Introduction
SAH is a common brain disorders among all age groups, especially young people. SAH is famous Titanic death (32-67%) which can lead to hydrocephalus and vasospasm and subsequent neurological symptoms and morbidity. Furthermore approximately 20% of patients who survived are inactive and remain dependent [1,2].
The incidence of hydrocephalus after SAH has been reported to range from 6 to 67% in various studies and the occurrence time is varied from several days to years [3-9]. Cerebral vasospasm due to ischemia following SAH with a morbidity and mortality rate of 10% to 30%, there is in 70% of cases [10,11]. Vasospasm in patients with SAH is one of the major causes of death and disability among patients. Therefore prevention and treatment of cerebral vasospasm is critical in the management of SAH patients [1,12].
In hydrocephalus following SAH, cerebral ventricular is dilated and brain tissue due to ischemic damage. Placing the shunt for chronic hydrocephalus following SAH is associated with mortality rate of 7% to 9%, and the failure rate is high (43% per year and 85% at 10 years) [3]. In addition shunt procedures is associated with complications such as reoperation, subdural haemorrhage or intracranial haemorrhage, infections, seizure, cerebrospinal fluid (CSF) leakage and injuries to the lungs or abdomen[11,13]. FLT is a triangular-shaped hole that is created in the between the upper edge of chiasm and lower edge of anterior commissure with average size 8.25 mm and a minimum size of 2 mm. FLT cause the CSF release from the third ventricular and it facilitates the brain relaxation [13].
Recently,there are conflicting few reports of the effect of FLT on the incidence of the vasospasm and shunt-dependent hydrocephalus in SAH [3,13,14]. Understanding complex interactions between FLT, vasospasm and shunt-dependent hydrocephalus in SAH is poorly and insufficiently investigated. To the best of our knowledge, because the uncertainty of the efficacy of FLT and the lack of comprehensive studies in this area, the aim of this study was to assess the effect of FLT on the incidence of vasospasm and shunt-dependent hydrocephalus in ACoA aneurismal in patients with SAH, in Imam Hussein hospital, Tehran, IR, during the year 2001-2009.The study hypothesis was: FLT is effective on vasospasm and shunt-dependent hydrocephalus in ACoA aneurismal in patients with SAH.
Materials and Methods
This was a randomized double-blind clinical trial study. After getting written permission data from the Imam Hussein hospital, at the Shahid Beheshti University of Medical Sciences, Tehran, Iran of 50 patients with SAH by ACoA aneurismal rupture, were selected between September 2001 and December 2009. The sample size was calculated using the information obtained from a pilot study with 10 patients and following formula:
n= (z1-α/2+z1-α)2(2s2)/ d2 = 25
Z1-α/2= 1.96, z1-β= 0.84 (test power)
S (An estimate of the standard deviation of parameters in the groups that 1.39 were obtained in a pilot study).
d (The minimum of mean difference of parameters between groups that show significant difference and obtained 1.1).
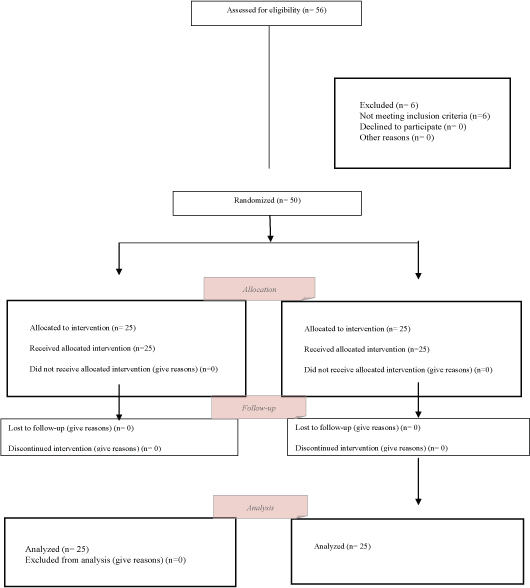
Due to limitation of statistical population, to increase the validity of study and achieve the sufficient sample size the sampling duration were raised. In a double-blind randomized trial Samples (1:1), with a simple random sampling assigned in two groups [Table/Fig-1]. Group I consisted of patients in whom FLT was performed (n=25) (FLT) and Group II consisted of patients in whom FLT was not carried out (n=25) (No FLT).
The inclusion criteria included all the patients that were due to Spontaneous SAH referred to the hospital Imam Hussein. The trialexclusion criteria were the haemorrhage due to elective surgery, SAH for reasons other than aneurism and unruptured aneurisms. Both groups were operated by a single neurosurgeon. The diagnosis of SAH was on brain Computed Tomography (CT) or Lumbar Puncture (LP) and the ruptured aneurismal on digital subtraction angiography was established. Severity of SAH was determined using the Hunt-Hess grade and Fisher grade.
In operation room all patients who had ACoA aneurismal ruptures, treated according to a standardized approach. Lumbar drainage or extra ventricular was not carried out prior to craniotomy. Brain inflation was managed by the opening and drainage of vessels. Ventriculostomy was performed when the brain inflation could not managed by mannitol or anesthetic techniques. Blood clots after aneurism surgery were carefully irrigated and sucked from the vessel. An incision in the lower midline in the LT, to prevent damage to the vascular space around the optic system was created and CSF was drainage through the aperture. To put ventricular-peritoneal shunts were decided by radiological and clinical criteria. The following variables were recorded for all patients: patient’s age, sex, Hunt-Hess grade[Table/Fig-2], Fisher grade [Table/Fig-3] and vasospasm, presence of hydrocephalus [Table/Fig-4] and incidences of shunt-dependent hydrocephalus. After surgery all the patients were managed using of hypervolemic therapy and calcium channel blocker to maintain appropriate haemodynamic condition.
Ethical Consideration: The study was approved by the Institutional Ethics Committee at the Shahid Beheshti University of Medical Sciences, Tehran, IR, and informed consent was obtained. (grant No: 275, date: 30/Jun/2010).
Statistical analysis
Collected data were analysed using SPSS, Ver.16 (SPSS Inc, Chicago, IL,USA). Descriptive statistics, Independent t-test, X2 test and Man-Whitney test were performed to analysing the results. p<0.05 was considered significant.
Results
Baseline characteristics of patients are shown in [Table/Fig-5]. None of the 50 enrolled patients was withdrawn for any reason. Mean age were (51.3 ± 14) in FLT group and (52.7 ± 13) in no FLT group. Women in both groups were the most frequent, 68% in FLT group and 76% in no FLT group (p>0.05).
There were no significant differences among groups in relation to demographic characteristics, neurological scale scores (Hunt-Hess grade) and the severity of the SAH (Fisher grade) (p>0.05). Patients were matched in baseline characteristics, Hunt-Hess grade and Fisher grade (p>0.05).
The rate of hydrocephalus on admission, in FLT and no FLT group were 24 and 16% respectively (p>0.05) [Table/Fig-5].
The shunt placement postoperatively were 16% in FLT group and 12% in no FLT group (p>0.05). The clinical vasospasm 20 and 24 % respectively in FLT and no FLT group (p> 0.05) [Table/Fig-6].
Discussion
Despite increasing our knowledge of surgery, over the past decade there has been no changes occurred in mortality and complications of subarachnoid haemorrhage. Spontaneous SAH is usually due to rupture of an intracranial aneurism that can cause morbidity and mortality or leading to complications such as vasospasm and hydrocephalus [15-19]. In this study, there was no significant differences between the FLT and without FLT group on the incidences of vasospasm and hydrocephalus in ACoA aneurismal ruptures in SAH patients which is consistent with previous studies by Kim et al., [3], Bae et al., [4], Dehdashti et al., [13], Komotar et al., [20], Komotar et al., [21] and contrast with some other studies by Komotar [14] and Tomasello [22].
Dehdashti et al., [13] in a study of Shunt-dependent hydrocephalus after rupture of intracranial aneurisms found that no significant difference in the rate of shunt-dependent hydrocephalus in both therapy groups. Komotar et al., [14] found FLT associated with a decreased incidence of shunt-dependent hydrocephalus of more than 80% after aneurismal SAH. In another study, Komotar et al.,[20] stated that in surgery with single-surgeon in contrast multisurgeon FLT not reduce the incidence of vasospasm or shunt-dependent hydrocephalus after aneurismal SAH. Kim et al., [3] in relation to influence of FLT on the occurrence of the shunt-dependent hydrocephalus in ACoA aneurismal ruptures found no significant correlation between the microsurgical fenestration and the rate of incidences of shunt-dependent hydrocephalus. In a systematic review by komotar et al., [21], revealed no significant association between reduced incidence of shunt-dependent hydrocephalus and FLT. Tomasello [22] stated favourable effect of FLT on CSF dynamics.
After aneurismal SAH, cerebral vasospasm is one of the most important factors to morbidity and mortality [23,24]. In other hand hydrocephalus that required a shunt operation is reported in about 20% of SAH [25]. Hydrocephalus according to the occurrence time is classified into three forms: the acute (0-3 days after haemorrhage), subacute (4-13 days after haemorrhage), and chronic (over the 14 days after haemorrhage). In chronic hydrocephalus, fibrosis and occlusion of the subarachnoid granules is effective in accelerating malabsorption and the communicating hydrocephalus.The FLT was carried out as a safe procedure by many surgeons but some complication such as decreased level of consciousness, hypothalamic injuries, transient confusion and memory loss were reported. For more decades, that FLT has been used for treatment of non-communicating hydrocephalus associated high intracranial pressure due to the obstructive pathologies in the midbrain and/or posterior cranial cavity. The mechanisms include CSF flow through the LT opening to an absorptive subarachnoid space and rapid transmission of the pulse pressure through a free communicating CSF space [3].
FLT should is protected for cases where the basal arachnoid cistern does not provide enough CSF release especially in that case of blocked basal cistern by adherent hematomas [3]. Fox and Sengupta [21] applied FLT for treatment of acute hydrocephalus and in order to avoid progress of chronic hydrocephalus [25]. In another study reported that FLT decreased the incidence of shunt-dependent hydrocephalus by more than 80% and reduced the morbidity and mortality associated the shunt operation [3].
According to studies older age, poor clinical grade on admission (Hunt-Hess, Fisher grade), the amount of the SAH, attendance of Primary intraventricular haemorrhage, hyponatremia, hypertension and the use of antifibrinolytic were all significant predictors of chronic hydrocephalus. Factors associated with development of shunt-dependent hydrocephalus included age, female, location of aneurism, poor neurological status and presence of initial intraventricular haemorrhage [4,26].
All patients enrolled in this study underwent surgery by a single surgeon that was the strengths of this study. Because of limited statically population, the time of study was prolonged and data collected from a single center which was the limitation of this study.
CONSORT diagram of participants in the clinical trail
| GRADE | NEUROLOGICAL CRITERIA | PERIOPERATI MORTALITY (%) |
|---|
| 0 | Incidental aneurysm , no subarachnoid haemorrhage | 0-2 |
| 1 | Asymptomatic or mild headache or maningismus | 0-5 |
| 2 | Moderate to severe headache, nuchal rigidity, no deficit other than cranial nerve palsy | 2-10 |
| 3 | Drowsiness ,confusion, mild focal deficit | 10-15 |
| 4 | Stupor, moderate to severe focal deficit, early decerebrate rigidity | 60-70 |
| 5 | Deep coma, decerebrate rigidity, moribund | 70-100 |
| GRADE | |
|---|
| 1 | Scan with no subarachnoid haemorrhage |
| 2 | Scan showing a thin layer of subarachnoid blood less than 1mm thick |
| 3 | Scan showing focal or diffuse thick subarachnoid blood more than 3 mm thick |
| 4 | Intracerebral or intraventricular blood with or without subarachnoid blood |
Measurement of hydrocephalus
| Age | Upper limit value |
|---|
| 30 or younger | 0.16 |
| 31-40 | 0.17 |
| 41-50 | 0.18 |
| 51-60 | 0.19 |
| 60-70 | 0.20 |
| 70-85 | 0.21 |
Characteristics of patients before of treatment
| Parameters | FLT FLT(n=25) | No FLT FLT (n=25) | p-value |
|---|
| Age , mean ± sd | 51.3± 14 | 52.7± 13 | p>0.05 |
| Sex, male: female (n %) | 8(32%): 17 (68%) | 6(24%):19(76%) | p>0.05 |
| Hydrocephalus on admission | 6 (24%) | 4 (16%) | p>0.05 |
| Hunt & Hess grade |
| ı/ıı | 16 (64%) | 16 (64%) | p>0.05 |
| ııı | 7 (28%) | 6 (24%) | p>0.05 |
| ıv | 2 (8%) | 3 (12%) | p>0.05 |
| V | 0.00 | 0.00 | |
| Fisher grade |
| 1/2 | 14 (56%) | 16 (64%) | p>0.05 |
| 3 | 9 (36%) | 8 (32%) | p>0.05 |
| 4 | 2 (8%) | 1 (4%) | p>0.05 |
Frequencies of postoperatively Complications according to group
| Parameters | FLT FLT(n=25) | No FLT FLT (n=25) | p-value |
|---|
| Shunt placement | 4 (16%) | 3 (12%) | p>0.05 |
| Conversion from acute hydrocephalus to shunt –dependent hydrocephalus | 2 (33%) | 2 (50%) | p>0.05 |
| Clinical vasospasm | 5 (20%) | 6(24%) | p>0.05 |
Conclusion
In conclusion, despite FLT can a safe method, there were not observed significant differences between group in relation to the effect of FLT on incidence of vasospasm and shunt-dependent hydrocephalus. This finding emphasizes the need for systematic evaluation of the affect of fenestration in this patient’s population with multisurgeon, multicentre and with greater sample size to disclose reality is suggested.
Acknowledgment
We thank Shahid Beheshti and Ilam University of Medical Sciences , participants, coordinators, and data reviewers who assisted in this study.
Authors’ contribution
Dr Hatefi in patients surgery, Dr Azhari, Dr Naebagaee and Dr Mohmmadi as supervisor and study design and Molouk Jaafarpour Contributed in literature review and the writing of article .
Funding/Support: This article was derived from PHD thesis in neurosurgery at the Shahid Beheshti University of Medical Sciences, Tehran, IR- Iran (grant No: 275, Date: 30/Jun/2010).
[1]. SM Ghodsi, N Mohebbi, S Naderi, M Anbarloie, A Aoude, SSH Pasdar, Comparative Efficacy of Meloxicam and Placebo in Vasospasm of Patients with Subarachnoid HaemorrhageIJPR. 2015 14(1):125 [Google Scholar]
[2]. J van Gijn, G Rinkel, Subarachnoid haemorrhage: diagnosis, causes and management.Brain. 2001 124(2):249-78. [Google Scholar]
[3]. JM Kim, JY Jeon, JH Kim, JH Cheong, KH Bak, CH Kim, Influence of lamina terminalis fenestration on the occurrence of the shunt-dependent hydrocephalus in anterior communicating artery aneurysmal subarachnoid haemorrhageJKMS. 2006 21(1):113-18. [Google Scholar]
[4]. I-S Bae, H-J Yi, K-S Choi, H-J Chun, Comparison of Incidence and Risk Factors for Shunt-dependent Hydrocephalus in Aneurysmal Subarachnoid Haemorrhage PatientsJ Cerebrovasc Endovasc Neurosurg 2014 16(2):78-84. [Google Scholar]
[5]. J Ding, Y Guo, H Tian, The influence of decompressive craniectomy on the development of hydrocephalus: a reviewArquivos de Neuro-Psiquiatria 2014 72(9):715-20. [Google Scholar]
[6]. R Rahme, AG Weil, M Sabbagh, R Moumdjian, A Bouthillier, MW Bojanowski, Decompressive craniectomy is not an independent risk factor for communicating hydrocephalus in patients with increased intracranial pressure.Neurosurgery. 2010 67(3):675-78. [Google Scholar]
[7]. S Honeybul, Complications of decompressive craniectomy for head injuryJournal of Clinical Neuroscience 2010 17(4):430-35. [Google Scholar]
[8]. S Honeybul, KM Ho, Incidence and risk factors for post-traumatic hydrocephalus following decompressive craniectomy for intractable intracranial hypertension and evacuation of mass lesionsJournal of Neuro Trauma. 2012 29(10):1872-78. [Google Scholar]
[9]. H-L Tian, T Xu, J Hu, Y-H Cui, H Chen, L-F Zhou, Risk factors related to hydrocephalus after traumatic subarachnoid haemorrhageSurgical Neurology 2008 69(3):241-46. [Google Scholar]
[10]. AP Carlson, H Yonas, Radiographic assessment of vasospasm after aneurysmal subarachnoid haemorrhage: the physiological perspectiveNeurological Research 2009 31(6):593-604. [Google Scholar]
[11]. JP Jeon, SH Sheen, Y-J Cho, Intravenous Flat-Detector Computed Tomography Angiography for Symptomatic Cerebral Vasospasm following Aneurysmal Subarachnoid Haemorrhage.The Scientific World Journal 2014 2014(315960) [Google Scholar]
[12]. KT Kreiter, D Copeland, GL Bernardini, JE Bates, S Peery, J Claassen, Predictors of cognitive dysfunction after subarachnoid haemorrhage.Stroke 2002 33(1):200-09. [Google Scholar]
[13]. AR Dehdashti, B Rilliet, DA Rufenacht, N de Tribolet, Shunt-dependent hydrocephalus after rupture of intracranial aneurysms: a prospective study of the influence of treatment modality.JNS. 2004 101(3):402-07. [Google Scholar]
[14]. RJ Komotar, A Olivi, D Rigamonti, RJ Tamargo, Microsurgical fenestration of the lamina terminalis reduces the incidence of shunt-dependent hydrocephalus after aneurysmal subarachnoid haemorrhage.Neurosurgery. 2002 51(6):1403-13. [Google Scholar]
[15]. J Konczalla, J Platz, P Schuss, H Vatter, V Seifert, E Güresir, Non-aneurysmal non-traumatic subarachnoid haemorrhage: patient characteristics, clinical outcome and prognostic factors based on a single-center experience in 125 patients.BMC Neurology 2014 14(1):140 [Google Scholar]
[16]. SK Gupta, R Gupta, VK Khosla, S Mohindra, R Chhabra, N Khandelwal, Nonaneurysmal nonperimesencephalic subarachnoid haemorrhage: is it a benign entity?Surgical Neurology 2009 71(5):566-71. [Google Scholar]
[17]. NA Bakker, RJ Groen, M Foumani, M Uyttenboogaart, OS Eshghi, JD Metzemaekers, Repeat digital subtraction angiography after a negative baseline assessment in nonperimesencephalic subarachnoid haemorrhage: a pooled data meta-analysis: A systematic reviewJNS. 2014 120(1):99-103. [Google Scholar]
[18]. JE Delgado Almandoz, BM Crandall, JL Fease, JM Scholz, RE Anderson, Y Kadkhodayan, Diagnostic yield of catheter angiography in patients with subarachnoid haemorrhage and negative initial noninvasive neurovascular examinationsAJNR. 2013 34(4):833-39. [Google Scholar]
[19]. A Tekiner, MB Yilmaz, E Polat, T Goker, MF Sargon, A Arat, The Therapeutic Value of Proanthocyanidin in Experimental Cerebral Vasospasm Following Subarachnoid Haemorrhage.Turk Neurosurg 2014 24(6):885-90. [Google Scholar]
[20]. RJ Komotar, DK Hahn, GH Kim, J Khandji, J Mocco, SA Mayer, The impact of microsurgical fenestration of the lamina terminalis on shunt‐dependent hydrocephalus and vasospasm after aneurismal subarachnoid haemorrhage.Neurosurgery. 2008 62(1):123-34. [Google Scholar]
[21]. RJ Komotar, DK Hahn, GH Kim, RM Starke, MC Garrett, MB Merkow, Efficacy of lamina terminalis fenestration in reducing shunt-dependent hydrocephalus following aneurysmal subarachnoid haemorrhage: a systematic review: Clinical ArticleJNS. 2009 111(1):147-54. [Google Scholar]
[22]. F Tomasello, D d’Avella, O de Divitiis, Does lamina terminalis fenestration reduce the incidence of chronic hydrocephalus after subarachnoid haemorrhage?Neurosurgery. 1999 45(4):827 [Google Scholar]
[23]. KT Kreiter, D Copeland, GL Bernardini, JE Bates, S Peery, J Claassen, Predictors of cognitive dysfunction after subarachnoid haemorrhageStroke. 2002 33:200-08. [Google Scholar]
[24]. J Claassen, GL Bernardini, K Kreiter, J Bates, YE Du, D Copeland, Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid haemorrhage: the Fisher scale revisited.Stroke. 2001 32:2012-20. [Google Scholar]
[25]. JJ Choi, HS Koh, JH Cho, SH Kim, JY Youm, SH Song, Clinical study on risk factors of hydrocephalus after aneurysmal subarachnoid haemorrhageJKNS. 2001 30(12):1375-80. [Google Scholar]
[26]. JG de Oliveira, J Beck, M Setzer, R Gerlach, H Vatter, V Seifert, Risk of Shunt‐dependent Hydrocephalus after Occlusion of Ruptured Intracranial Aneurysms by Surgical Clipping or Endovascular Coiling: A Single‐institution Series and Meta‐analysisNeurosurgery. 2007 61(5):924-34. [Google Scholar]