Bilateral Cystic Lymphangioma of Ovary Associated with Chylous Ascites
Savitri Mallikarjun Nerune1, Surekha Ulhas Arakeri2, Vijaya L. Patil3, Himanshu Dilip Mulay4
1 Assistant Professor, Department of Pathology, B.L.D.E.U’S Shri B.M. Patil Medical College Hospital and Research Centre, Vijayapur, Karnataka, India.
2 Professor, Department of Pathology, B.L.D.E.U’S Shri B.M. Patil Medical College Hospital and Research Centre, Vijayapur, Karnataka, India.
3 Professor, Department of Surgery, B.L.D.E.U’S Shri B.M. Patil Medical College Hospital and Research Centre, Vijayapur, Karnataka, India.
4 Postgraduate Student, Department of Pathology, B.L.D.E.U’S Shri B.M. Patil Medical College Hospital and Research Centre, Vijayapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Savitri Mallikarjun Nerune, Assistant Professor, Department of Pathology, BLDEU’S Shri B.M. Patil Medical College, Vijayapur 586103, Karnataka, India.
E-mail: saviraj31j@gmail.com
Intraabdominal cystic lymphangiomas are rare and are located in retroperitoneum, mesentery, omentum and other visceral organs. Lymphangiomas of the ovary are rare and are usually unilateral. Cases with bilateral cystic lymphangiomas of the ovary are reported very rarely in literature. We report a rare case of bilateral cystic lymphangioma of ovary associated with chylous ascites in a 35-year-old lady who presented with complaints of severe dysmenorrhoea and oligomenorrhoea since 6 months with history of chyluria for the past 3 years.
Chyluria, Dysmenorrhoea, Oligomenorrhoea
Case Report
A 35-year-old woman presented with complaints of severe dysmenorrhoea and oligomenorrhoea since 6 months. There was history of chyluria for the past 3 years. Ultrasound examination of abdomen and pelvis revealed bilateral tubo-ovarian mass with solid & cystic component suggestive of tuberculosis. Anti-tuberculosis treatment was given for 6 months but there was no response. Patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy. During surgery chylous ascitic fluid was drained and the specimen was sent for histopathological examination.
The specimen comprised uterus and cervix measuring 11×9×7 cm with bilateral adnexa. Uterus, cervix and both fallopian tubes were normal grossly. Both ovaries were enlarged in size, right ovary was 8×3×1 cm in size & left ovary measured 4×2×1.5 cm. External surface of both ovaries were pale white and nodular. Cut section was pale white, solid, with many cystic spaces varying in size from 0.5×0.5cm to 2×1 cm [Table/Fig-1]. Multiple sections were given from both ovaries and slides were stained with H&E, PAS and Alcian blue.
Gross photograph of cut surface showing spongy appearance with multiple cysts of varying sizes in bilateral ovaries

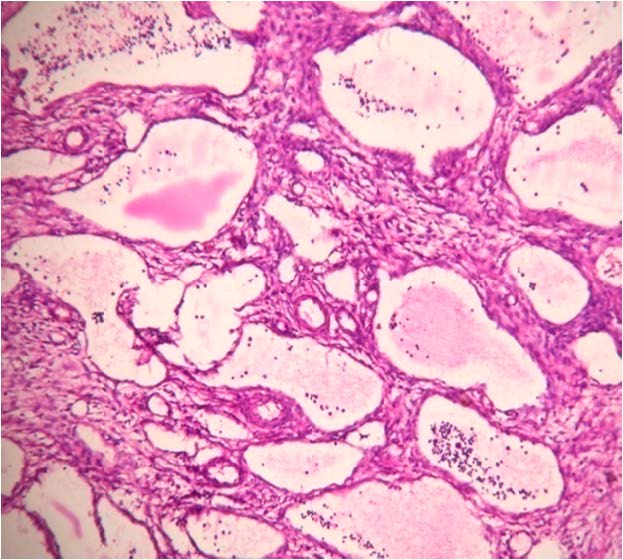
On microscopic examination cervix, endometrium, myometrium and both fallopian tubes were normal. Sections studied through both ovaries showed multiple cystic (lymphatic) spaces of varying sizes lined by flattened endothelial cells separated by thin fibrocollagenous septae. In some lymphatic spaces numerous lymphocytes & eosinophilic proteinaceous material was noted in the lumen [Table/Fig-2]. Intervening thin fibrocollagenous septae showed sparse mononuclear cell infiltration. Adjacent ovarian tissue showed cystic follicles and focal lymphocytic infiltration. PAS stain and alcian blue were negative [Table/Fig-3,4]. So, final diagnosis offered was bilateral cystic lymphangioma of ovary. On follow up for 3 months, there was mild chylous ascites with chyluria. Lipid profile was within normal limits.
Photomicrograph of ovary showing multiple irregular & variably sized vascular spaces lined by flattened endothelium, some of which show luminal lymphocytes & lymph (H&E 100X)
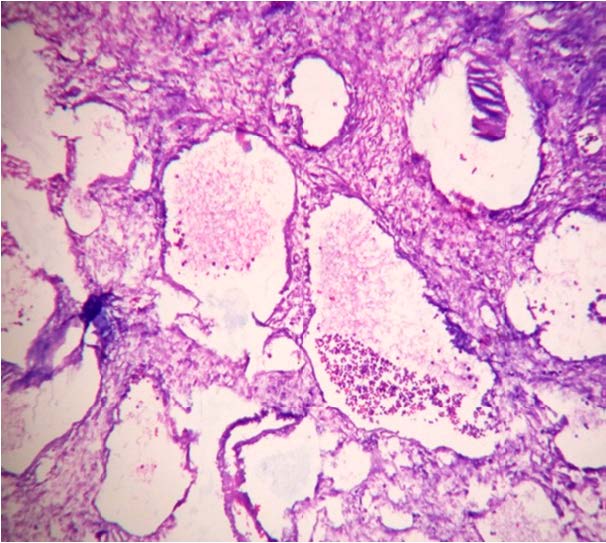
Photomicrograph of ovary showing negative staining with periodic-schiff stain (PAS 100X).
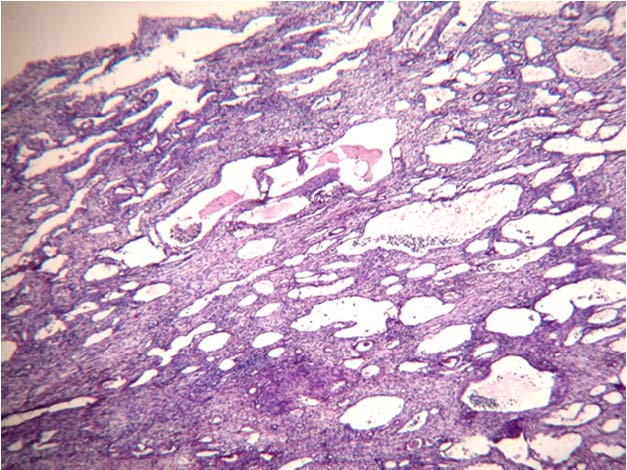
Photomicrograph of ovary showing negative staining with alcian blue (Alcian blue 40X)
Discussion
Lymphangiomas are rare malformations, which arise from sequestration of lymphatic tissue which fails to communicate with lymphatic system [1]. Morphologically they are comprised of multiple cystic spaces lined by single layer of flattened endothelium, containing serous or chylous fluid and are classified into capillary, cystic or cavernous type [2,3]. Lymphangiomas are most commonly seen in head, neck and axillary region but can occur anywhere in body [1]. They can also be seen in intestine, pancreas and mesentery [4].
Lymphatic system is formed by a network of unidirectional vessels that collects excess fluid from interstitial tissue, which is transported to the regional lymph nodes and ultimately drains to venous system through the thoracic duct. The lymphatic system is present in all organs except in the brain, anterior chamber of the eye, bone marrow and spleen [3].
Lymphangioma of the ovary is very rare and it was first described in 1908 [5]. As of now, around 20 cases have been reported in the literature [6]. Lymphangiomas are benign lesions characterised by proliferating lymphatic vessels and are common in head, neck and upper body regions. Intra-abdominal lymphangiomas are very rare which are mostly present in relation to the intestine and the mesentery [3]. Lymphangioma of the ovary is extremely rare, which is a usually unilateral, case with bilateral lymphangiomas have been reported very rarely in literature [3,6].
Pathogenesis of lymphangiomas is uncertain and matter of discussion. Some authors thought they are true neoplasms [5]. According to well established theory, sequestration of lymphatic tissue during embryonic development can cause lymphangiomas [7]. Various authors thought that impaired regional lymphatic drainage due to chronic salphingitis or radiation therapy may be the cause for cystic lymphangioma of ovary [5]. In present case there was no evidence of chronic salphingitis on microscopy and there was no history of radiation therapy, patients follow up for 3 months showed mild chylous ascites and chyluria, so in the present case sequestration of lymphatic tissue during embryonic development or neoplastic nature may be possible pathogenic mechanism.
Size and location of lymphangiomas are the determinants of clinical presentations which can vary from an asymptomatic state to acute onset of severe abdominal pain [8]. Abdominal pain and distension are the most common symptoms of the intra-abdominal lymphangiomas. Other presentations like compression symptoms, rupture, secondary infection, volvulus or intestinal obstruction have also been reported [8]. In the present case patient presented with complaints of severe dysmenorrhoea, oligomenorrhoea, history of chyluria and chylous ascites. Literature search revealed clinical presentation of cystic lymphangioma of ovary accompanied by chylous ascites is very rare. In a study done by Takeshi Iawasa et al., [5] unilateral lymphangioma of the ovary was associated with chylous ascites. In present case cystic lymphangioma was bilateral and was associated with chylous ascites and chyluria which is rare presentation.
USG evaluation is the first step in diagnosis. A cystic lesion with multiple thin septa is the typical USG finding of lymphangioma [8]. In our case, USG showed bilateral tubo-ovarian mass which was solid and cystic in nature. So, tuberculosis was suspected and anti-tuberculosis therapy was started. CT scan and MRI can also be utilised. MRI is more useful than CT scan for detecting fluid filled cystic lesions [1,8].
The main differential diagnosis for lymphangioma of ovary is an adenomatoid tumour and haemangioma of the ovary. Adenomatoid tumour of the ovary is a benign solid tumour of mesothelial origin affecting female genital tracts. Adenomatoid tumour stains positive with PAS and Alcian blue while lymphangiomas do not stain [4]. In the present case PAS and Alcian blue stains were negative and cystic spaces were filled with lymphocytes hence we have concluded this case as cystic lymphangioma. Another differential diagnosis includes haemangioma which unlike lymphangioma, contains RBCs within the vascular spaces [4].
The gold standard treatment modality of cystic lymphangiomas is surgical excision [1,5]. Laparoscopic excision can be done. It carries excellent prognosis. It has advantages over conventional surgical excision like less intraoperative blood loss, early recovery, less morbidity and fewer complications [1]. Few authors suggest conservative management of asymptomatic cystic lymphangiomas due to spontaneous regression rate of 10%. Other treatment options include aspiration and injection of sclerosant agents, OK-432, steroids, bleomycin, fibrin glue or ethibloc which are not been established superior to surgery [8].
Conclusion
Ovarian lymphangiomas are rare cystic lesions of ovary and should be considered as a differential diagnosis of ovarian cystic masses. This lesion is often missed radiologically hence histopathological examination is must for the diagnosis of this lesion.
[1]. Karkera PJ, Sandlas GR, Ranjan RR, Kesan K, Gupta AR, Gupta RK, Intra-abdominal cystic lymphangiomas in children: A Case SeriesArchives of International Surgery 2012 2:91-95. [Google Scholar]
[2]. Naik SA, Rare case of ovarian cystic lymphangioma managed at laparoscopyJ Gynaecol Endo Surg 2011 2:97-100. [Google Scholar]
[3]. Kafeel G, Telisinghe PU, Hla OO, Lymphangioma of the OvaryBrunei Int Med J 2010 6:145-48. [Google Scholar]
[4]. Bavikar RR, Tampi C, Lymphangioma of OvaryBombay Hosp J 2011 53:89-91. [Google Scholar]
[5]. Iwasa T, Tani A, Miyatani Y, Bekku S, Yamashita M, Nakanishi K, Fujii Y, Lymphangioma of the ovary accompanied by chylous ascitesJ Obstet Gynaecol Res 2009 35:812-15. [Google Scholar]
[6]. Pillai S, O’Brien D, Stewart CJR, Bilateral ovarian lymphangioma (lymphangioleiomyoma)Int J Gyneacol Pathol 2013 32:171-75. [Google Scholar]
[7]. Rieker RJ, Quentmeier A, Weiss C, Kretzschmar U, Amann K, Mechtersheimer G, Cystic lymphangioma of the small-bowel mesentery. Case report and a review of the literaturePathology Oncology Research 2000 6:146-48. [Google Scholar]
[8]. Yildiz C, Karadayi K, Sarkis C, Cetin A, Huge cystic lymphangioma mimicking ovarian malignancy: a case reportTurk J Gastroenterol 2011 22:344-46. [Google Scholar]