with the disease. This study is thus aimed at describing the pattern of cancers treated with radiotherapy in Sokoto, north-western Nigeria.
Materials and Methods
The study was a retrospective cross-sectional descriptive study of cancer patient seen and treated with radiotherapy in the Department of Radiotherapy and Oncology, Usmanu Danfodiyo University Teaching Hospital Sokoto, Nigeria. This center serves as a referral center for all the neighbouring states which includes; Kano, Katsina, Zamfara, Kebbi, Kaduna, Niger, Kwara states. The department of radiotherapy and oncology was brought into being in year 2007 under vamed project. The centre is equipped with a multi-modal linear accelerator with two photons energy (6mv and 15mv) and five electron energy capabilities, a CT-Simulator (CT-Sim), a computerised treatment planning system (TPS) and a fully functional mould room. All available radiotherapy case notes and treatment records of cancer patients attended to at the department of Radiotherapy and Oncology from June 2013 to May 2014 were retrieved from hospital’s record department.
Statistical Analysis
Data was extracted into a microsoft excel spreadsheet, including patients demographic data, diagnosis, cancer types, and stage at presentation. Attention was paid to patient’s biodata and diagnosis. Stage at presentation and cancer type were all taken from the case notes. The data was analysed using statistical package software for social sciences (SPSS, version 20)
Results
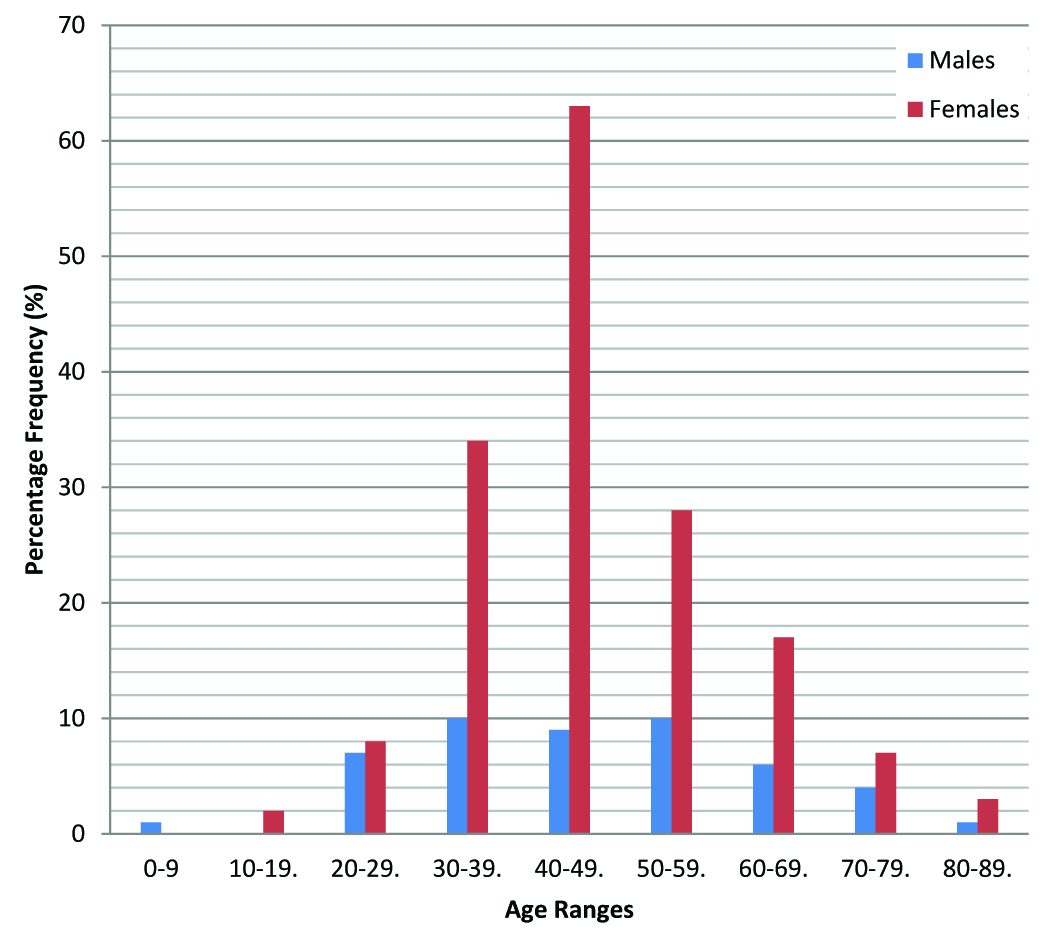
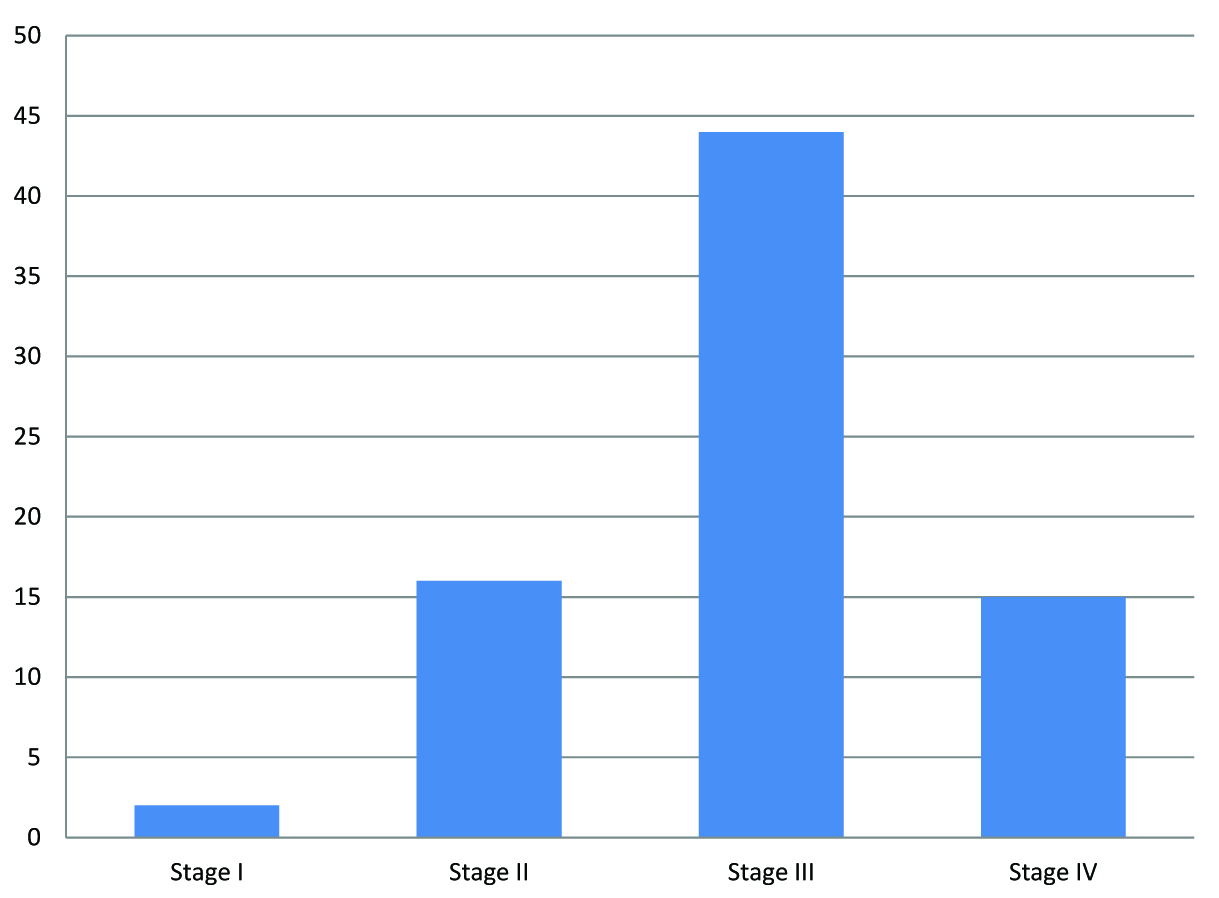
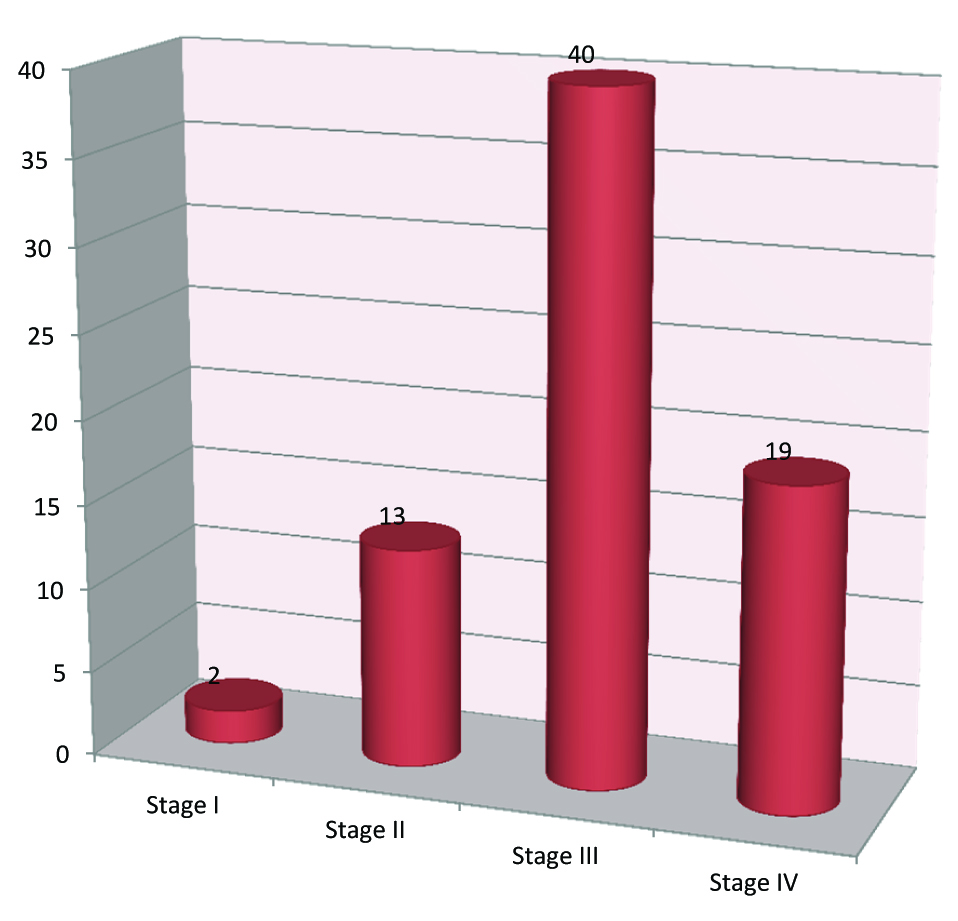
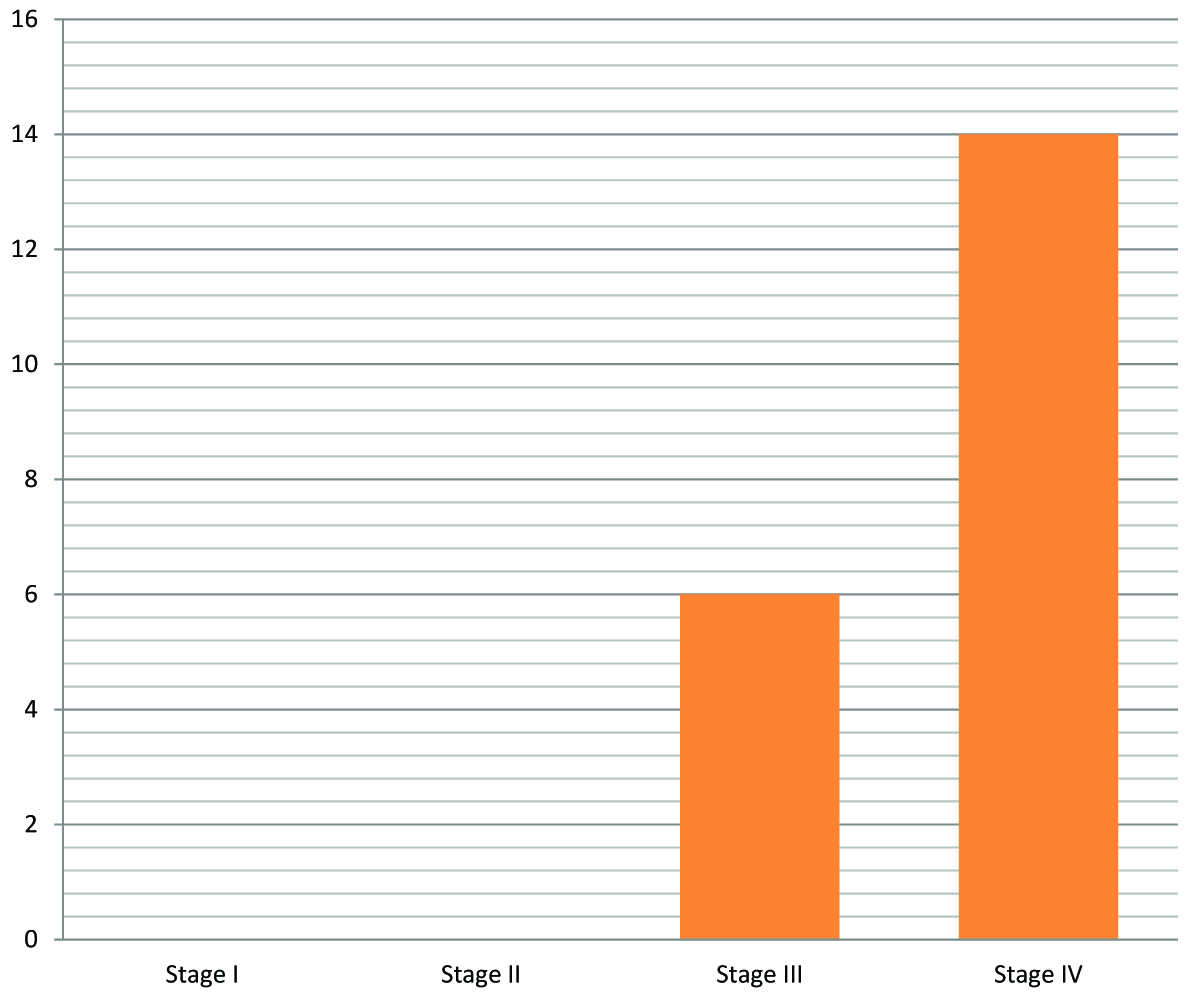
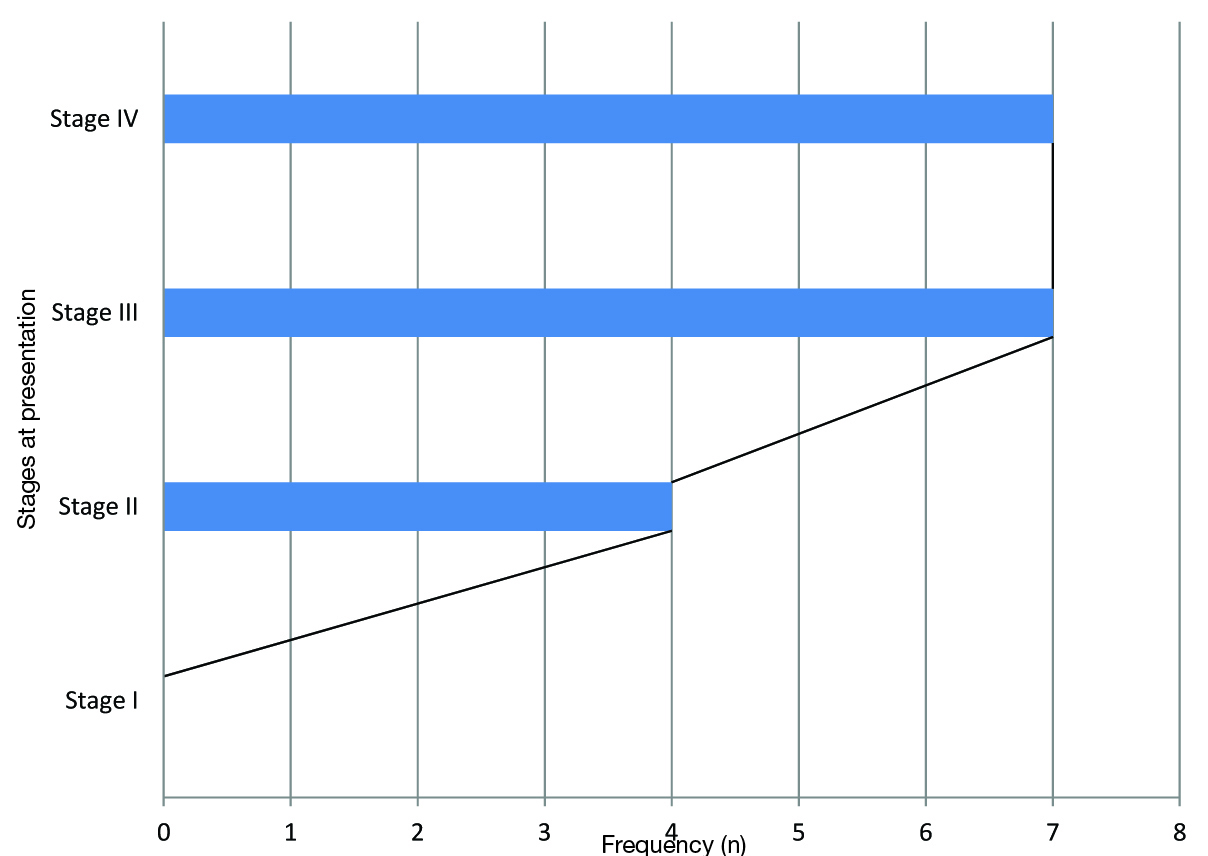
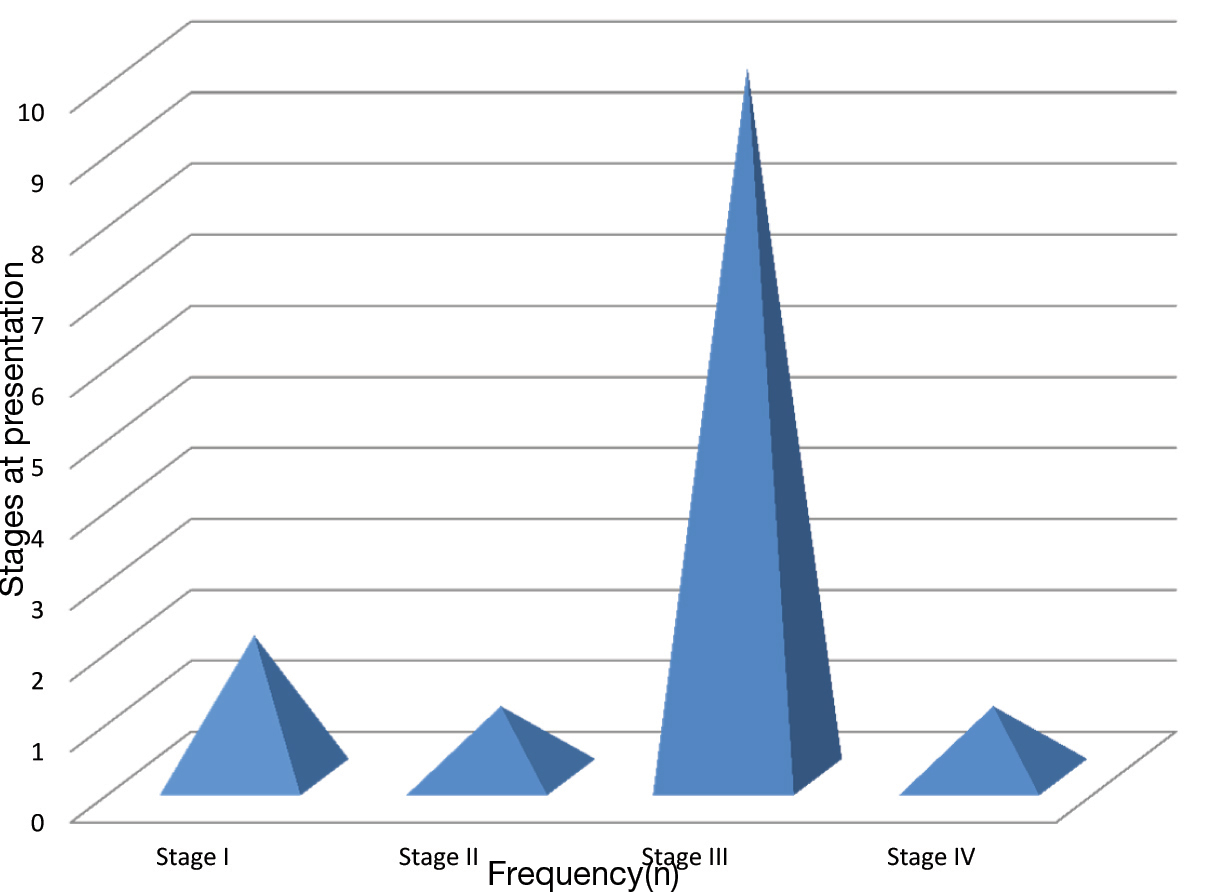
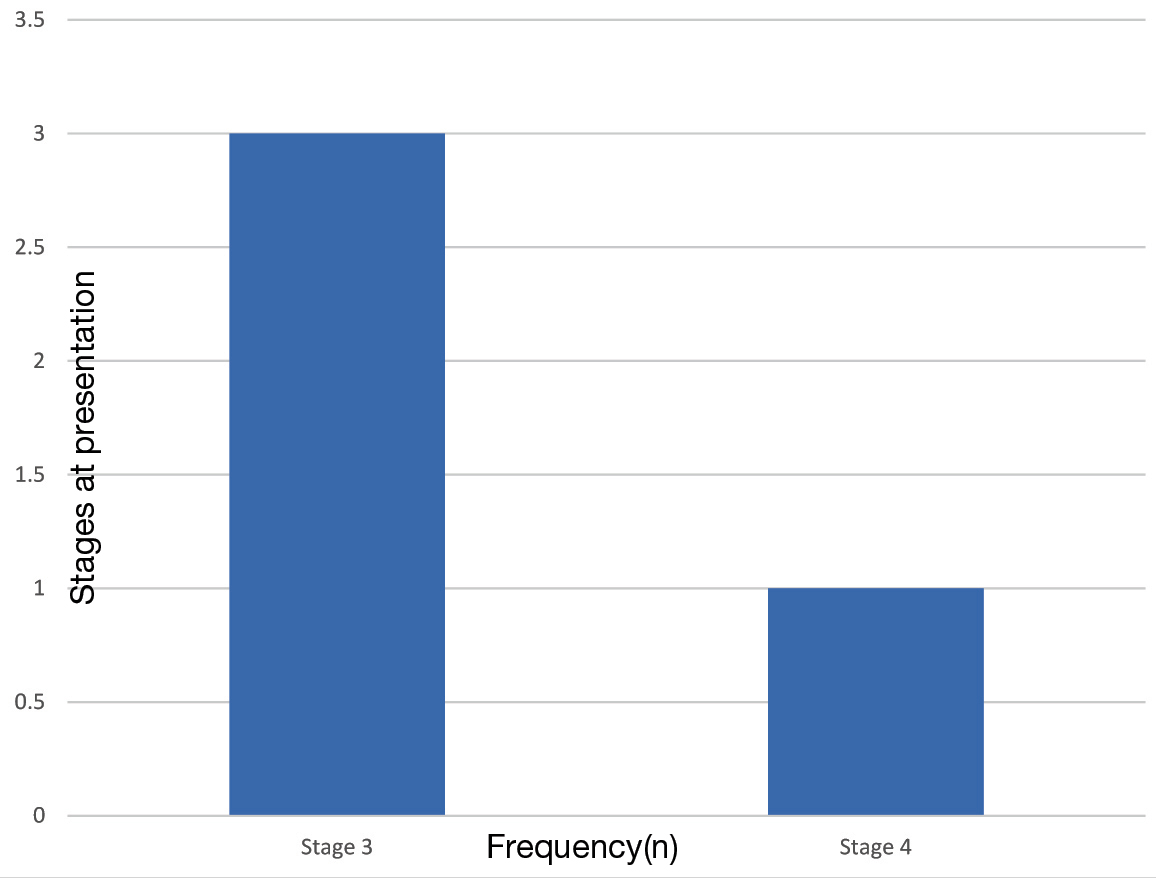
Two hundred and ten cases were seen in the department within the study period. The majority 162 (77.1%) were females with a mean age of 45.681±12.4 years. The male patients were 48 (22.9%) with a mean age of 46.271±6.5 and male to female ratio were approximately 3:1. The age range of the patients was between 5 to 85 years with a mean age of 45.81±13.44 [Table/Fig-1]. Cervical cancer was seen in 77 (36.67%) of the patients, of which two (2.60%) presented at stage I, 16 (20.78%) at stage II, 44 (57.14%) at stage III and 15 (19.48%) at stage IV [Table/Fig-2,3]. Seventy-four (35.24%) of the study population had breast cancer. Two (2.7%), 13 (17.57%), 40 (54.05%) and 19 (25.68%) breast cancer patients presented at stages I, II, III and IV respectively [Table/Fig-2,4]. Twenty (9.52%) had nasopharyngeal cancer with the highest percentage (14, 70.0%) presenting at stage IV while six (30.0%) presented at stage III [Table/Fig-2,5]. Four (22.22%), 7 (38.89%) and 7 (38.89%) of the laryngeal cancers presented at stages II, III and IV respectively [Table/Fig-6]. The majority (10, 71.43%) of the 14 patients with rectal cancer presented at stage III. Out of the 3 (1.43%) patients with oropharyngeal cancer, 66.67% came at the late stage [Table/Fig-7]. Anal cancer recorded only stages 3 and 4 [Table/Fig-8].
Cancer types and frequencies
| Cancer Type | Frequency | Percentage (%) |
|---|
| Cervix | 77 | 36.67 |
| Breast | 74 | 35.24 |
| Nasopharynx | 20 | 9.52 |
| Oropharynx | 3 | 1.43 |
| Larynx | 18 | 8.57 |
| Rectal | 14 | 6.67 |
| Anal | 4 | 1.90 |
| TOTAL | 210 | 100 |
Distribution of Cervical cancer according to stages at time of presentation
Distribution of Breast Cancer according to stages at time of presentation
Distribution of Nasopharyngeal cancer according to stages at time of presentation
Distribution of cancer of the Larynx according to stages at time of Presentation
Distribution of Rectal cancer according to stages at time of presentation
Distribution of Anal cancer according to stages at time of presentation
Discussion
Cancer is a major public health problem worldwide [1]. Knowing the cancer type and pattern of presentation helps in planning and implementing appropriate measures in terms of prevention, early diagnosis and treatment and limitation of disability. This will in turn reduce morbidity and mortality associated with the disease. This study was aimed at finding the distribution pattern of cancers treated with radiotherapy in Sokoto, north-western Nigeria.
The study showed that more female were affected with cancers. Similar studies reported female population to be more affected by the disease [8,12]. Contrarily, men were also reported to be more affected by the disease [13]. Most of the cases seen were within the age range 40 to 49 with mean ages of 46.27 and 45.68 years for male and female respectively. Previous work showed similar mean ages [7,10]. Higher mean ages of 61.8 And 56.8 years for males and females respectively have also been reported [12]. Another study reported that cancer is commoner in elderly especially in those greater than 65 years [14]. Other non cancer related studies in the centre revealed a mean age of 46.50 years [15]; with a higher percentage of female subjects [16]. The spectrum of malignant lesions observed in this study was cancer of the cervix, breast cancer, nasopharyngeal cancer, cancer of the larynx and rectal cancer, anal cancer. Cervical carcinoma was the most common followed by cancer of the breast. Similar studies in Nigeria and Uganda also reported cervical and breast cancers as the most common female cancers [9–11]. This finding is contrary to what was reported by Jedy-Agba et al., and Iseh and Malami showing breast cancer as the commonest followed by cervical cancer [17,18]. The Pattern of presentation was disturbing, as most of the patients presented in the late stages of the cancer. Several previous studies have reported late stage presentations [19–23]. Majority of cancer cases were diagnosed at advanced stages probably due to lack of effective screening and early detection services, in addition to the lack of eloquent public awareness campaign [24]. Study by Lannin et al., described socio-economic, cultural and attitude as factors that cause late-stage presentation of breast carcinoma [25]. In a study by Ajekigbe fear of mastectomy, preference for prayer houses [26], spiritual healings or native doctors were reasons responsible for late presentation of breast carcinoma, with a sizable percentage of cancer patients using one form or the other of traditional medicine [27]. Delay in seeking health care and delay in referring patients to tertiary hospitals were reasons for late presentation of cervical carcinoma [28]. Nasopharyngeal cancer was reported as the commonest head and neck cancer [18]. This finding is in agreement with the finding in this study which showed nasopharyngeal cancer as the third must common malignancy.
Although, prostatic cancers were previously reported as one of the common male cancer [1,7–11] the current study did not report any case of prostatic cancer.
Limitations of The Study
The limitations of this study include the sample size and gender distribution within the study period reflecting the situation in a local hospital but with limited implication for a general epidemiological viewpoints.
Conclusion
Age at presentation was relatively early compared to some previous studies. This is quite alarming and calls for urgent action to curtail the menace of this disease. Cancer of the cervix is the commonest malignancy observed, hence the need for advocacy and effective screening among women in the region. Majority of the patients presented late (stages III and IV), hence the need for a holistic approach in order to make early diagnosis and prompt treatment to prevent morbidity and mortality associated with the disease. Based on the findings there is an urgent need for a comprehensive and vibrant cancer registry for more research. An effective Public enlightenment campaign to inform the public on cancer with the aim of improving their knowledge, hence achieving a change in attitude toward positive health seeking behavior is strongly advocated. Setting a functional and effective early referral system from primary health care centers to a tertiary center equipped with the tools necessary for effective management. Constructing and equipping a radiotherapy and oncology center in each of the tertiary hospitals in the country. Setting a screening programme to reach out to those at risk with the aim preventing the disease from becoming advanced. Early diagnosis and multidisciplinary treatment is highly advocated to achieve cure and prevent morbidity and mortality.
[1]. Siegel R, Ma J, Zou Z, Jemal A, Cancer statisticsCA: a cancer journal for clinicians 2014 64:9-29. [Google Scholar]
[2]. World Health Organization. Preventing chronic diseases: a vital investment: WHO global report 2005 [Google Scholar]
[3]. Parkin DM, The global health burden of infection-associated cancers in the year 2002International journal of cancer 2006 118:3030-44. [Google Scholar]
[4]. John RM, Tobacco consumption patterns and its health implications in IndiaHealth policy 2005 7:213-22. [Google Scholar]
[5]. Mathers CD, Loncar D, Projections of global mortality and burden of disease from 2002 to 2030PLoS medicine 2006 3:e442 [Google Scholar]
[6]. Cohen JE, Human population: the next half centuryScience 2003 302:1172-75. [Google Scholar]
[7]. Malami SA, Pindiga UH, Abimiku BA, Mungadi IA, Abdullahi AD, Dauda A, A descriptive retrospective study of the pattern of malignant diseases in Sokoto, Northwestern Nigeria (1999–2004)J Med Sci 2007 7:1033-38. [Google Scholar]
[8]. Afolayan E, Ibrahim O, Ayilara G, Cancer Patterns In Ilorin: An Analysis Of Ilorin Cancer Registry StatisticsTropical Journal of Health Sciences 2012 19 [Google Scholar]
[9]. Dogo D, Gali B, Ali N, Nggada H, Male breast cancer in north eastern NigeriaNigerian journal of clinical practice 2007 9:139-41. [Google Scholar]
[10]. Awodele O, Adeyomoye AA, Awodele DF, Fayankinnu VB, Dolapo DC, Cancer distribution pattern in south-western NigeriaTanzania journal of health research 2011 13:106-8. [Google Scholar]
[11]. Wabinga H, Pattern of cancer in Mbarara, UgandaEast African medical journal 2002 79:193-97. [Google Scholar]
[12]. Doumi EBA, Ahmed M, Hamad A, Pattern and incidence of cancer at El Obeid Hospital, Western SudanSudan Journal of Medical Sciences 2009 4 [Google Scholar]
[13]. Ferlay J, Cancer IAFRO, GLOBOCAN 2000: cancer incidence, mortality and prevalence worldwide 2001 IARC press [Google Scholar]
[14]. Sankaranarayanan R, Ramadas K, Qiao YL, Managing the changing burden of cancer in AsiaBMC medicine 2014 12:3 [Google Scholar]
[15]. Jimoh AO, Sabir AA, Chika A, Sani Z, Pattern of antidiabetic drug use in a diabetic outpatient clinic of a tertiary health institution in Sokoto, North-western NigeriaJournal of Medical Sciences 2011 11(5):241-45. [Google Scholar]
[16]. Jimoh AO, Etuk EU, Sani Z, Hudu AS, The pattern of antibiotic use in a family medicine department of a tertiary hospital in Sokoto, North Western NigeriaJournal of Clinical and Diagnostic Research 2011 5(3):566-69. [Google Scholar]
[17]. Jedy-Agba E, Curado MP, Ogunbiyi O, Oga E, Fabowale T, Igbinoba F, Cancer incidence in Nigeria: A report from population-based cancer registriesCancer epidemiology 2012 36:e271-78. [Google Scholar]
[18]. Iseh K, Malami S, Pattern of Head and Neck Cancer in SokotoNigerian Journal of Otorhinolaryngology 2006 3:77-83. [Google Scholar]
[19]. Daniel C, Emmanuel I, Lydia R, Magaji A, Siddique M, Screening for cervical cancer: Experience from a university hospital in north western Nigeria (2007-2009)Journal of Basic and Clinical Reproductive Sciences 2013 2:18 [Google Scholar]
[20]. Agbo P, Khalid A, Oboirien M, Clinical Presentation, Prevalence and Management of Breast Cancer in Sokoto, NigeriaJ Women’s Health Care 2014 3:2167-0420.1000149. [Google Scholar]
[21]. Iseh K, Abdullahi A, Malami S, Clinical and Histological Characteristics of Nasopharyngeal Cancer in Sokoto, North Western, NigeriaWest African journal of medicine 2009 28 [Google Scholar]
[22]. Anorlu RI, Cervical cancer: the sub-Saharan African perspectiveReproductive Health Matters 2008 16:41-49. [Google Scholar]
[23]. Otieno E, Micheni J, Kimende S, Mutai K, Delayed presentation of breast cancer patientsEast African medical journal 2010 87:147-50. [Google Scholar]
[24]. Parkin D, Ferlay J, Hamdi-Cherif M, Sitas F, Thomas J, Wabinga H, Whelan S, Cancer in AfricaEpidemiology and prevention 2003 LyonIARC Press [Google Scholar]
[25]. Lannin DR, Mathews HF, Mitchell J, Swanson MS, Swanson FH, Edwards MS, Influence of socioeconomic and cultural factors on racial differences in late-stage presentation of breast cancerJama 1998 279:1801-07. [Google Scholar]
[26]. Ajekigbe A, Fear of mastectomy: the most common factor responsible for late presentation of carcinoma of the breast in NigeriaClinical Oncology 1991 3:78-80. [Google Scholar]
[27]. Jimoh AO, Bakare TA, Safety perception and knowledge of commonly used complementary and alternative medicine among physicians in Usmanu Danfodiyo University Teaching Hospital Sokoto, North-western NigeriaSahel Medical Journal 2014 17(4):140-44. [Google Scholar]
[28]. Anorlu R, Orakwue C, Oyeneyin L, Abudu O, Late presentation of patients with cervical cancer to a tertiary hospital in Lagos: what is responsible?European journal of gynaecological oncology 2003 25:729-32. [Google Scholar]