Stress fractures (SFs) have recently been a matter of concern in military cadets undertaking basic training since it results in attrition as well as significant economic losses. Basically an over use injury, these fractures are a result of repeated application of stress lower than that required to fracture the bone in a single loading situation [1]. The activities involved in the diverse types of military training may put personnel at different injury risks. The most frequently reported cause of these fractures is repetitive weight-bearing activities such as running and marching, a recent increase in physical activity, beginning of a new activity or some other change in their routine can also result in increase of these fractures [2].
Symptom includes pain which increases on bearing weight and swelling. Typical findings include localized tenderness, swelling and erythema. Preliminary diagnosis of these fractures is through history assessment and clinical diagnosis. Radiological diagnosis provides a reliable confirmation of these fractures and site associated. SFs may heal completely, slowly or incompletely. Prevention, however difficult is the best approach for avoiding SFs. Treatment strategies includes early identification of the symptoms, early diagnosis, a sufficiently long training pause and in special cases consultation of experts in the field. Surgical treatment may be needed in some cases [2,3].
Beside the knowledge about the occurrence of these fractures and their effect on economy and loss of training hours, there are relatively few studies that provide actual incidence of these fractures in India. Information about the correct incidence is necessary to provide a basis for recommending future prevention strategies. The present study aimed at determining the incidence and type of SFs in Border Security Force cadets (BSF) recruited in Bangalore through clinical and radiological diagnosis.
Materials and Methods
In a prospective study of SFs, a group of 2000 BSF cadets training in Bangalore was selected and those presenting with symptoms were evaluated clinically and radiologically, appropriately managed and followed up every two weeks till fracture union. CT scans were performed only for femoral neck fractures. Only plain X-rays were taken for every patient as the digital facility was not available at our setup. All the participants in the study gave their informed consent and knew the objectives of the study. Any trainee having acute history of trauma was excluded from the study.
During their training, the recruits were reviewed by the doctor appointed at the BSF training campus. All the recruits were encouraged to report symptoms of possible SF, and all symptomatic recruits were referred to our hospital (Bangalore Medical College, Bangalore) for further management. Appropriate radiographs were taken. The time of fracture was considered to coincide with the earliest manifestation of pain in the affected limb. The cadets had free access to the medical staff as well as mandatory examinations every two weeks during training. All but 8 patients were treated conservatively; with initial period of immobilization with POP, rest, ice packs and analgesics, followed by muscle conditioning, mobilization and gradual re-induction into training programme. Period of management was decided according to the site and grade of SFs and radiological signs of union.
The SF was graded in to 4 groups based on the suggested clinic-radiological classification by Agarwal [4].
Grade I: Mild pain, periosteal reaction, tenderness, walks without pain.
Grade II: Severe pain, hair line crack of cortex, tenderness, and walk without support.
Grade III: Severe pain, partial thickness involvement of cortex, tenderness, walks with support.
Grade IV: Severe pain, tenderness, cannot walk/walks with difficulty even with support, full thickness of cortex involved.
Results
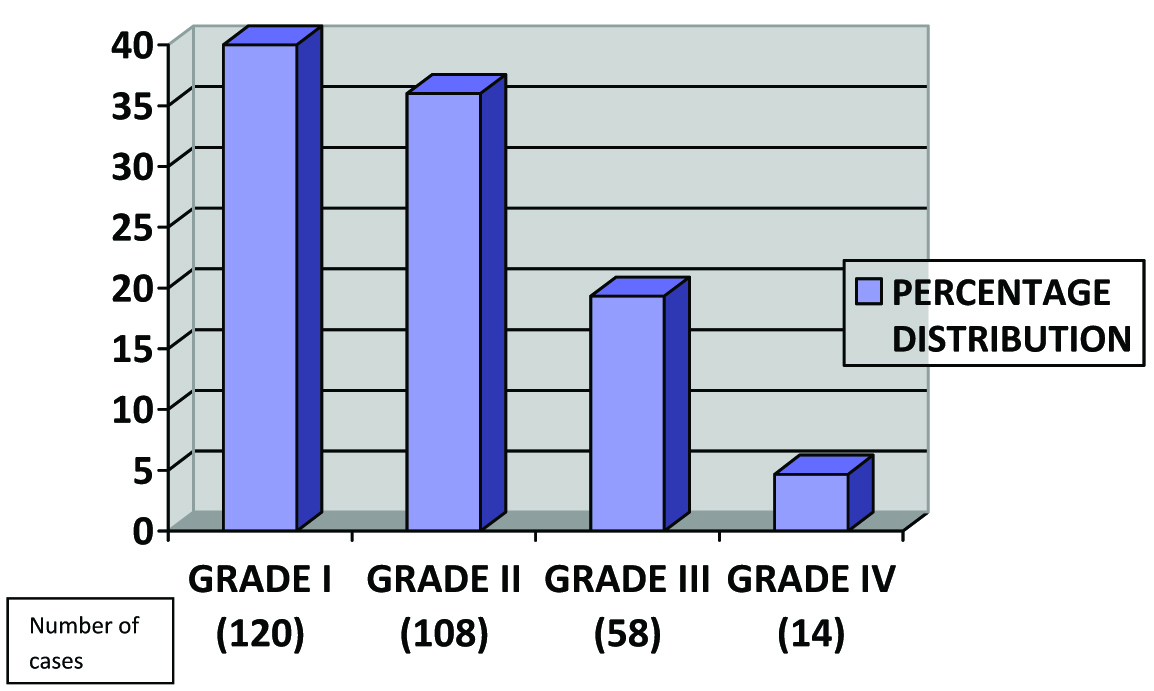
Three hundred and forty eight out of 2000 consecutive recruits had symptoms of SFs. On evaluation by radiography 300 recruits (15%) were diagnosed as having SFs. Out of 300 diagnosed with SF 120 (40%) were Grade I, 108 (36%) was Grade II, 58 (19.33%) were Grade III and 14 (4.67%) were Grade IV [Table/Fig-1].
Percentage distribution of stress fractures according to clinic-radiological classification by Agarwal
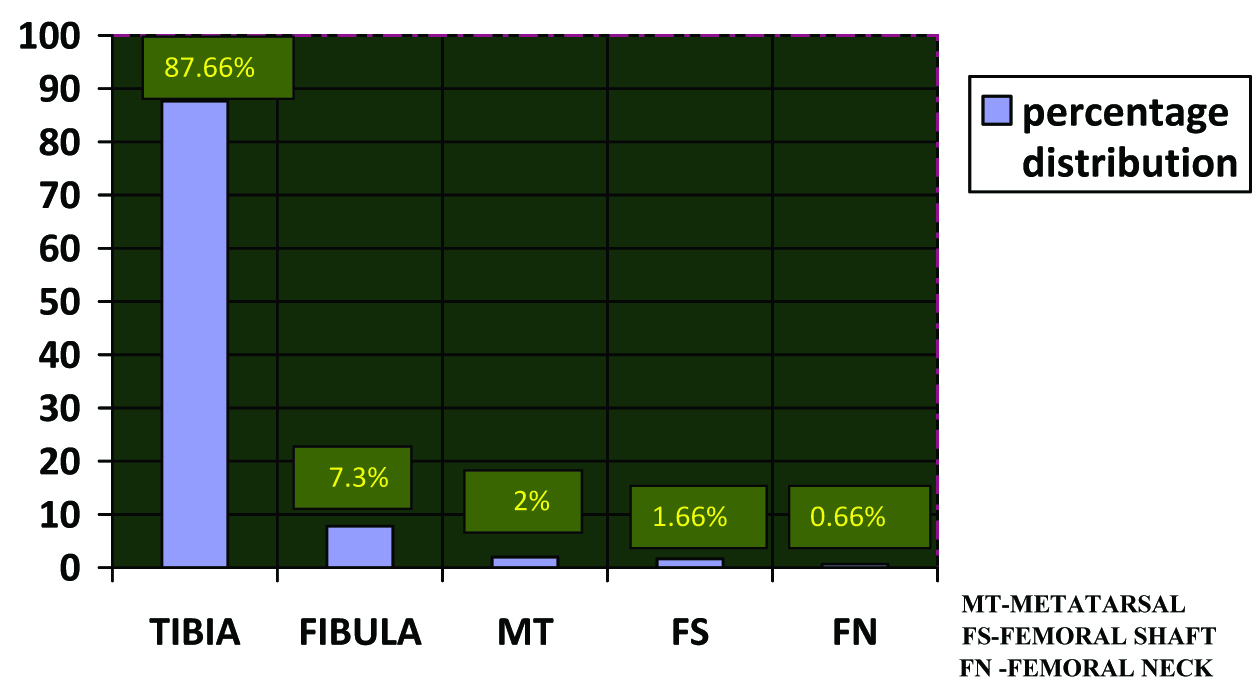
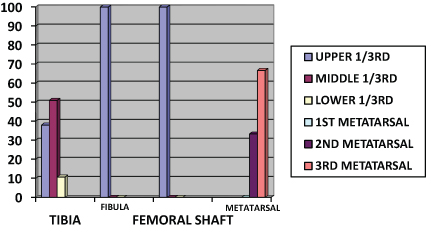
[Table/Fig-2] shows the number of fractures at each site. Highest number of injuries was found in the tibia (87.66%) [Table/Fig-3,4], followed by the fibula (7.3%), and metatarsals (2%). There were five femur injuries fractures including one bilateral femur proximal shaft (1.66%) [Table/Fig-5] and two neck of femur (0.66%) [Table/Fig-6,7,8]. Out of all the tibia fractures 38.02% fractures were at the proximal 1/3rd, 50.95% were at the middle 1/3rd junction and 10.7% were at the lower 1/3rd junction. All fibula fractures were at the proximal 1/3rd junction. Third metatarsal was most commonly involved (66.66%) followed by 2nd metartarsal (33.33 %). All femoral shaft fractures were in the proximal 1/3rd junction [Table/Fig-9].
Percentage distribution of stress fractures according to site involved
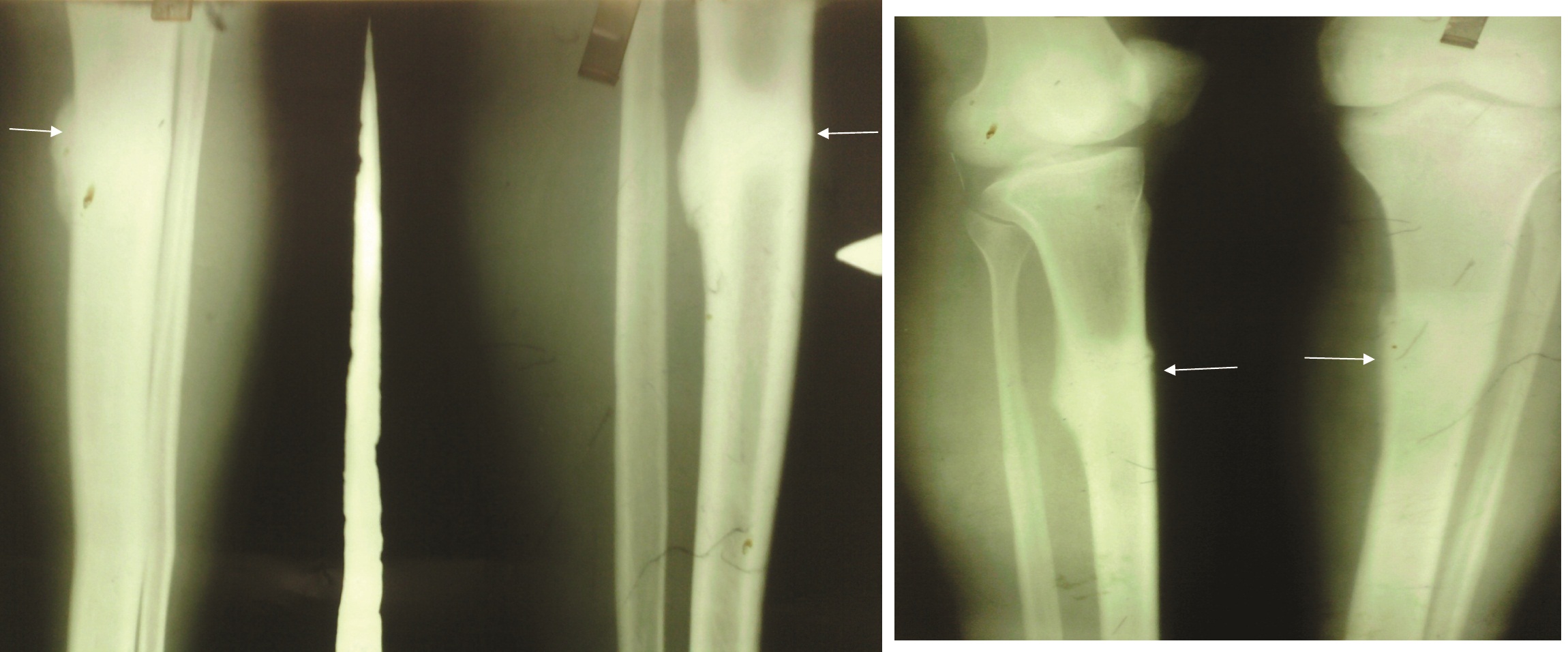
X-ray tibia fibula AP/LAT showing healed stress frature proximal 1/3rd
X-ray pelvis with both femur showing bilateral femoral stress fractures

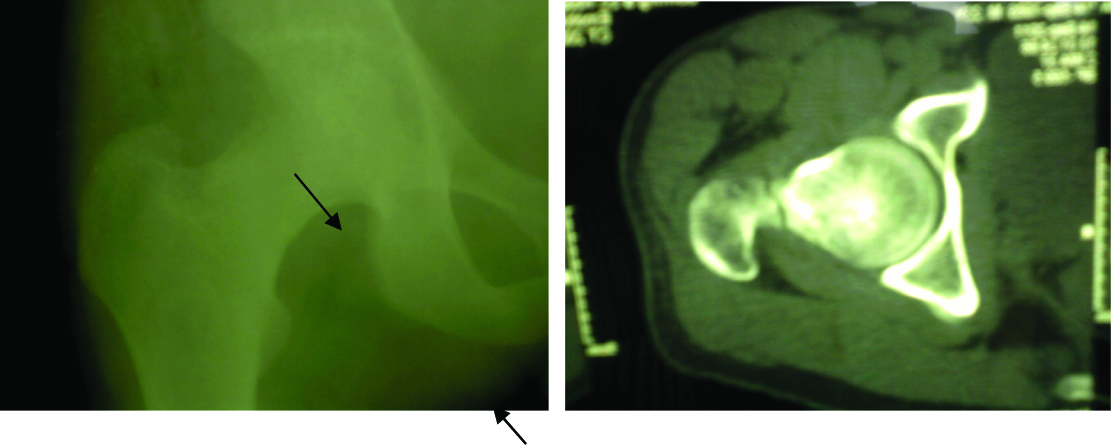
X-ray and ct right hip joint showing fracture neck femur
X-ray right hip of same patient, operated with Dynamic Hip Compression Screw

Percentage of site wise distribution of stress fractures
The incidence of SFs was more during their initial training period and reached maximum at 12 weeks of the training schedule. All the fractures were treated conservatively except 8 fractures (3 tibia,3 femur and 2 neck femur fractures) that were operated. All fractures healed uneventfully in an average period of 7 weeks. All cadets returned to full activity in an average period of 9 weeks.
Discussion
SF in military recruits is an overgrowing concern all over the world. The losses it confers in terms of SF morbidity, protracted recovery or termination of sporting pursuits are huge and needs immediate attention. The incidence and distribution of these SFs varies around the world. Data about the actual incidence from Indian military forces and precisely at what point in training do they occur is limited. The present study was performed to provide accurate answers to these questions, and the controlled circumstances of military service of Bangalore border service forces cadets provided a suitable group to study.
The incidence of SFs among military recruits has been reported to be around 5% amongst the US military recruits [5]. However, in India two studies by Agrawal PK and Dash N et al., reported high incidence of 11.4% and 7.04% in two different military training centres [4,6]. Apparently, the 15% incidence of SFs in our study far exceeds this figure or those reported from any previous study.
The significant higher incidence of SFs has been attributed to training with maximum stress on running, jumping, parade on hard ground, and gymnastics [7]. It can be also due to sudden increase in amount and intensity of physical activity along with repeated impact due to running on hard surface, improper technique and equipment [2,8]. Moreover, direct entry cadets partly due to their initial entry level fitness and partly not accustomed to the training regimens suffer a lot of impact on the bone.
Commonest site involved in our cases was tibia (87.66%) followed by fibula and metatarsal. The distribution of sites of SF in this study is similar to the study by Singh SC, et al., [9]. However, in contrast Alexander M Wood et al., reported metatarsals as the most common site for stress fracture [3].
The maximum occurrence of SF in our study was found at 12 weeks of training. However, in another study, the maximum occurrence of SF was found between the basic phase of training i.e. between nine weeks and 27 weeks [7].
In our study, SFs were confirmed on the basis of radiography. An additional bone scan was not performed in cases where radiographs were inconclusive as reported by Agrawal PK in his study [6]. It is thus likely that the incidence, we reported, could have been even higher if a bone scan or an additional scintigraphy was performed. Return to full activity has been reported at 12.2 weeks for metatarsal fractures to 21.1 weeks for tibial stress fractures [3]. In our case, all cadets returned to their full activity in an average period of nine weeks.
Conclusion
The study provides evidence that there is a high incidence of SF in military cadets that remains unreported otherwise. Additionally the possibility that some cadets do not report pain and continue strenuous exercise for fear of losing their term despite symptoms cannot be excluded and further add to the problem. The physician must therefore maintain a high index of suspicion of a SF. The cornerstone in avoiding SF is prevention. Education of trainees, trainers and instructors, modification in training procedures, use of better equipments can reduce occurrence of these fractures. Early reporting to hospital and treatment is also necessary as it can help in early return to full activity.