Large Cervical Paraspinal Haemangioma in Association with Intraosseous Haemangioma: A Rare Case Report
Hanish Bansal1, Ashwani Kumar Chaudhary2, Anuj Mahajan3
1 Assistant Professor, Department of Neurosurgery, Dayanand Medical College and Hospital, Ludhiana, India.
2 Professor, Department of Neurosurgery, Dayanand Medical College and Hospital, Ludhiana, India.
3 Resident, Department of Surgery, Dayanand Medical College and Hospital, Ludhiana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hanish Bansal, 10-B, Udham Singh Nagar, Ludhiana, Punjab-141001, India. E-mail : y2khanish@gmail.com
Haemangiomas are most commonly found in skin and subcutaneous tissue and are very rare in intramuscular region. Paraspinal musculature has been barely reported as location of intramuscular haemangioma while we could not find any literature reporting haemangioma in cervical paraspinal previously. We report a case of middle aged woman with a large intamuscular haemangioma involving left cervical paraspinal musculature extending from suboccipital region to C5 vertebra and reaching upto left parotid gland along with C6 vertebral body haemangioma.
Benign, Intramuscular, Masseter
Case Report
A 52-year-old female presented to the Department of Neurosurgery with complaints of pain and heaviness in posterior neck for last one month. Patient gave history of surgical excision of mass from posterior part of neck around 20 years back but exact details of the pathology and the procedure were not available. According to the patient, she was asymptomatic during this period and had noticed pain recently since one month. Skin over posterior neck revealed multiple small patches of cutaneous haemangiomas besides horizontal scar mark about 6 cms in size over nape of neck [Table/Fig-1]. The patient first noticed these 10 years back and these had not increased in size since then. Rest of general physical examination and systemic examination was within normal limit. MRI revealed haemangioma approximately 11×7.9×7.0 cm in size in posterior neck extending from suboccipital region to C5 level in middle and left side [Table/Fig-2].
Horizontal scar mark along with purple patches of skin discoloration

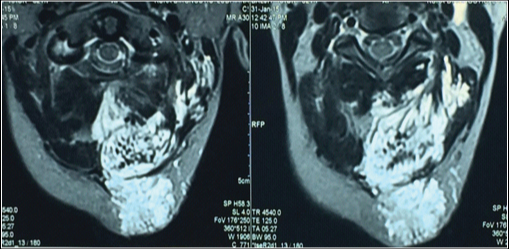
MRI shows vertical extension of Haemangioma

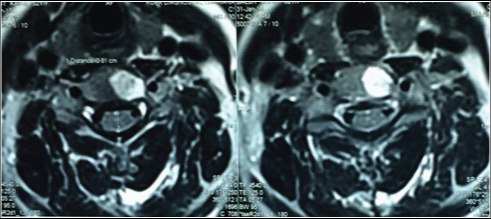
The Haemangioma involved paraspinal muscles and occipital bone and reached near posterior elements of C2 vertebra body and left parotid gland [Table/Fig-3]. MRI also revealed haemangioma in C6 vertebral body and another smaller lesion in left parapharyngeal space abutting larynx [Table/Fig-4]. In view of the clinical appearance and such an invasive growth of the lesion, an angiography was planned preoperatively. But patient was lost to follow up.
MRI shows involvement of cervical paraspinal muscles
MRI depicting C6 vertebral body Haemangioma
Discussion
Intramuscular Haemangiomas are very rare and account for less than 1% of all haemangiomas [1]. Trunk and lower limbs are two most common sites for intramuscular haemangioma. Less than 20% of these are found in the head and neck area with most common muscles involved in order of frequency being masseter muscle, trapezius, periorbital, sternocleidomastoid and temporalis muscle. Less frequently involved muscles include tongue, extra ocular and posterior neck muscles [2].
Paraspinous haemangiomas have been barely mentioned in the literature. Swaroop et al., reported a case of 29-year-old female with lumbar paraspinal Haemangioma for which surgical excision was done [3]. Makeieff et al., reported a case of 39-years-old female with Haemangioma of splenius capitis muscle which was surgically excised [4]. Cervical paraspinal haemangioma in association with intraosseous haemangioma (C6 vertebral body) has not been reported previously in medical literature. Intramuscular haemangioma occurs most common in the third and forth decades of life, in contrast to cutaneous haemangiomas which occur during infancy [5]. Eighty percent of Haemangiomas are solitary while 20% of affected patients may have multiple tumours [6].
They are non metastasizing benign congenital tumours that may present as palpable, fluctuant or firm mass in upto 98% of cases [7]. Vascular signs such as thrill or skin discoloration that are characteristic of superficial haemangiomas are usually absent in intramuscular haemangiomas. Phleboliths (calcified nodules) regarded as characteristic property of venous or cavernous haemangiomas are usually absent in haemangioma in head and neck region. Intramuscular haemangiomas are generally poorly encapsulated and have the ability to infiltrate adjacent muscles. These parapsinalhaemangiomas may rarely extend upto epidural space and may cause neurological sequelae or epidural haematoma. Shima et al., reported a case of angioma in the paraspinal muscles with extension into the epidural tissue complicated by epidural Haematoma in the thoracolumbar region [8].
Intramuscular haemangioma in contrast to infantile cutaneous haemangioma do not regress spontaneously, and are relatively insensitive to systemic corticosteroid therapy [9]. Growth spurt or trauma may accelerate growth of haemangioma. Haemangiomas may be classified histopathologically into capillary and cavernous types or according to the size of the vessels into small vessels or capillary type, large-vessel or cavernous type and into mixed type. Magnetic Resonance Imaging (standard imaging technique for evaluation of soft tissue Haemangiomas) findings include a focal, lobulated soft-tissue mass that is isointense relative to muscle on T1-weighted images and hyperintense on T2-weighted images [10]. In cases where vascular feeder needs to be delineated for embolization, angiography is helpful [11]. Preoperative embolization of haemangiomas before surgery helps to decrease intraoperative blood loss. Cohen et al., reported two cases of intramuscular hemngioma of paraspinous muscles treated with arteriographic embolization followed by immediate local excision [12].
Various treatment options recommended for intramuscular haemangiomas include surgery, sclerosing agents, cryotherapy, steroid administration, blood vessel ligation and embolisation. However, to prevent recurrence wide local excision that includes normal muscle beyond the gross limits of the tumour is the optimal management. Partial excision is associated with an 18% recurrence rate [13]. Lesions that are highly localized well circumscribed single-muscle, and have minimal loculations have better surgical outcomes. Our case was probably a case of incomplete excision leaving a large residual/recurrent lesion in cervical paraspinal region. The indication for surgery includes sudden rapid acceleration of tumour size, gross functional impairment, local skin necrosis, thrombocytopenia, cosmetic deformity and suspicion of malignancy [14].
Conclusion
Intramuscular haemangiomas are very rare and paraspinal involvement being even rarer. We report a very rare case of large cervical paraspinal Haemangioma extending from suboccipital region to C5 vertebra and reaching up to left parotid gland in association with C6 vertebral body haemangioma. Complete surgical excision with a cuff of normal tissue remains treatment of choice. Preoperative angiography with selective embolization helps in reducing intraoperative blood loss. Partial excision is associated with high recurrence rate.
[1]. Mohamad I, Soleh MN, Rahman KSA, Sharif SET, Intramuscular sternohyoid haemangioma: an unusual neck massMed J Malaysia 2013 68(2):166-67. [Google Scholar]
[2]. Nayak S, Shenoy A, Intra-muscular haemangioma: a reviewJ Orofac Sci 2014 6:2-4. [Google Scholar]
[3]. Swaroop A, Chaudhury S, Chakraverty U, Singh D, Lumbar para-spinal haemangioma as a rare differential diagnosis of lumbar disc prolapseThe Internet Journal of Orthopedic Surgery 2008 11(1) [Google Scholar]
[4]. Makeieff M, Maurice N, Mondain M, Crampette L, Guerrier B, Intramuscular haemangioma of posterior neck musclesEur Arch Otorhinolaryngol 2001 258:28-30. [Google Scholar]
[5]. Kim DH, Hwang M, Kang YK, Kim IJ, Park YK, Intramuscular haemangioma mimicking myofascial pain syndrome: a case reportJ Korean Med Sci 2007 22:580-82. [Google Scholar]
[6]. Pekiner FN, Kodallı N, Horasan S, Haemangioma: Case Report of a lesion of the mid-face focusing upon imaging findingsJournal of Marmara University Institute of Health Sciences 2011 1(3):184-89. [Google Scholar]
[7]. Jain V, Bahri N, Parekh HP, Mody SS, Intramuscular heangioma of the masseter: erectile haemangiomaInternational Journal of Head and Neck Surgery 2011 2(3):169-71. [Google Scholar]
[8]. Shima F, Mihara K, Hachisuga S, Angioma in the paraspinal muscles complicated by spinal epidural haematomaJ Neurosurg 1982 57:274-77. [Google Scholar]
[9]. Afsar FS, Oziz E, Hamdioglu Y, Karasoy I, Uguz B, Intramuscular haemangioma of the masseter muscle in a 9-year-old girlActa Angiol 2007 13(1):42-46. [Google Scholar]
[10]. Hussain A, Mahmood H, Almusawy H, Moderate size infantile haemangioma of the neck –conservative or surgical treatment? : a case reportJournal of Medical Case Reports 2008 2:52 [Google Scholar]
[11]. Brown RA, Crichton K, Malouf GM, Intramuscular haemangioma of the thigh in a basketball playerBr J Sports Med 2004 38:346-48. [Google Scholar]
[12]. Cohen AJ, Youkey JR, Clagett GP, Huggins M, Nadalo L, d'Avis JC, Intramuscular HaemangiomaJAMA 1983 249(19):2680-82. [Google Scholar]
[13]. Vakilha M, Farhan F, Samiei F, Shariat S, Intramuscular Haemangioma of the forearm; Report of a caseIran J Radiat Res 2003 1(3):175-79. [Google Scholar]
[14]. Nurliza I, Kenali MS, Sani A, Intramuscular Haemangioma in the Head and NeckMed J Malaysia 2007 62(5):409-10. [Google Scholar]