Aetiology, diagnosis and treatment of temporomandibular disorders (TMDs) are still controversial. The guidelines of the American Academy of Orofacial Pain suggest a link between TMD and cervical spine. Mehta et al., listed “the ‘triad of dysfunction’, which incorporate myofascial pain and dysfunction, Internal derangement of the temporomandibular joint (TMJ) and cervical spine dysfunction (CSD)” [1].
There are numerous types of associations between the cervical spine and the craniofacial region i.e. anatomic, biomechanical, neurological, and pathological [2]. The relationship between the position of the head and neck and incidence of TMD is a common research topic which has not become so fruitful even after years of research.
Still, many reports suggest that cranial and spinal postures may be contributing factors for TMD [3–6]. Others do not support the hypothesis of head and craniocervical posture to be a predisposing factor for temporomandibular disorders [7–10].
The objective of the present study was to evaluate head and craniocervical posture among individuals with and without TMD and its subtypes by photographic and radiographic method.
Materials and Methods
Sample
The present study was conducted in the Department of Oral Medicine and Radiology, The Oxford Dental College and Hospital, Bengaluru for the duration of 1 year (2012 August to 2013 August).
The reason for the selection of sample size was done based on previous studies and in consultation with the statistician. As the patient flow was more a few more patients were added in the sample so that the authenticity of the study may be improved. Accordingly the initial sample size was 20 which were increased to 34. Final calculations were done based on the increased sample.
The study group consisted of 34 TMD Patients between the age group of 18-50 years and 34 age and sex matched control patients visiting the outpatient department.
The TMD subjects were carefully chosen based on Research Diagnostic Criteria [2] for TMD’s (RDC/TMD) and were allocated into 2 groups: Group I (17 patients), muscle disorder; Group II (17 patients), disc displacement. It included patients with age ranging from 18-50 years without any medical illness, who are diagnosed with muscle disorders and disc displacement as per RDC criteria for both the Groups i.e. Group I (muscle disorders) and group II (disk displacement) . In muscle disorders only muscular tenderness is the criteria for inclusion in the group 1, whereas in disk displacement along with muscular pain mouth opening is also considered.
The exclusion criteria considered for both the groups were any medical illness, physical deficiency, neurological problems, and patients undergoing orthodontic treatment, current use of dental prosthesis, previous mandibular fracture or previous orthognathic surgery.
An informed consent was taken and detailed TMJ, masticatory and neck muscle examinations were performed among all the participants. A brief methodology was explained and they were subjected to both photographic and radiographic methods of evaluation. The study protocol was accepted by ethical committee of RGUHS.
Photographic Analysis
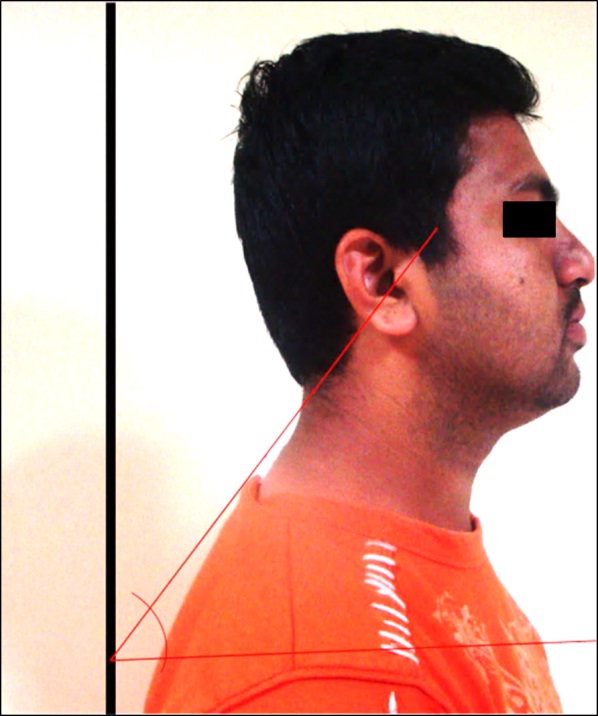
The skin overlying the tip of the seventh cervical spinous process was palpated and indicated by an adhesive marker. To standardize head posture, the participants were instructed to look into his eyes in a mirror placed in front of him and a lateral photograph was taken using camera (SONY cyber-shot 7.2 mega pixels) mounted on a leveled tripod, at a fixed distance (approximately 1.5m) from patients right side. The skin markings were always positioned by the same investigator, who also took all the photographs. A free hanging plumb line was used to define the true vertical axis on the photographs. On photographs the angle between the horizontal plane (the line perpendicular to true vertical axis) and a line between the tragus of the ear and seventh cervical spinous process was measured [Table/Fig-1].
Photographic Method for Head Posture evaluation
Radiographic Analysis
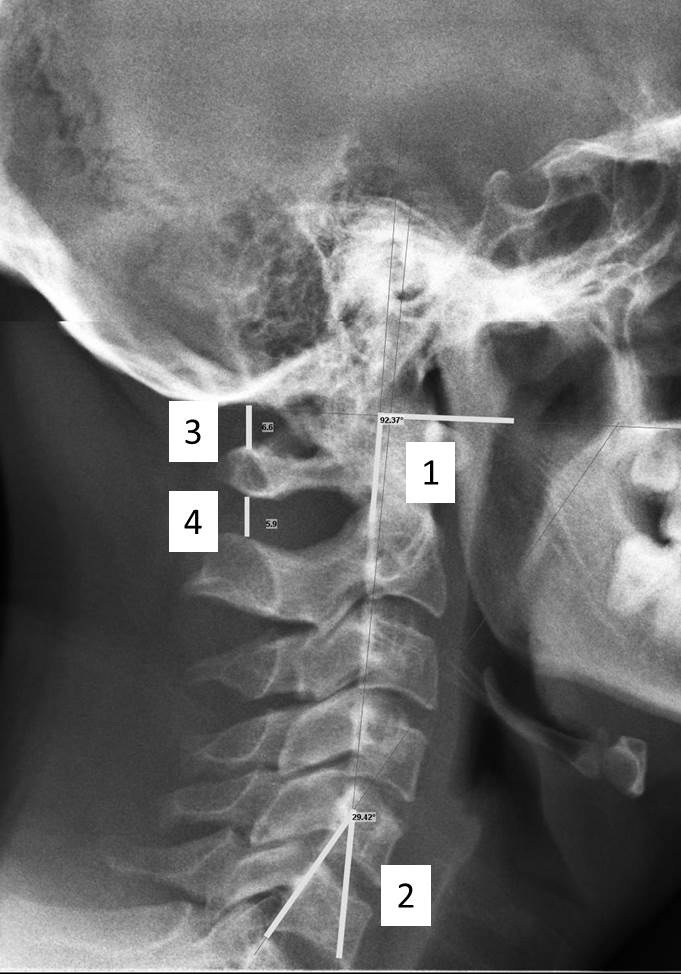
In order to interpret the relationship of the cranium with cervical spine the radiograph of the patients was taken in the self-balanced position. The lateral skull radiograph of the cranium and cervical spine was taken in digital radiographic machine (Planmeca Prolin XC) to evaluate the head and cervical posture. Exposure factors varied in accordance with the biotype of each subject in the study. (Depending on the patients build, structure and bone density mild changes in exposure parameters, but no changes have been made in posture). For analyses of craniocervical changes, the following 4 parameters [Table/Fig-2] were measured by using computer software i.e. Planmeca Romexis 2.1.1.R [Table/Fig-3].
Parameters used for radiographic analysis of craniocervical posture
| 1 | Craniocervial Angle (CCA) | The angle between McGregor plane (tangent drawn from most inferior surface of the occipital bone until it reaches the posterior nasal spine on the hard palate) and tangent line to the posterior surface of odontoid apophysis [5,6]. |
| 2 | Cervical Curvature Angle (C3-C6) | The angle between the extended line from the posterior margin of the third and sixth cervical vertebral body [6]. |
| 3 | Suboccipital Space (C0-C1 distance) | The perpendicular distance from the base of the occipital bone to the postero-superior point of the first cervical vertebra [11,12]. |
| 4 | Atlas-Axis Distance (C1- C2 distance) | The perpendicular distance from the most infero-posterior point of the posterior arch of the atlas to the most supero-posterior point of the spinous process of axis [11,12]. |
Lateral skull radiograph with Craniocervical Posture parameters
1. Craniocervial Angle (CCA)
2. Cervical Curvature Angle (C3-C6)
3. Suboccipital Space (C0-C1 distance)
4. Atlas-Axis Distance (C1- C2 distance)
Statistical Analysis
To analyse the head and craniocervical posture among individuals with and without TMD, t-test was performed. The association between cervical myofascial pain and TMD groups was analysed by Chi-square test. Means and standard deviation were calculated. The SPSS 17 package windows program was used for statistical analysis. A p-value less than 0.05 were considered as statistically significant.
Results
Demographic characteristics of TMD and control groups (n=34) revealed 19 females and 15 males with majority belonged to the age range of 20-30 (62%) years.
Photographic head posture angle and radiographic craniocervial angle (CCA) showed no statistical significant difference (p > 0.05) between Group I, Group II and control group [Table/Fig-4]. However, statistical significant difference was noted with Atlas-Axis Distance (c1- c2 distance) among Group II (p = 0.001) and cervical curvature angle among Group I (p = 0.045) individuals.
Comparison of mean head posture angle, craniocervical angle, cervical curvature angle, suboccipital distance & atlas-axis distance between TMD groups and control group
| Parameter | Group | Mean | ±SD | p-Value |
|---|
| Head Posture Angle | Group I | 43.58 | 7.63 | 0.998 |
| Group II | 43.00 | 4.67 | 0.740 |
| Control Group | 43.59 | 5.42 | |
| Craniocervical Angle | Group I | 95.79 | 8.82 | 0.920 |
| Group II | 91.01 | 7.69 | 0.147 |
| Control Group | 93.20 | 15.61 | |
| Cervical Curvature Angle | Group I | 13.90 | 6.13 | 0.045 |
| Group II | 12.62 | 9.47 | 0.484 |
| Control Group | 10.28 | 7.84 | |
| Suboccipital Distance | Group I | 6.90 | 2.84 | 0.844 |
| Group II | 8.69 | 3.68 | 0.093 |
| Control Group | 7.07 | 2.46 | |
| Atlas-Axis Distance | Group I | 5.29 | 2.77 | 0.216 |
| Group II | 6.68 | 1.19 | 0.001 |
| Control Group | 4.31 | 2.15 | |
Discussion
Craniofacial pain encompasses pain in the head, face, and related structures that originate from a variety of conditions, organs, and aetiologies [2].
The increased Craniocervial angle (CCA) are implicated with an exaggerated posterior rotation of the head that may cause a lot of alterations, such as reduction of the suboccipital space with signs of craniofacial pain and strong tension in the supra and infra hyoid musculature. Anterior rotation of the head may be related to lower CCA which may be associated with concurrent increase in Suboccipital space, kyphosis and increased tension in the soft tissue part of posterior part of cranial vertebra [5].
There is ample evidence in literature of studies regarding craniocervical posture and TMD. Some are positive [2,13] and some are negative [14] and even some suggest that the anterior positioning may be more as a result of TMD rather than cause for it [11]. The study population, the methods employed etc, may also contribute to these varied results.
In the present study majority of TMD subjects were belonged to the age range of 20-30 (62%) year with a females predominance which supports the various studies in the literature [6,7].
We had assessed Head Posture by both photographic and radiographic method (CCA). Results revealed that no significant difference (p > 0.05) in head posture between group I, II and control group, thus agreeing with the results of Visscher et al., Ciacanglini et al., Munhoz et al., Hackney et al., Lunes DH et al., and Matheus RA et al., [4,5,8–10,14].
Motta LJ et al., suggested three linear distances and two angles to measure head posture by photographic method to assess relationship between forward head posture and TMD. The results revealed that the angle between the horizontal plane and a line between the tragus and the skin overlying the tip of the 7th cervical spinous process was the only one that showed statistically significant difference between the TMD patients and controls [15], which is contradictory to our results.
The data from the present study disagrees with the findings of Darlow et al.,, Braun et al.,, Huggare & Raustia, Hackney et al., Lee et al., who suggested positive relationship between TMD and head posture [13,14,16–18]. Braun, Lee et al., used the same photographic technique, which gave a positive relationship between head posture and TMD [13,17], whereas Hackney et al., yielded a negative result [14]. Often different techniques and sometimes unspecified patient groups were used. The well-defined classification and RDC criteria for selection of our participants led us to the conclusion that there is no relationship between head posture and TMD.
As TMD has multifactorial aetiology, during selection of present study group aetiological factors like trauma, parafunctional habits, clinical occlusal evaluation and systemic illness were excluded out. The present study also revealed that head posture did not have a significant role in the causation of TMD. Role of other aetiological factors like emotional stress, hormonal factors, functional occlusal loading could be considered in the present study subjects.
In the present study, we found increased Atlas-Axis Distance (c1- c2 distance) among Group II which was statistically significant (p = 0.001). These results were not in accordance with the studies conducted by Lunes et al., and Farias Neto JP et al., [3,4].
As per our study we could not find any positive correlation between head posture and TMD. Even though there was statistical significance in one of the parameter (Co-C1 space) overall correlation was not considered. Thus our result supports the results of Matheus RA et al., [5].
Cervical curvature angle was used between C3 and C6 in radiographic analysis as the seventh cervical vertebra was often not completely visible because of overlap on the shoulder girdle. The increased cervical curvature angle showed statistically significant (p = 0.045) between Group I and control group. This suggests that cervical lordosis was present in Group I i.e. myogenous group only.
The data from the present study agrees with the findings of Matheus et al., Visscher et al., and Munhoz et al., who did not find any alteration in the positioning of the cranium and in the angulation of the cervical spine [5,8,19]. However, Fatma A. El-Hamalawy supported the relation between forward head posture and TMD. He studied forward head postural exercise on myogenic TMD who showed significant decrease in crainocervical angle and lower cervical curvature with improvement in myogenic TMD [6].
Future recommendations in order to support a cause-effect relationship, more rigorous studies should be conducted among large sample size. For assessment of head posture different authors have used different parameters which lead to varied results and made difficulty in comparing their results with our study. Therefore need of standardization of parameters is recommended for better results.
Limitations of The Study
Sample size in the present study was small and duration of the study was short. More studies with large sample size and longer duration are needed.
Conclusion
The head and cervical posture did not influence the occurrence of TMD, according to photographic and radiographic analyses. However, myogenous group exhibited correlation in cervical alignment. It could be declared that the muscular component plays a more significant role in the production of TMD rather than the articular component. If a positive correlation between the cervical posture and temporomandibular joint disorder is established preventive measures becomes easier. In the world of advanced technology of computers and computer professional’s posture related occupational hazards are more, so if cervical posture is a contributory factor and if it can be established by photographic and radiographic methods it will help in formulating treatment strategies.