Unruptured Noncoronary Sinus of Valsalva Aneurysm Associated with Atrial Septal Defect (ASD)
Kartik Mittal1, Divyesh Dadhania2, Amit Kumar Dey3, Rohit Gadewar4, Priya Hira5
1 Post Graduate Student, Department of Radiology, Seth GS Medical College and K.E.M Hospital, India.
2 Post Graduate Student, Seth GS Medical College and KEM Hospital, India.
3 M.B.B.S Student, Department of Radiology, Seth GS Medical College and KEM Hospital, India.
4 Post Graduate Student, Department of Radiology, Seth GS Medical College and K.E.M Hospital, India.
5 Additional Professor, Department of Radiology, Seth GS Medical College and KEM Hospital, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kartik Mittal, Post Graduate Student, Department of Radiology, Seth G.S. Medical College and K.E.M. Hospital, Room No. 107, Main Boy’s Hostel, Acharya Donde Marg, Parel, Mumbai-400012, Maharashtra, India.
E-mail: amit3kem@gmail.com
Sinus of Valsalva aneurysms are rare cardiac anomalies. Incidence of this anomaly is higher in Asian population with male preponderance. Our case highlights a rare association between unruptured sinus of Valsalva aneurysm and atrial septal defect (ASD). Rarely diagnosis of sinus of Valsalva aneurysm is missed on two dimensional echocardiography. Multi slice CT scan is done to confirm echocardiographic findings and to detect any missed complications, other cardiac abnormalities and anatomy for a precise surgical approach.
Aortic regurgitation, Chest pain, Echocardiography
Case Report
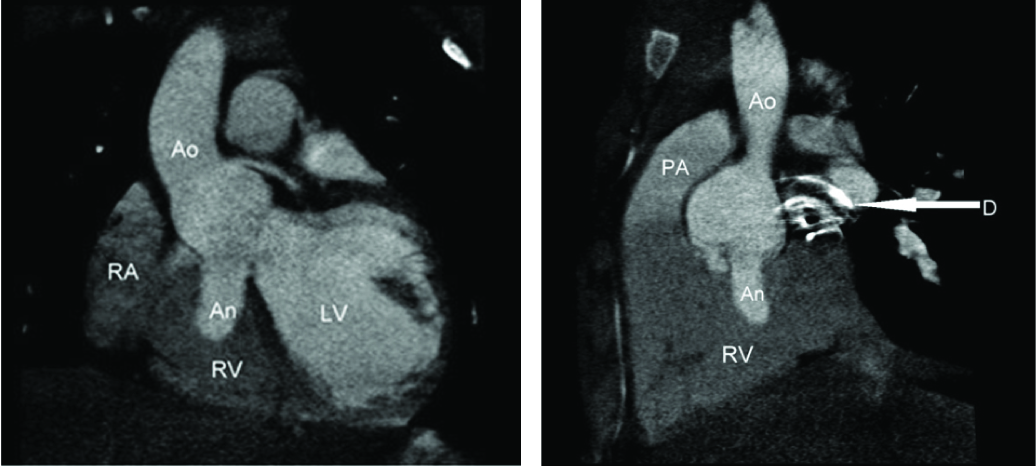
A 15-year-old male patient with past history of atrial septal defect (ASD) closure done at the age of five years, presented with chest pain. On examination pulse rate was 84/min, RR was 20/min, BP 120/70 mmHg with grade 2/3 pan systolic murmur. Plain Chest X-ray revealed surgical clips of ASD closure. Patient underwent 2D echocardiography during evaluation which revealed saccular dilatation of non coronary sinus superior to the aortic annulus with mildly dilated aortic root projecting into the right atrium measuring 4x4 cm in size without any signs of rupture. Right and left coronary sinuses were normal with normal right ventricle (RV)/Left ventricle (LV) function and associated aortic regurgitation. A diagnosis of unruptured non-coronary sinus of Valsalva aneurysm was made. For confirmation and pre-operative planning ECG gated contrast CT was done which revealed an out pouching from the non-coronary cusp with same contrast intensity as seen in aorta [Table/Fig-1a,b]. Metallic closure device of ASD was also seen on CT [Table/Fig-1b,c], hence the diagnosis of sinus of Valsalva aneurysm was confirmed. Despite of the giant sinus of Valsalva aneurysm requiring surgical intervention, patient refused surgery. Because surgical intervention was not possible medical management with beta blocker was advised with six monthly follow up by 2D Echo. After 3 follow-ups, neither did the aneurysm increase in size nor was the patient symptomatic.
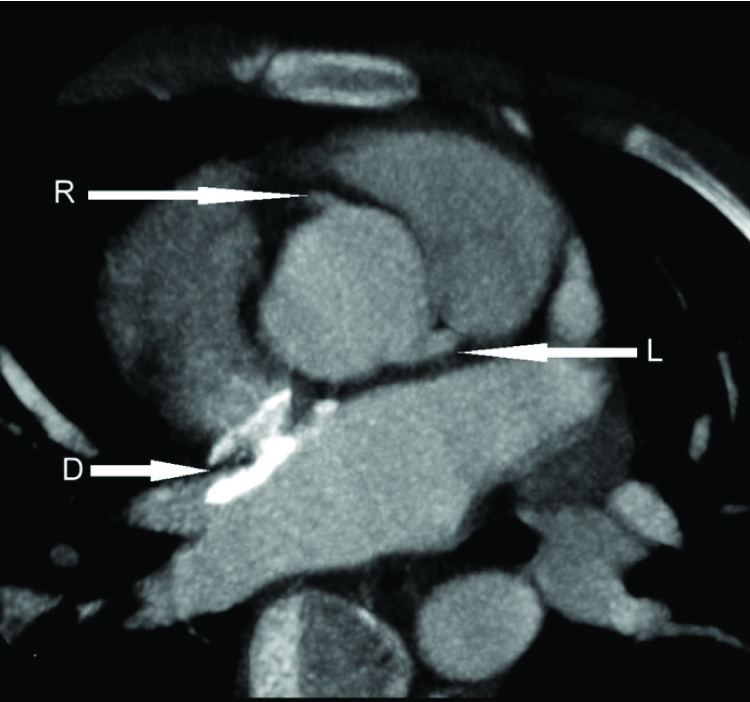
[Table/Fig-1]: (a&b) ECG gated contrast enhanced cardiac CT reformatted images in coronal (1a) and sagittal (1b) plane showing unruptured aneurysm (An) of size 2.7cm x 1.3 cm x1.2 cm (CC X TR X AP) arising from the non-coronary sinus of valsalva protruding into the right ventricle (RV). Metallic ASD closure device [D] seen in figure 1b. LV indicates left ventricle. RA indicates right atrium. Ao indicates aorta. PA indicates pulmonary artery. D indicates ASD closure device. (c) Normal origin of right coronary artery[R] and left main coronary artery [L] from respective normal coronary sinus seen. Metallic ASD closure device [D] seen
Discussion
There are very few cases in clinical literature with unruptured sinus of Valsalva aneurysms. Most commonly these aneurysms are from right aortic sinus, sometimes from non coronary sinus and rarely from left coronary sinus [1]. These aneurysms are five times more common among Asians as compared to Caucasians [2]. They are more common in men as compared to women [2]. Both unruptured and ruptured sinus of valsalva aneurysms is associated with potentially life threatening complications. Presentation of an uncomplicated unruptured sinus of valsalva aneurysm is very rare. The clinical manifestations of sinus of valsalva aneurysms vary widely. Patient tends to present with aneurysm rupture or symptoms due to the mass effect [3].
Commonly the non ruptured aneurysms are discovered as an incidental finding from an echocardiography while evaluating murmurs or from abnormal cardiac contours on radiological imaging [3]. Aortic valve regurgitation is frequently associated with sinus of Valsalva aneurysms and can have a prevalence rate of up to 44% [4]. Bulkley et al., reported two patients in which aneurysms of the non-coronary sinus projected into the right atrium and caused tricuspid incompetence [5]. Multiple published cases were reported in which a nonruptured sinus of Valsalva aneurysm had partially obstructed the right ventricular outflow tract [6–9]. Also, cases were reported in which a non ruptured Valsalva sinus aneurysm had dissected into the interventricular septum [10,11] at the time of manifestation [12]. In our case, the patient presented with chest pain which can be angina secondary to myocardial ischemia and with a pan systolic murmur which can be secondary to a tricuspid regurgitation on account of the aneurysm extending into the right atrium [12]. However, they can rarely present with chest pain, continuous murmur or right ventricular outflow tract (RVOT) obstruction and tricuspid regurgitation. However, there were no such changes on echocardiography which means they were temporary findings. Aortic regurgitation in this patient is most likely related to the aortic root dilation. While doing imaging studies, the criteria for diagnosing a Valsalva sinus aneurysm are an origin above the aortic annulus, a saccular shape, and normal dimensions of the adjacent aortic root and ascending aorta [12]. Small sized unruptured aneurysms as in the case of this patient can be kept under observation however surgery is offered in case of suspected complications [12]. Right and non-coronary sinus rupture into right side causing left to right shunt and can lead to heart failure [Table/Fig-2] SOVA is easily diagnosed on colour Doppler echocardiography. Nevertheless contrast CT or MR provide much better spatial resolution and anatomical details with 3D reformation which are invaluable in surgical planning. MR is advantageous in depicting left ventricular haemodynamics and aortic regurgitation but CT is less time consuming and preferred. Surgery is the preferred treatment in case of ruptured aneurysm. In unruptured sinus of Valsalva aneurysm, symptoms of cardiac dysfunction and progression are important determinants. However, there is controversy regarding surgical intervention in unruptured and asymptomatic patients [12].
Diagrammatic depiction of complication of right and non-coronary sinus in the form of rupture into right side causing left to right shunt. RVOT indicates right ventricular outflow tract. LA indicates left atrium and LAA indicates left atrial appendage. RA indicates right atrium

Conclusion
Our case demonstrates unusual association between ASD and unruptured sinus of Valsalva aneurysm. Rarely diagnosis of sinus of Valsalva aneurysm is missed on 2D echocardiography which can easily diagnosed by Contrast enhanced ECG gated CT scans. Nonetheless CT is required for its complication, associated cardiac anomalies and gives anatomical details which help in surgical approach. Patient is doing well even after 18 months. Sinus of Valsalva aneurysm is a rare finding and is usually diagnosed on 2D echocardiography. Surgery is the treatment of choice.
[1]. Thankachen R, Unruptured aneurysm of the sinus of valsalva presenting with right ventricular outflow obstructionTex Heart Inst J 2003 30:152-54. [Google Scholar]
[2]. Mayer ED, Ruffmann K, Saggau W, Ruptured aneurysms of the sinus of ValsalvaAnn Thorac Surg 1986 42:81-85. [Google Scholar]
[3]. Feldman DN, Roman MJ, Aneurysms of the sinus of ValsalvaCardiology 2006 106:73-81. [Google Scholar]
[4]. Takach TJ, Reul GJ, Duncan JM, Cooley DA, Livesay JJ, Ott DA, Sinus of Valsalva aneurysm or fistula: management and outcomeAnn Thorac Surg 1999 68(5):1573-77. [Google Scholar]
[5]. Bulkley B, Hutchins GM, Ross RS, Aortic sinus of Valsalva aneurysm simulating primary right-sided valvular heart diseaseCirculation 1975 52:696-99. [Google Scholar]
[6]. Chung E, Baek JY, Chung HH, Park SI, Jang JH, Yu HA, A case of unruptured aneurysm of the right sinus of valsalva with right ventricular outflow obstructionKorean Circ J 2014 44(4):274-77. [Google Scholar]
[7]. John SH, A rare case of unruptured sinus of valsalva aneurysm obstructing the right ventricular outflowtractJ Cardiovasc Ultrasound 2010 18(2):55-57. [Google Scholar]
[8]. Gelfand EV, Bzymek D, Johnstone MT, Images in cardiovascular medicine: sinus of Valsalva aneurysm with right ventricular outflow tract obstruction—evaluation with Doppler, real-time 3-dimensional and contrast echocardiographyCirculation 2007 115(2):e16-e17. [Google Scholar]
[9]. Mohanakrishnan L, Vijayakumar K, Sukumaran P, Menon N, Prabu CR, Balaji S, Unruptured sinus of Valsalva aneurysm with right ventricular outflow obstructionAsian Cardiovasc Thorac Ann 2003 11(1):74-76. [Google Scholar]
[10]. Kalimanovska-Ostric D, Ostojic M, Petrovic P, Krotin M, Ostric V, Avramovic D, Unruptured congenital aneurysm of the right sinus of Valsalva. Dissecting into the interventricular septumTex Heart Inst J 1996 23(3):217-21. [Google Scholar]
[11]. Zannis K, Tzvetkov B, Deux JF, Kirsch EW, Unruptured congenital aneurysms of the right and left sinuses of ValsalvaEur Heart J 2007 28(13):1565 [Google Scholar]
[12]. Bricker AO, Avutu B, Mohammed TL, Williamson EE, Syed IS, Julsrud PR, Valsalva sinus aneurysms: findings at CT and MR imagingRadiographics 2010 30(1):99-110. [Google Scholar]