Sigmoid volvulus is considered to be one of the leading causes of acute intestinal obstruction. This could be related to sigmoid colon being a mobile loop which normally lies in the lesser pelvis, but its length and form are the most variable of all colonic segments [1]. It is usually completely invested in peritoneum and is attached to the lower posterior abdominal wall by the fan-shaped sigmoid mesocolon [2]. The position and shape of the sigmoid colon varies according to the length of the colon; the length and mobility of its mesocolon; the degree of distension; the condition of the neighbouring viscera like rectum, bladder and uterus. Studies have shown that variation in the shape of mesocolon could alter the morphology of sigmoid colon [3]. In addition, the length and diameter of the sigmoid colon was found to vary in both genders [4,5] and noted to increase with age [6]. The present study aims to find the morphology of sigmoid colon in South Indian population using cadavers in view of the high incidence of sigmoid volvulus in cases of intestinal obstruction.
Materials and Methods
Approval of the Institutional review board and ethics committee was obtained for the study. Thirty one cadavers donated to the Department of Anatomy for the purpose of teaching and research during the years 2012 to 2014 were evaluated. Cadavers with normal colons without any colonic disease were included in the study. The exclusion criteria were: 1) laparotomy incisions found on cadavers that indicated surgeries in life; 2) diseased or injured sigmoid colon; 3) intra-abdominal pathology such as peritonitis, stricture or adhesions. The age and gender of the cadavers were noted.
The sigmoid colon was classified into three main types, classical, long- narrow and long- broad types as described by Madiba and Haffajee [5]. The classical type of sigmoid colon was the one that lies close to the pelvic brim with the normal anatomical textbook description. In long-narrow type, sigmoid colon was long with the root of mesocolon being narrow, while in long-broad type, though the sigmoid colon was long, the mesocolon was broad. The position of the sigmoid colon in reference to pelvic brim was categorised into pelvic and suprapelvic positions.
The following dimensions were measured as shown in [Table/Fig-1a,b]. Length of the sigmoid colon in relation to pelvic brim and root of sigmoid colon along the mesenteric and antimesenteric border was noted. Considering the pelvic brim as the reference point, two points corresponding to the apex of the pelvic brim on either side of the loop was pinned. With the help of a string, the length of the sigmoid was measured along the mesenteric (l1) and antimesenteric border (L1). Similarly, with reference to the two ends of the sigmoid mesocolon, extent of the colon along mesenteric (l2) and antimesenteric borders (L2) of the loop was noted.
Schematic illustration showing points regard to pelvic brim (a) and root of sigmoid mesocolon (b)
L1 and L2 – length along the antimesenteric border of sigmoid colon l1and l2 – length along the mesenteric border
W1 and W2 – width of the mesocolon; H1 and H2 – height of the mesocolon
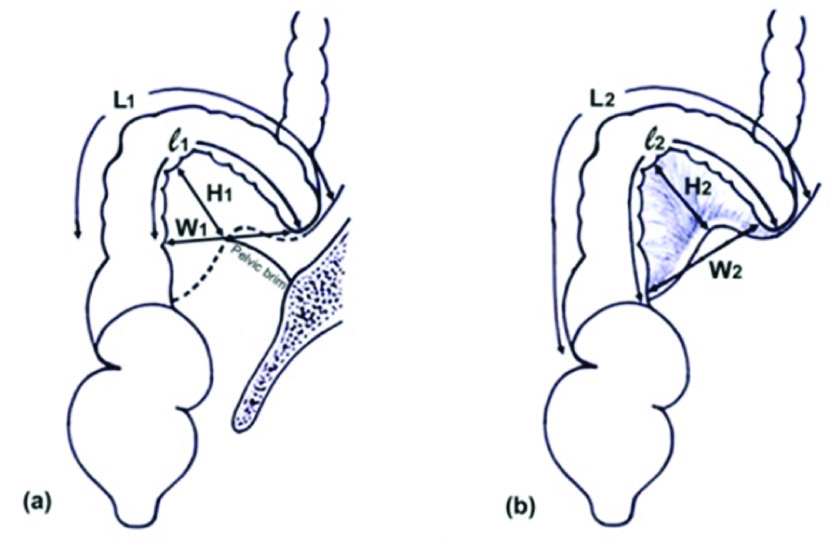
The width and the height of sigmoid mesocolon were also measured in relation to pelvic brim and root of sigmoid mesocolon on full stretch of the sigmoid loop. Width of the sigmoid mesocolon with reference to pelvic brim (W1) and root of sigmoid mesocolon (W2) was measured. From the pelvic brim to the highest point of the sigmoid mesocolon was considered as height (H1). Vertical length from the midpoint of root of sigmoid mesocolon to the Highest point of mesocolon was taken (H2).
Statistical Analysis
As 10 cadavers had fixed sigmoid colon (the sigmoid colon had very short mesocolon, thus rendered immobility to sigmoid colon), measurements were taken only in 21 cadavers. The data obtained was analysed using SPSS package version 16.0. Categorical data were presented as number and percentages. Continuous data were presented as mean and standard deviation. Association between categorical variables has been studied using chi-square test (Fisher exact test). Relationship between the continuous variables has been studied using correlation (Spearman rank correlation). Mann Whitney U-test was used to find the difference of sigmoid colon parameters among gender and position. Kruskal-Wallis test was used to find the difference of sigmoid colon parameters among type of sigmoid colon.
Results
Type and Position of Colon
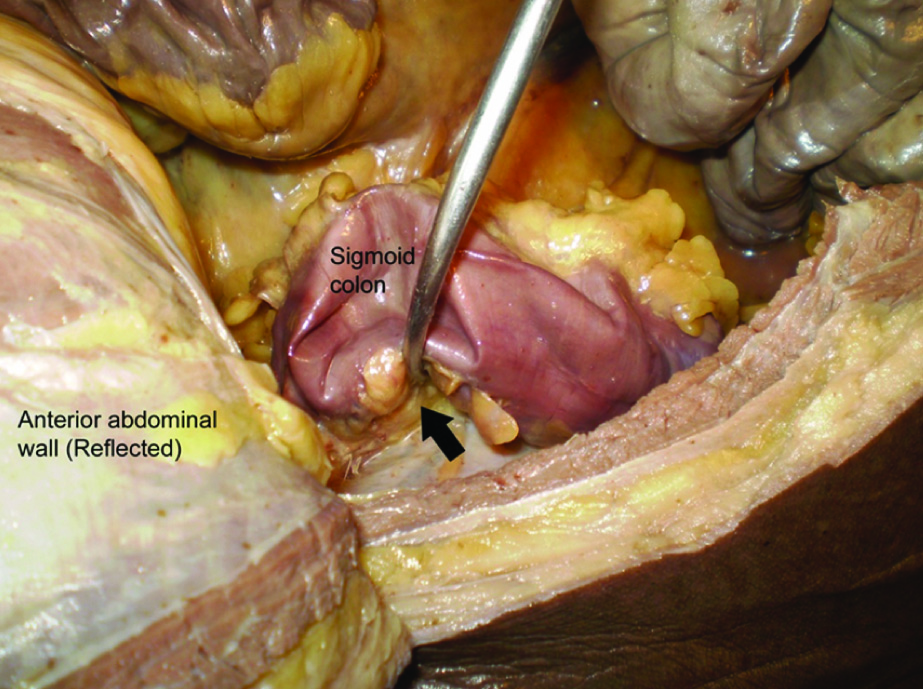
The age range of cadavers was 45 - 93 years, 62% being males and the rest females (38%). Surprisingly, 32.2% of the sigmoid colons examined, i.e., 10 out of 31 were of fixed type [Table/Fig-2]. Of the rest, majority of the sigmoid colon fell into the classical type (47.6%) followed by 33.3% being long- narrow type and 19% long-broad type. There was no significant correlation between the length of sigmoid colon and its various types. There was a significant difference regarding the position of sigmoid colon, the pelvic position being more common than the suprapelvic position [Table/Fig-3].
Photograph showing fixed sigmoid colon. The anterior abdominal wall has been reflected and sigmoid colon retracted. Arrow indicates very short sigmoid mesocolon
Sigmoid colon length along the mesenteric border with regard to pelvic brim (l1) and mesenteric root (l2), its relation to various shapes and position of sigmoid loop.
| Shape of sigmoid colon | p-value |
|---|
| Long broad(n = 4) | Classical(n = 10) | Long narrow(n = 7) |
|---|
| Length along mesenteric border l1 (Mean ± SD) | 16.86 ± 5.34 | 13.80 ± 4.19 | 16.10 ± 4.41 | .364 |
| Position assumed by the sigmoid colon loop | Pelvic (n = 13) | 12.92 ± 3.59 | | | | .003 |
| Supra-pelvic (n = 8) | 18.78 ± 3.23 | | | | |
| Length along mesenteric border l2 (Mean ± SD) | 21.23 ±6.09 | 16.86 ±4.82 | 21.46 ±7.41 | .280 |
| Position assumed by the sigmoid colon loop | Pelvic | 16.72 ±5.03 | | | | .015 |
| Supra-pelvic | 23.25 ±5.85 | | | | |
There was no significant positive correlation between the position and type of sigmoid colon with age and gender. The long- narrow and long-broad types were more prevalent in males whereas classical among females as shown in [Table/Fig-4].
Association of Type of Sigmoid colon in Males and Females
| Long —broad (n = 4) | Classical (n = 10) | Long- narrow (n = 7) |
|---|
| Male | 75% | 40% | 85.7% |
| Female | 25% | 60% | 14.3% |
Sigmoid Colon Length
The length of sigmoid colon along the mesenteric border ranged from 8.6 – 23.2cm (Mean 15 ± 4.45) and 11- 34.6cm (Mean 19.2 ± 6) considering the pelvic brim and root of mesentery as reference points of measurement respectively. The colon length along antimesenteric border ranged from 10.4 - 41.5cm (Mean 22 ± 7.9) and 11.9 – 45.5cm (Mean 25 ± 8.7) along the same reference points [Table/Fig-5]. The length of sigmoid colon was significantly higher in males when compared with females [Table/Fig-6]. There was statistically significant negative correlation between the age and sigmoid colon length in male alone.
Sigmoid Length with regard to pelvic brim and root of sigmoid mesocolon along the mesenteric and antimesenteric border
| Reference points | Border | Total (n = 21) Mean ±SD | Minimum | Maximum |
|---|
| Sigmoid colon length (cm) | Pelvic brim | Mesenteric (l1) | 15± 4.45 | 8.6 | 23.2 |
| Antimesenteric (L1) | 22±7.9 | 10.4 | 41.5 |
| Root of sigmoid mesocolon | Mesenteric (l2) | 19 ± 6 | 11 | 34.6 |
| Antimesenteric (L2) | 25 ± 8.7 | 11.9 | 45.5 |
Gender Comparison of Length of Sigmoid Colon in Males and Females
| Sigmoid colon length | Males | Females | p-value |
|---|
| Mean±SD | Median | Mean±SD | Median |
|---|
| Pelvic brim | Mesenteric (l1) | 17 ± 3.8 | 17 | 11.6 ± 3 | 11 | 0.003 |
| Antimesenteric (L1) | 22 ± 5 | 23 | 14 ± 3 | 13 | 0.001 |
| Root of sigmoid mesocolon | Mesenteric (l2) | 25 ± 7 | 23 | 18 ± 7 | 16 | 0.025 |
| Antimesenteric (L2) | 28 ± 8 | 26 | 20 ± 7 | 16 | 0.019 |
Analysis was also done to determine any correlations between the various parameters themselves. It showed that the length of the sigmoid colon correlates positively with the height of the mesocolon.
Sigmoid Mesocolon
The measurements of mesocolon height ranged from 1.5 – 15.4cm with reference to pelvic brim and 2.0 – 14.8cm with reference to root of mesentery respectively. The width of mesocolon ranged from 2.5 – 14.3cm (pelvic brim) and 4.5 – 11.6cm (root of mesentery) [Table/Fig-7]. When the height of sigmoid mesocolon (along both reference points) was correlated with gender, it was found that the sigmoid mesocolon was significantly longer in males when compared with females. The width of mesocolon along the pelvic brim was also statistically wider in males compared to those of females [Table/Fig-8]. There was no significant difference between age and the height and width of mesocolon.
Height and Width of Sigmoid Mesocolon with regard to pelvic brim and root of sigmoid mesocolon
| Reference points | Total (n = 21)Mean ±SD | Minimum | Maximum |
|---|
| Height of Sigmoid mesocolon | Pelvic brim (H1) | 6.5 ± 3 | 1.5 | 15.4 |
| Root of sigmoid mesocolon (H2) | 7.3 ± 3 | 2 | 14.8 |
| Width of Sigmoid mesocolon | Pelvic brim (W1) | 7.4 ± 3 | 2.5 | 14.3 |
| Root of sigmoid mesocolon (W2) | 8 ± 2 | 4.5 | 11.6 |
Gender Comparison of Height and Width of Sigmoid mesocolon in Males and Females
| Males | Females | |
|---|
| Mean ±SD | Median | Mean ±SD | Median | p-value |
|---|
| Height of Sigmoid mesocolon | Pelvic brim (H1) | 7.7 ± 3 | 7.6 | 4.5 ± 0.8 | 4.4 | 0.002 |
| Root of sigmoid mesocolon (H2) | 8.5 ± 3 | 8.5 | 5.3 ± 1.6 | 5.4 | 0.005 |
| Width of Sigmoid mesocolon | Pelvic brim (W1) | 8.4 ± 3 | 8 | 5.8 ± 2 | 6.6 | 0.032 |
| Root of sigmoid mesocolon(W2) | 8.4 ± 2 | 8.8 | 7.2 ± 1.9 | 7.8 | 0.218 |
Discussion
The morphology of sigmoid colon has been considered as one of the prime factor in the development of sigmoid volvulus [7]. Akinkuotu et al., reported in African population, longer sigmoid colon and mesosigmoid colon in sigmoid volvulus when compared with controls [8]. Sigmoid volvulus is characterised by the twisting of the sigmoid colon and its mesentery around at least one point of fixation [9]. An interesting geographical distribution has been described in the incidence of sigmoid volvulus that included the Indian population as one of the leading nations [1]. This led us to compare the normal morphology of sigmoid colon with studies done in other ethnic/geographical groups.
This study describes the morphometric measurements of sigmoid loop in cadavers which have found to be not different from living subjects as reported by Alatise et al., [6]. The sigmoid colon length and the height and width of sigmoid mesocolon were assessed at two levels, one being with regard to pelvic brim and the other in relation to mesenteric root. This was done so as to compare our results with the different methods of measurements taken by the previous studies both among Indian group and with other population groups. Madiba et al., [5] have measured the sigmoid loop length along the mesenteric border and the width and height of mesocolon with regard to pelvic brim unlike Bhatnagar et al., Alatise et al., Atamanalp et al., whose sigmoid length were measured in antimesenteric border and mesocolon width and height were in relation to mesenteric root [3,6,7]. A comparison of length of sigmoid colon with previous studies [3,6,7] is shown in [Table/Fig-9].
A Comparison of parameters with previous studies
| Antimesenteric border | Mesenteric border |
|---|
| Alatise et al., [6] (Nigeria) | Bhatnagar et al., [3] (Indian) | Atamanalp et al., [7] (Turkey) | Present study (South Indian) | Madiba et al., [4] | Present study (South Indian) |
|---|
| African | Indian | White |
|---|
| Sigmoid length in cm (L2)Range (Mean ± SD) | 38 – 62cm(50.1 ± 1.6) | 18.5 – 43.0(28 ± 7.6) | 20 – 84(43.7 ± 8.9) | 11.9 – 45.5(25.1 ± 8.7) | 29.6 ± 12.1 | 20.6 ± 9.2 | 22.6 ± 12.4 | 15.5 ± 4.4 |
| Sigmoid mesocolon | With reference to root of sigmoid mesocolon | With reference to pelvic brim |
| Width in cm | 4.0 – 11.0(6.5 ± 0.3) | 3.0 – 12.0(5.6 ± 1.4) | 4 – 16(8.6 ± 1.5) | 4.5 – 11.6(8.0 ± 2.17) | 8.3 ± 2.5 | 9.55 ± 2.8 | 9.8 ± 3.4 | 7.4 ± 2.9 |
| Height in cm | 8.0 – 19.0(14.1 ± 0.5) | 7.5 – 23.0(13.7 ± 3.5) | 9 – 42(19.3 ± 4.6) | 2.0 – 14.8(7.3 ± 3.1) | 8.9 ± 4.8 | 6.4 ± 2.9 | 6.5 ± 3.9 | 6.5 ± 2.9 |
In the current study, 32.2% of the sigmoid colons examined were of fixed type. They had very short mesocolon, thus rendering the sigmoid colon immobile. This type of sigmoid colon has not been considered earlier in previous studies. Knowledge about this type should be thought of by the gastroenterologist while performing colonoscopy.
Comparison of Length of Sigmoid Colon
In the present study, there was a wide range in the length of sigmoid colon. Studies have shown that the sigmoid colon length was considerably more in Africans [5]. Barium enema films of patients of the same population groups were also studied by Madiba et al., and the results showed longer sigmoid loop among Africans, followed by Whites and then Indians [4]. The present study is in accordance with Bhatnagar et al., who reported shorter sigmoid colon in Indian group [3]. The difference in the length of sigmoid colon could be attributed to the different ethnic groups. In a radiological study done among the Calabar community in Nigeria, Bassey suggested that chronic use of enema along with the instrumentations used to deliver the concoction results in the lengthening of loop [10]. This could be responsible for a similar finding by Madiba et al., [5] belonging to the same continent.
Comparison of Width and Height of Sigmoid Mesocolon
A long mesocolon with a narrow base forming a long-narrow loop was predominant in African group compared to others which suggests that they are a more vulnerable group for sigmoid colon torsion [5]. The term ‘dolichomesentery’ is being used to describe the same characteristics by Bhatnagar et al., and they found it to be the commonest in Indians. This pattern of mesocolon is considered as a prerequisite for volvulus whose frequency is high in endemic areas such as in Africa, Asian, South America and Eastern and Northern European countries [3,5,7,11–13]. The present study showed more of classical type in South Indian population. In fact, in the present study 10 cases had fixed and short sigmoid colon.
Gender Differences
Though the anatomical textbooks do not mention a gender difference in sigmoid morphology, several articles quote a male preponderance to sigmoid volvulus attributing it to longer redundant sigmoid loop in males. The gender analysis in the present study showed that males had statistically significant longer sigmoid loop which is in accordance with the previous studies done by Alatise et al., Atamanalp et al., and Saidi et al., in African, Nigerian and Turkish population [6,7,14], though Bhatnagar et al., and Madiba et al., in Indian population did not find any gender difference. The height of mesocolon was also significantly higher in males in the present study which is contrary to Bhatnagar et al., and Madiba et al., [3,4]. The preponderance of the parameters in males could explain the results obtained in a study on sigmoid volvulus in Middle East by Heis et al., [15]. Lal et al., describes a “volvulus belt” that encompasses Africa, India, Iran and Russia and South America where again the male to female ratio was 2: 1 [1]. In addition to the length and height of sigmoid colon, the smaller pelvic inlet size in males which does not allow sufficient mobilisation of enlarged colon could predispose to torsion [16], whereas, the spacious pelvis and lax abdominal wall could attribute to less prevalence in females [17,18].
Age difference
In the present study correlation of age with the sigmoid length (both with regard to pelvic brim and mesenteric root) in males was shown to have significant negative correlation with age. Alatise et al., reported increase in length of sigmoid colon and mesocolon with age [6]. Yamazaki et al., also found a similar positive correlation while, Sadahiro et al., showed a negative correlation with age [19,20]. However, authors like Bhatnagar et al., Atamanlp et al., found no correlation of parameters with age or its correlation with various measurements in both gender [3,7]. The different results among various authors could be attributed to different methods of study or ethnical variations.
Position of Colon
A significant proportion of men had a suprapelvic colon among the African group in Madiba et al., but no such significance was identified in the present study.
Conclusion
To conclude, though the present study is limited by the small sample size it establishes the morphology of sigmoid colon and its mesocolon in South Indian population. High incidence of fixed sigmoid colon has been reported for the first time. Classical type of sigmoid colon is more prevalent in South Indian population. It is longer in males than in females and males have more of long-narrow types compared to females. This finding, no doubt contributes to the literature that explains male preponderance in the manifestation of sigmoid volvulus in various geographical areas. In addition, we found a decrease in sigmoid colon length as age advances, unlike previous reports in literature. All the more, the present study has an added advantage of considering all the parameters with regard to pelvic brim and root of sigmoid mesocolon in order to substantiate the findings by other authors. Though India is considered a part of the volvulus belt, no literature is available regarding the incidence of sigmoid volvulus in South Indian population. There is a need for further studies to substantiate its incidence in South Indian population considering the high incidence of fixed sigmoid colon.