In recent years, coagulase negative staphylococci (CoNS) have emerged as important causative agents of nosocomial and community acquired infections [1]. Methicillin-resistant CoNS (MR-CoNS), most notably S. epidermidis, S. haemolyticus, S. hominis are major MR-CoNS and the main colonizers of the anterior nares and human skin [2]. Methicillin-resistant staphylococcal strains have acquired and integrated into their genome the staphylococcal cassette chromosome mec (SCCmec), which carries the methicillin resistance (mecA) gene, and other antibiotic resistance determinants [3].
Antimicrobial resistance is recognized as a substantial problem for a number of community-acquired infectious diseases. In the vast majority of staphylococcal isolates, resistance to macrolides such as erythromycin resistance in CoNS is mediated by the erm(A), erm(C) and msrA genes [6,7]. Tetracycline resistance, encoded by tetK and tetM gene, mediates active efflux and reduces the sensitivity of the ribosome to the drug respectively [6]. Aminoglycoside resistance is attributed to drug inactivation caused by aminoglycoside modifying enzymes (AMEs) encoded within mobile genetic elements. The most frequent AMEs are the bifunctional enzyme AAC(6′)/APH(2′) encoded by the gene aac (6′)-Ie-aph(2′)-Ia, APH(3′)-III enzyme encoded by aph(3′)-IIIa gene and ANT(4′)-I enzyme encoded by ant(4′)-Ia gene [8].
Mupirocin resistance occurs in two phenotypes: low- level and high- level resistance. The high-level resistant strains contained the ileS-2 gene, which encodes a novel staphylococcal isoleucyl-tRNA synthetase. While, low level mupirocin-resistant CoNS contained the mutation V588F, located near the conserved motif KMSKS, within the chromosomal staphylococcal isoleucyl-tRNA synthetase gene (ileS) [9]. Plasmid mediated fusidic acid resistance has also been described and genes encoding proteins that play a protective role in Elongation Factor-G were recently identified. The genes encoding these proteins are known as fusB, fusC and fusD [10].
The accurate and rapid diagnosis of antibiotic resistance genes in staphylococcal carriage is extremely important in preventing the spread of bacterial infections from nasal carriage to bloodstream and has been considered as the potential source of bacterial invasion. There is no Indian study on the distribution of SCCmec types and various antibiotic resistant genes among nasal isolates from healthy individuals. Hence, the present study was designed to find the distribution of SCCmec and the various antibiotic resistance genes amongst MR-CoNS isolates from community settings in Chennai, South India.
Materials and Methods
(a) Nasal Swabs from Community Settings
A total of 145 nasal swabs were collected from asymptomatic individuals during November 2013- February 2014 from orphanages and old age homes in and around Chennai. The asymptomatic individuals did not take any antibiotics and had no contact with the hospital in the three months prior to sampling and were considered to be community carriers. This study was approved by institutional Human ethical committee.
The anterior nasal swabs were collected using sterile Hi Culture collection cotton swabs (HiMedia) and transported immediately to the laboratory. The nasal swabs were enriched with 7.5% salt nutrient broth at 37°C for 24 h and sub-cultured onto blood agar and MacConkey agar.
Bacterial isolates obtained were identified by colony morphology, Gram staining and biochemical reactions. All CoNS isolates (catalase-positive, tube coagulase-negative, Gram-positive cocci) were further analysed.
(b) Identification of CoNS Isolates
Speciation of CoNS isolates was done by the standard biochemical tests which include Alkaline phosphatase test, haemolysis on blood agar, Urease test, Sugar fermentation (mannitol, sucrose, maltose, mannose, trehalose), polymixin B & novobiocin susceptibility [11]. S. epidermidis and S. haemolyticus were further confirmed by species specific PCR by using S. epidermidis specific PCR fragment and mvaA genes respectively [12].
(c) Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was done for the following antibiotics using Kirby-Bauer disc diffusion method according to the Clinical and Laboratory Standards Institute (CLSI) 2012 guidelines [13]. The following antimicrobial agents (HiMedia) were tested: amikacin (30μg), ciprofloxacin (5μg), clindamycin (2μg), co-trimoxazole (1.25/23.75μg), erythromycin (15μg), fusidic acid (30μg), gentamicin (10μg), linezolid (30μg), mupirocin (5 & 200μg), ofloxacin (5μg), rifampicin (5μg), tetracycline (30μg), tobramycin (10μg) and vancomycin (30μg). S. aureus ATCC 25923 and S. epidermidis ATCC 12228 were used as control strains.
The inducible phenotype was characterized by a positive D test, a flattening of the inhibition zone around the clindamycin disc near the erythromycin disk indicated inducible clindamycin resistance (iMLSB). The phenotype cMLSB was characterized by erythromycin and clindamycin resistance. The zones of inhibition were interpreted according to the CLSI guidelines 2012.
(d) DNA extraction – Boiling lysis Method
DNA extraction was done by the modified method of Abimanyu et al., [14]. Few bacterial colonies were suspended in 300μl of DNase free water (Qiagen) and kept in dry bath (Labnet) for 10 min, kept in freezer (-20°C) overnight. The suspension was then centrifuged at 6000 rpm for 5 min. Two microlitres of the supernatant was used as template for PCR.
(e) Screening of Methicillin resistance by Phenotypic and genotypic Methods
Methicillin resistance was screened by using cefoxitin (30μg) disc diffusion method and Multiplex PCR (M-PCR) was performed for the simultaneous detection and differentiation of MRSA from MR- CoNS [14]. S. aureus ATCC 43300 and S. epidermidis RP62A were used as positive control.
(f) PCR Screening of Antibiotic resistant determinants
Antibiotic resistant determinants of conventional and newer antibiotics viz., erm(A), erm(C), tetK, tetM, msrA, dfrA, aac(6′)-Ie-aph(2′)-Ia, aph(3′)- IIIa, ant(6)-Ia, ant(4′)-Ia genes were detected by previously described method [6,7,8]. Mupirocin resistant (mupA) gene and fusidic acid resistant (fusB, fusC & fusD) genes were determined by the method of Yun et al., and Castanheira et al., [9,10] respectively [Table/Fig-1].
Primers and their sequences for various antibiotic resistance encoding genes used in this study
| Target genes | Primer sequences | Product (bp) | Annealing temper-ature (°C) | Reference |
|---|
| mecA | F: TGCTATCCACCCTCAAACAGG | 286 | 54.5 | Abimanyu et al.,[14] |
| R: AACGTTGTAACCACCCCAAGA |
| femA | F: AAAAAAGCACATAACAAGCG | 132 |
| R: GATAAAGAAGAAACCAGCAG |
| erm (A) | F: AAGCGGTAAACCCCTCTGA | 190 | 55 | Strom-menger et al., [6] |
| R: TTCGCAAATCCCTTCTCAAC |
| erm (C) | F: AATCGTCAATTCCTGCATGT | 299 |
| R: TAATCGTGGAATACGGGTTTG |
| tetK | F: GTAGCGACAATAGGTAATAGT | 360 |
| R: GTAGTGACAATAAACCTCCTA |
| tetM | F: AGTGGAGCGATTACAGAA | 158 |
| R: CATATGTCCTGGCGTGTCTA |
| msrA | F: GAAGCACTTGAGCGTTCT | 287 | 50 | Shittu et al., [7] |
| R: CCTTGTATCGTGTGATGT |
| dfrA | F: CTCACGATAAACAAAGAGTCA | 201 |
| R: CAATCATTGCTTCGTATAACG |
| aac(6′)-Ie aph(2″) | F: CATTATACAGAGCCTTGGGA | 279 | 57 | Ida et al., [8] |
| R: AGGTTCTCGTTATTCCCGTA |
| ant(4′)-Ia | F: ATGGCTCTCTTGGTCGTCAG | 367 |
| R: TAAGCACACGTTCCTGGCTG |
| aph(3′)-IIIa | F: CGATGTGGATTGCGAAAACT | 175 |
| R: CACCGAAATAACTAGAACCC |
| fusB | F: TCATATAGATGACGATATTG | 496 | 53 | Castanheira et al., [10] |
| R: ACAATGAATGCTATCTCGAC |
| fusC | F: GATATTGATATCTCGGACTT | 128 |
| R: AGTTGACTTGATGAAGGTAT |
| fusD | R: TGCTTATAATTCGGTCAACG | 525 |
| R: TGGTTACATAATGTGCTATC |
| mupA | F: TATATTATGCGATGGAAGGTTGGR: AATAAAATCAGCTGGAAAGTGTTG | 456 | 57 | Yun et al., [9] |
All the PCR reactions were carried out Initial Denaturation:94°C- 4 minutes, Denaturation: 94°C- 1 minute, Annealing - refer table 1, Extension: 72°C- 1minute, Final extension 72°C- 7minutes.
(g) Detection of SCCmec types and sub typing of SCCmec type IV
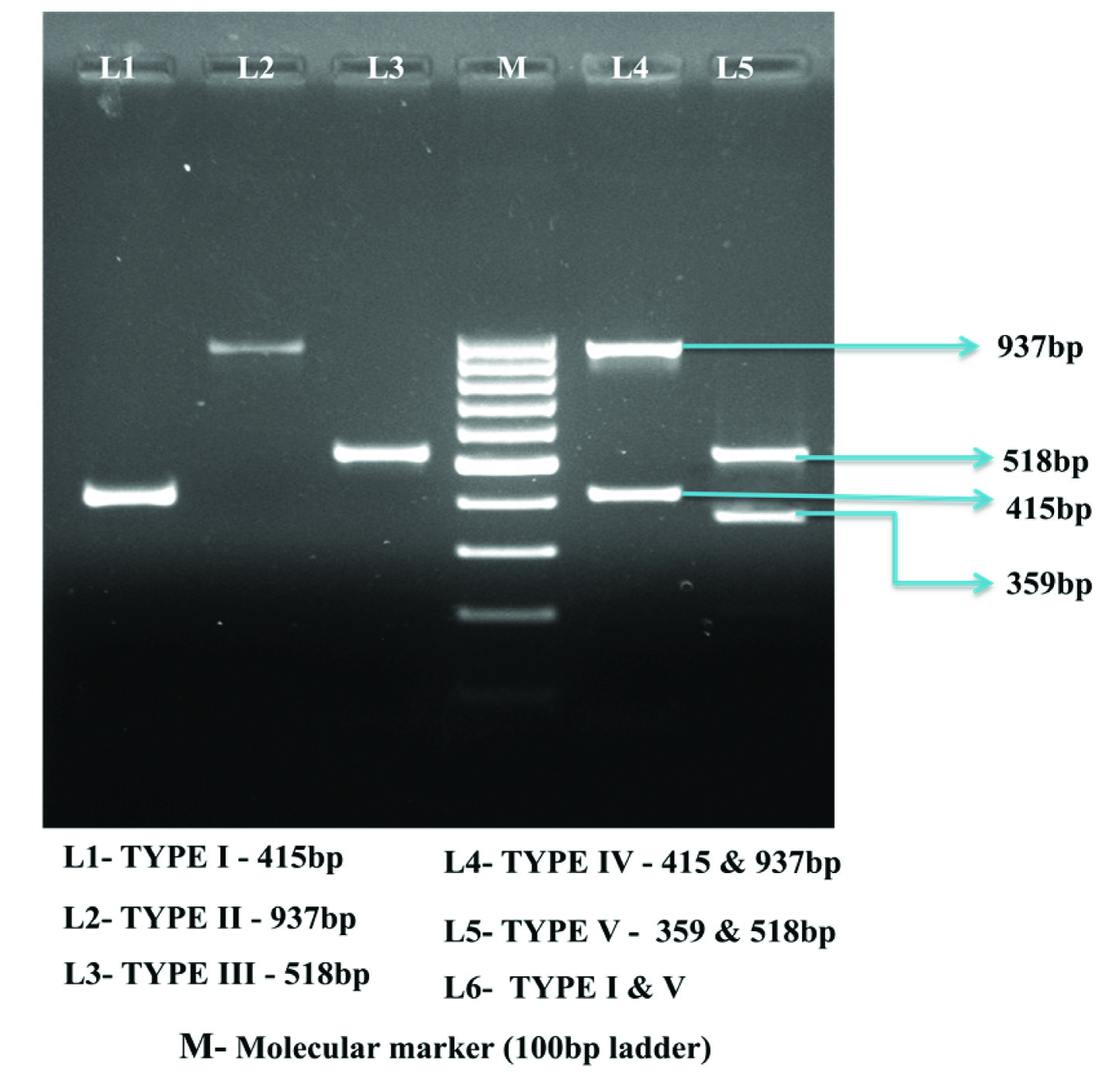
SCCmec typing (type I- V) was done by using M-PCR [15]. Positive control strains used in the determination of the SCCmec type were the MRSA strains COL- SCCmec type I, Mu50- SCCmec type II, SCCmec type III- ANS46, SCCmec type IV- MW2, SCCmec type V- WIS. SCCmec IV subtypes (IVa, IVb/IVF, IVc/IVE, IVd, IVg, IVh) were determined by M-PCR with primers described by Milheirico et al., [4]. SCCmec IV subtype was described as “ND” when the PCR amplicon was not detected.
Results
Among 145 nasal swabs from closed community settings, 50 (44.6%) non-duplicate isolates were found to be methicillin resistant by phenotypic & genotypic method. Among Species identified S. epidermidis (n= 20, 40%) was the predominant species followed by S. haemolyticus (n= 14, 28%), S. hominis (n= 10, 20%) and S. warneri (n= 6, 12%).
Antimicrobial Susceptibility Testing
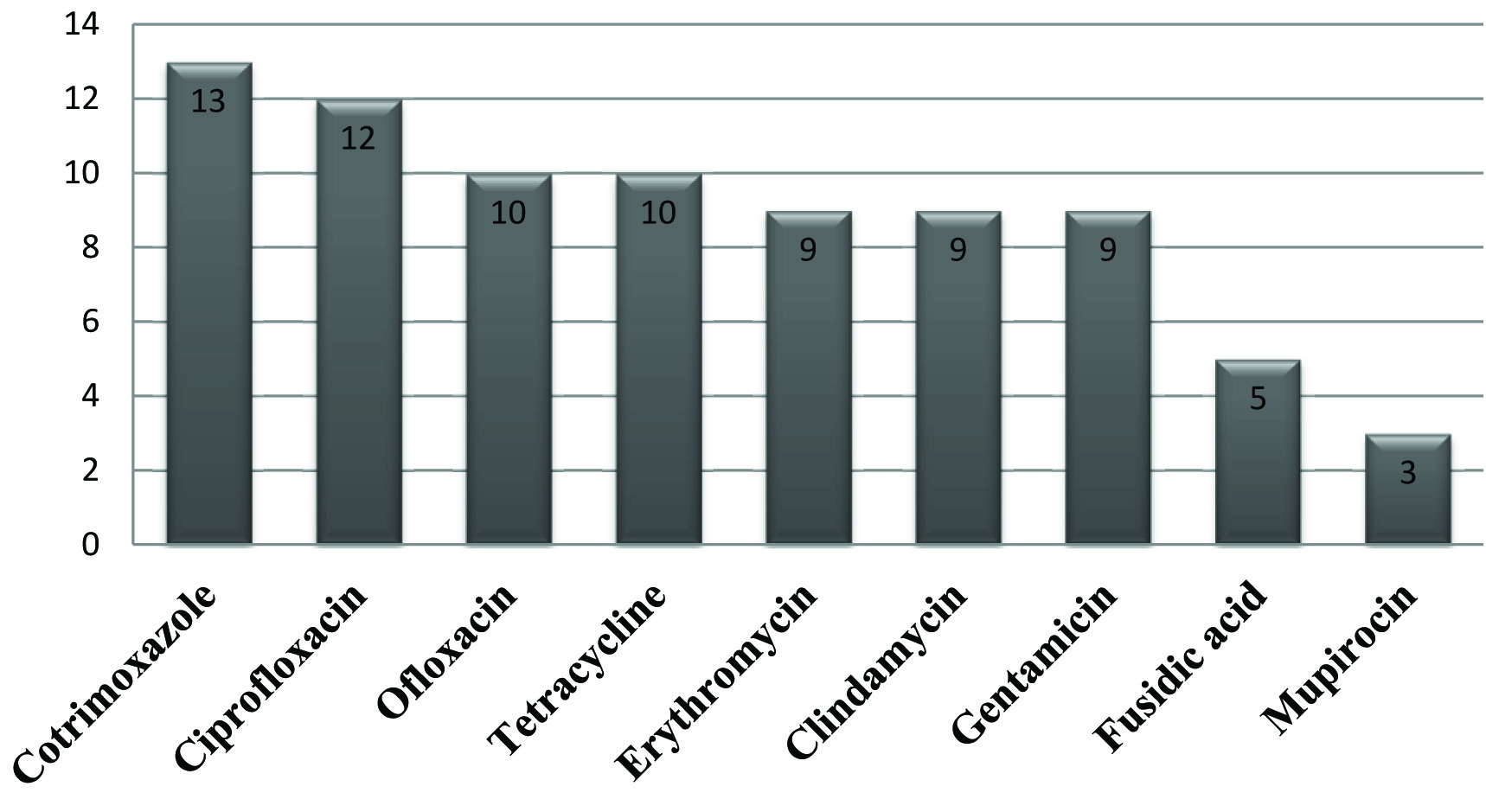
Among the antibiotics tested, highest resistance was seen for cotrimoxazole (n= 13, 26%), followed by ciprofloxacin (n= 12, 24%), ofloxacin(n= 10, 20%), tetracycline (n= 10, 20%), gentamicin (n= 9, 18%) and erythromycin (n= 9, 18%). Low level resistance was seen for fusidic acid (n= 5, 10%) and mupirocin (n= 3, 6%). Amongst the erythromycin resistant isolates, 7 (77.8%) isolates and 2 (22.2%) isolates were found to be positive for iMLSB and cMLSB phenotype respectively. All MR-CoNS isolates included in our study were susceptible to amikacin, rifampicin, vancomycin and linezolid [Table/Fig-2].
Antibiotic resistant pattern of MR-CoNS isolates from community settings
Detection of Resistance Genes among MR-CoNS
Complete correlation between phenotypes and genotypic traits of resistance to the antibiotics was found. All the 13 (26%) cotrimoxazole resistant isolates were positive for dfrA gene, Among the 10 (20%) tetracycline resistant isolates, all the isolates harbored tetK gene. The aac(6′)-Ie-aph(2′)-Ia was the most prevalent gene among aminoglycoside-resistant isolates, detected alone in 6 (67%%) isolates and in combination with aph(3′)-IIIa 3 (33%) among the remaining isolates. Among the 5 (10%) fusidic acid resistant isolates, (n=3) isolates carried fusB and 2 isolates harboured fusC gene. All the three mupirocin resistant isolates were positive for mupA gene. Among the 9 (18%) erythromycin resistant isolates, 7 isolates (77.8%) harbored ermC gene and 2 isolates (22.2%) carried the ermA gene.
Diversity of SCCmec elementsamong MR-CoNS
A high genetic diversity of SCCmec was observed. Of the 50 MR-CoNS studied, 44 isolates showed single type, including type I (n=15, 30%), type IV (n=12, 24%), type II (n= 9, 18%), type V (n=7, 14%) and type III (n=1, 2%). 6 isolates had two types, III+IV (n= 2, 4%), II+V (n=2, 4%), IV+V (n=1, 2%) and type I+V (n=1, 2%). Subtypes of type IV (n=12) isolates showed IVA (n=6/12, 50%), IVG (n=2/12, 16.7%) and 4/12 isolates(33.3%) showed ND [Table/Fig-3,4].
Distribution of SCCmec types among nasal carriage of methicillin resistant coagulase negative staphylococci (MR- CoNS)
| SCCmec types | S. epidermidis | S. haemolyticus | S. hominis | S. warneri | Total (%) |
|---|
| Type I | 0 | 8 | 4 | 3 | 15 (30) |
| Type II | 4 | 3 | 2 | 0 | 9 (18) |
| Type III | 1 | 0 | 0 | 0 | 1 (2) |
| Type IV | 7 | 2 | 2 | 1 | 12 (24) |
| Type V | 3 | 1 | 1 | 2 | 7 (14) |
| Type I + V | 1 | 0 | 0 | 0 | 1 (2) |
| Type II + V | 2 | 0 | 0 | 0 | 2 (4) |
| Type III + IV | 1 | 0 | 1 | 0 | 2 (4) |
| Type IV + V | 1 | 0 | 0 | 0 | 1 (2) |
| Total | 20 | 14 | 10 | 6 | 50 |
Multiplex PCR for SCCmec Typing among MR-CoNS
Antibiotic Resistant Genes and Its Associated SCCmec Types
The overall resistance to non β-lactam antibiotics was more common in SCCmec type I positive isolates. One isolate of SCCmec type III was found to be resistant to non-β-lactam antibiotics and harbouring combination of resistant genes tested [Table/Fig-5].
Analysis of antibiotic resistance genes and its associated SCCmec types
| SCCmec Types | Antibiotic Resistant Determinants |
|---|
| aac (6′)-Ie-aph(2′)-Ia | aph(3′)-IIIa | tetK | erm(A) | erm(C) | dfrA | mupA | fusB | fusC |
|---|
| Type I (15) | 4 (26.7%) | 2 (13.3%) | 3 (20%) | 0 (0) | 3 (20%) | 3 (20%) | 0 | 1 (6.7%) | 1 (6.7%) |
| Type II (9) | 0 (0) | 0 (0) | 2 (22.2%) | 0 (0) | 1(11.1%) | 0 | 1 (11.1%) | 0 (0) | 1 (11.1%) |
| Type III (1) | 1 (100%) | 1 (100%) | 1 (100%) | 0 (0) | 1 (100%) | 1 (100%) | 1 (100%) | 0 (0) | 0 (0) |
| Type IV (12) | 0 (0) | 0 (0) | 2 (16.7%) | 0 (0) | 2 (16.7%) | 4 (33.3%) | 1 (8.3%) | 1 (8.3%) | 0 (0) |
| Type V (7) | 1 (14.3%) | 0 (0) | 1 (14.3%) | 1 (14.3%) | 0 | 3 (42.8%) | 0 | 0 (0) | 0 (0) |
| Combinations (6) | 0 (0) | 0 (0) | 1(16.6%) | 1 (16.6%) | 0 | 2 (33.3%) | 0 | 1 (16.6%) | 0 (0) |
| Total | 6 | 3 | 10 | 2 | 7 | 13 | 3 | 3 | 2 |
Discussion
Worldwide, there are several reports in the recent past on the spread of MR-CoNS out of the hospital setting into the community [2,16]. But, in India there is a paucity of data regarding diversity of SCCmec types and antibiotic resistant genes among MR-CoNS from community settings.
Prevalence of MR-CoNS carriage was 44.6% which was significantly higher than previous studies [2]. The impact of antibiotic selective pressure might possibly explain the high prevalence of MR-CoNS carriage. Among the MR-CoNS isolates, S. epidermidis (n= 20/50, 40%) was the predominant species followed by S. haemolyticus (n= 14/50, 28%), S. hominis (n= 10/50, 20%) and S. warneri (n= 6/50, 12%) which was consistent with previous reports [2,17].
The MR-CoNS isolates were analyzed for the (dfrA) gene, 13(26%) isolates were positive for dfrA gene. Among the genes encoding aminoglycoside resistance, aac(6′)- Ie-aph (2′)-Ia (67%) was the most prevalent AME gene which was in agreement with the other previous studies [18–20]. Among tetK and tetM genes- tetK (20%) gene alone was detected, whereas tetM was not found in any of the isolates unlike previous reports in which both tetK and tetM genes were found [18–20].
Among mupA and fusB, fusC, fusD resistant genes tested, three (6%) isolates were mupA positive and 5 isolates (10%) showed the fusidic acid resistant genes in which, fusB was the most prevalent gene followed by fusC gene. This finding was supported by previous reports [10,21]. In India, fusidic acid and mupirocin resistant genes were not detected among MR-CoNS isolates. Among erm(A), erm(C) and msrA, 18% of isolates showed erythromycin resistant genes of which erm(C) gene was the most prevalent gene which was supported by previous studies [19,22].
The SCCmec element is a mobile genetic element widely distributed among MR-CoNS species which varies depending on the host species, various environments and geographical locations. The SCCmec types among MR-CoNS were type I (15/50, 30%) followed by type IV (12/50, 24%), type II (9/50, 18%), type V (7/50, 14%) and type III (1/50, 2%). Six (12%) isolates were found to be of two types of SCCmec. As described previously, the diverse SCCmec type profile among CoNS strains, is due to the higher capacity of genetic transferability between the species [16,18,20].
A strong association was observed between multidrug resistance and the presence of SCCmec type I and type III. These two SCCmec types were found to show high percentage of resistance to non-β- lactam antibiotics harbouring combination of resistant genes tested. According to the literature, isolates containing SCCmec type III contain a large number of resistance genes [17,18]. In this study, overall resistance to non-β-lactam antibiotics was more common in SCCmec type I positive isolates (probably due to the significantly higher proportion of isolates with SCCmec type I than type III). Although SCCmec IV is not associated with multi-resistant isolates, in this study, a few isolates harbored (dfrA n= 4, ermC n= 2, tetK n= 2, mupA n= 1and fusB n= 1) multidrug resistance indicating the existence of multidrug- resistant SCCmec IV isolates.
Among S. epidermidis, great diversity of SCCmec was found, type IV (7/12), type II (4/9), type V (3/7), type III (1/1) and two types II+V (2/2), III+IV (1/1), I+V (1/1) & IV+ V (1/1). Of the 7 isolates carrying SCCmec type IV, 4 isolates carried subtype IVa and 2 carried subtype IVg and one isolate showed “ND” which was in agreement with the previous studies [16]. The high number of different SCCmec types present in S.epidermidis, together with those present in other MR-CoNS may build up a large reservoirof new SCCmec types for S.aureus probably facilitating horizontal transmission between Staphylococcus species. Although there is no experimental evidence, many studies have supported the hypothesis of MR-CoNS acting as a reservoir for diverse SCCmec elements among S. aureus [2,5,16,17,20].
Two types of SCCmec elements were found in S. epidermidis (n= 6, 12%) and S. hominis (n= 5, 10%) isolates. This is no surprise as the co-existence of two SCCmec elements appears to be common in MR-CoNS which strongly suggests that new variants may be present in CoNS and may have a different impact on drug resistance. Due to the various combinations of different SCCmec types in the CoNS observed here and reported by others [5,23,24], there is a clear need to develop a unique typing system for CoNS.
Conclusion
The species identification of MR-CoNS could help in determining the contribution of each species to antibiotic resistance and SCCmec types in the community and help in designing effective surveillance and control strategies. This study highlights the high carriage rate of MR-CoNS in the community and further provides evidence of their role as facilitator for genetic diversity of SCCmec in this setting.