Clear Cell Hidradenoma of the Ear Lobule: An Unusual Site of Presentation
Neeraja Myreddy1, Venkata Ramanababu Pagatikaluva2, Suman Thirunamala Chenchu Subbarayula3, Sravani Peddaganganna Gari4, Bhavani Chinnappa Gari5
1 Professor and H.O.D, Department of Pathology, Government Medical College, Anantapuramu, Andhra Pradesh, India.
2 Associate Professor, Department of Pathology, Government Medical College, Anantapuramu, Andhra Pradesh, India.
3 Tutor, Department of Pathology, Governmant Medical College, Anantapuramu, Andhra Pradesh, India.
4 Assistant Professor, Department of Pathology, Government Medical College, Anantapuramu, Andhra Pradesh, India.
5 Assistant Professor, Department of Pathology, Government Medical College, Anantapuramu, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Venkata Ramanababu Pagatikaluva, Associate Professor, Department of Pathology, Government Medical College, Anantapuramu, Andhra Pradesh, India. E-mail : Pvramanababu22@gmail.com
The origin of hidradenoma was from the eccrine sweat glands, generally found in the head, face, and upper extremity regions. This lesion has not been reported to be large enough to present in the ear lobule. Hence, its description in the otolaryngology literature is extremely rare. The rarity of this neoplasm and failure to identify its morphologic features may lead to misdiagnosis. We present a benign clear cell hidradenoma of the right ear lobule in a 45-year adult male. We encountered a tumour measuring 4 cm in diameter. Mass shows ulcerated surface, bleeds on touch and remained a diagnostic dilemma till an excision biopsy was carried out and a histopathological report confirmed that it was a hidradenoma of clear cell variant. The aim of presenting this case report was interesting in the fact that it has added clear cell hidradenoma in the final diagnosis, in an uncommon site of presentation.
Controversial histogenesis, Skin adnexal tumour, Wide excision
Case Report
A 45-year-old male came to the Department of Otolaryngology, Government General Hospital, Anantapur, with complaints of mass over the right ear lobule for the last 6 months. The pain was dull aching in character, there is no history of trauma, or any other medical or surgical history of illness and no history of any other lump in the body. On examination, the right ear lobule showed mass like ulcerated growth. A mass were palpated in the right ear lobule which was tender on deep palpation, well circumscribed, of the size of a small orange, firm in consistency and adherent to the underlying structures but not to the overlying skin. The mass was non pulsatile and no bruit was heard on auscultation. The patient on further questioning revealed that this mass started as a small nodule observed 6 months back. The mass increased in size gradually but the patient ignored it till such time that he developed abnormal fullness, discomfort in the right ear, and the lesion occupying entire lobe of pinna (ear lobule). Thorough clinical examination of the affected right ear lobule was carried out to rule out any chronic infection, leading to lymphadenopathy. Examination of the other sites did not reveal any similar swelling. Haematological tests were performed, complete Haemogram, Erythrocyte sedimentation rate and C-reactive protein for any possibility of occult systemic ailment manifesting as ear lobule mass. In our institution biopsy was performed and histopathology finding was hidradenoma (clear cell variant). Wide tumour removal with lower 1/3 ear lobectomy under local anaesthesia was performed, keeping the upper 1/3 and middle 1/3 of auricle intact. In the second stage procedure bi-flap reconstruction of pinna was performed.
Pathological findings
Macroscopic examination: Specimen of skin covered irregular, bosselated greyish white large mass measuring 4 × 3× 1.5cm and smaller grey brown soft tissue bits measuring 1 x 1 x 0.4 cm. It is firm in consistency. External surface of the larger mass shows an ulcer measuring 0.5 x 0.5cm. with everted margins. The cut surface is grayish white with few circular homogenous areas and a small cyst filled with serous fluid [Table/Fig-1,2].
Gross specimen shows skin covered bosselated irregular ulerated greyish white large and small tumour masses

Cut section shows grey white homogenous and small cyst filled with serous fluid

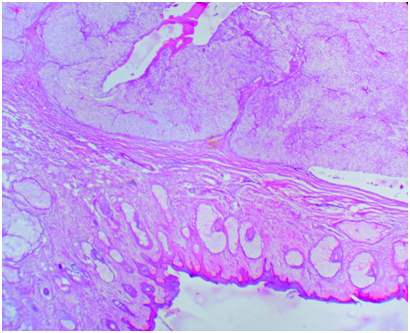
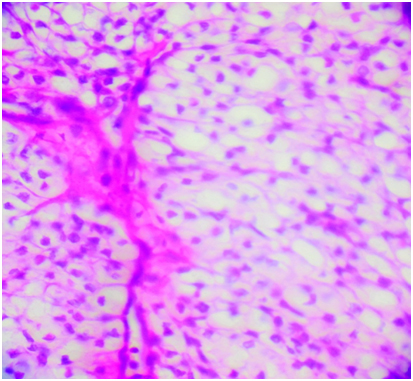
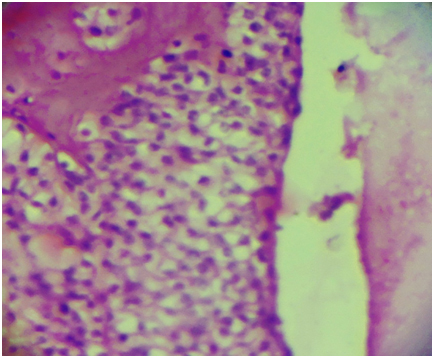
Histopathological examination: The tumour is well circumscribed and encapsulated; dermis showed tumour lobules composed of cellular masses separated by thin fibrous bands. Within the lobulated masses tubular lumina of various sizes were seen. In solid portion of the tumour, two types of cells could be recognized; one cell type is polyhedral with round or elongated nucleus and slightly basophilic cytoplasm. Another predominant cell type is usually round and contains very clear cytoplasm with small dark nucleus. Surface epidermis is free of the tumour component. Foci of hyalinized stroma were evident. Mitotic figures were rare and there was no necrosis. The histopathological diagnosis of clear cell hidradenoma was made in view of the above mentioned findings typical for this tumour [Table/Fig-3,4,5].
(50x) H & E Stain- Intact epidermis with multiple lobules of tumour component were seen in the dermis
(100x) H & E Stain- Hidradenoma, the tumour comprises clear and polygonal cells and small dark nucleus separated by thin fibrous septae
(100x) H & E Stain – lesional area shows foci of cystic change and hyalinized stroma
Discussion
Benign hidradenomas described in the literature at various names as, solid cystic hidradenoma, clear cell myoepithelioma, eccrine sweat gland adenoma, large cell hidradenoma and eccrine acrospiroma. Females were frequently affected when compared to males [1], they usually present as a single, small skin-coloured lesion, well demarcated, varies in size from 5-30mm in diameter [2]. Because of their controversial histogenesis, they cause diagnostic dilemma. They occur on any anatomical site, usually found on the scalp, face, anterior trunk and extremities [3]. Subcutaneously in various locations like eyelids, vulva, face, palmar aspect of the hand, and axillary tail of the breast [4]. These tumours found at any stage of life, lesions in children are very rare, but most common in the fourth decade [5]. Malignant transformation is very rare. Presence of malignant change is considered clinically by a rapid growth, cutaneous ulceration and pigmentation, histologically by an increased number of mitotic figures, nuclear atypia, angiolymphatic or perineural invasion and areas of necrosis [6]. Malignant lesions in the foot metastasizing to the skeleton were also reported in the literature [7]. When there is no evidence of invasive features but it has a high mitotic rate or nuclear atypia is labeled as atypical clear cell hidradenoma. To the best of our knowledge, the present case benign clear cell hidradenoma was not been reported over the ear lobule in the review of literature. Initially clinicians diagnosed as rodent ulcer and infected haemangioma on the basis of clinical examination. On histopathological examinations these tumours represent two types of cells, predominantly round cells with clear cytoplasm and polyhedral cells with rounded nucleus and slightly basophilic cytoplasm. The clear cells contain glycogen and Periodic Acid-Schiff-positive, diastase-resistant material, but no lipid. Focal cystic change also seen. Rarely some lesions show squamous differentiation [8], and malignant transformation [9]. Compared to benign lesions malignant lesions has more tendencies to invade local tissues, incidence of recurrence rate and distant metastasis were high [10]. Incomplete excision of the tumour leads to the recurrence [11]. Local recurrences were rare and surgical excision was treatment of choice [12]. However, there is no evidence of malignant transformation in this case as per the clinical and histopathological features. Being itself rare, a skin adnexal tumour located in the ear lobule is unusual. Histopathological examination plays an important diagnostic modality in these benign but unusual rare cases and awareness of the lesions is essential in their management.
Conclusion
Clear cell hidradenoma is a least common ear lobule tumour, and an uncommon site for these tumours. The possibility of sweat gland tumours should be considered in the differential diagnosis of ear louble tumours to ensure early detection and treatment. Histopathologic confirmation is necessary and wide excision of tumour is the treatment of choice.
[1]. Revis P, Chyu J, Medenica M, Multiple eccrinespir adenoma: case report and reviewJ Cutan Pathol 1988 15:226-29. [Google Scholar]
[2]. Thompson LDR, Nelson BL, Barnes EL, Ceruminous adenomas: a clinicopathologic study of 41 cases with review of the literatureAm J Surg Pathol 2004 28(3):308-18. [Google Scholar]
[3]. Winkelmann R, Wolff K, Solid- cystic hidradenoma of the skinArch Dermatol 1968 97:651-61. [Google Scholar]
[4]. Dina ED, Dean D, Alowami S, Clear cell hidradenoma: An unusual vulvar tumourInt J Gynecol Pathol 2008 27:457-60. [Google Scholar]
[5]. Devinder MT, Mummidi VR, Telanseri J, Changanti R, Ulcerated nodular hidradenomaIndian J Dermatol 1998 43:171-74. [Google Scholar]
[6]. Biddlestone LR, McLaren KM, Tidman MJ, Malignant hidradenoma : a case report demonstrating insidious histological and clinical progressionClin Exp. Dermatol 1991 16:474-77. [Google Scholar]
[7]. Ogilvie JW, Malignant eccrineacrospiroma. A case reportJ Bone Joint Surg Am 1982 64:780-82. [Google Scholar]
[8]. Stanley R, Sanchez N, Massa M, Cooper A, Ctotty C, Winkelmann R, Epidermoid hidradenomaJ Cutan Pathol 1982 9:293-302. [Google Scholar]
[9]. Hernandz E, Cestoni R, Nodular hidradenoma and hidradeno carcinomaJ Am AcadDermatol 1985 12:15-20. [Google Scholar]
[10]. Yildrim S, Akoz T, Apaydin I, Ege G, Gideroglu K, Malignant clear cell hidradenoma with giantmetastasis to the axillaAnn Plast Surg 2000 45:102 [Google Scholar]
[11]. Liapakis IE, Korkolis DP, Koutsoumbi A, Fida A, Kokkalis G, Vassilopoulos PP, Malignant hidradenoma: a report of two cases and review of the literatureAnticancer Res 2006 26(3B):2217-20. [Google Scholar]
[12]. Shaikh-Naidu N, Breitbart A, Eccrinespiradenoma of the upper extremity: case report and an algorithm for managementEur J Plast Surg 2003 26:160-63. [Google Scholar]